
Abstract
Background:
The disease trajectory of heart failure (HF), along with other organ failures, is still being elucidated. The trajectory is represented as a descending saw-tooth curve, indicating the frequent exacerbations and hospitalizations and slow progression to death. However, the clinical pattern of HF is no longer unique because of the definition of three distinct phenotypes, according to different values of ejection fraction (EF): HF with reduced EF (HFrEF), mildly reduced EF (HFmEF), and preserved EF (HFpEF). Patients with HFrEF have access to pharmacological and nonpharmacological treatments that have been shown to reduce mortality, unlike the other two classes for which no effective therapies are present. Therefore, their disease trajectories are markedly different.
Methods:
In this study, multiple new disease trajectories of HFrEF are being proposed, ranging from a complete and persistent recovery to rapid clinical deterioration and premature death. These new trajectories pose challenges to early implementation of palliative care (PC), as indicated in the guidelines.
Results:
From these considerations, we discuss how the improved prognosis of HFrEF because of effective treatment could paradoxically delay the initiation of early PC, especially with the insufficient palliative knowledge and training of cardiologists, who usually believe that PC is required only at the end of life.
Conclusions:
The novel therapeutic approaches for HF discussed in this study highlight the clinical specificity and peculiar needs of patients with HF. The changing model of disease trajectories of patients with HF will provide new opportunities for the early implementation of PC.
Introduction
Heart failure (HF) is a leading cause of death, morbidity, hospitalization, and symptom burden. 1 One of its main characteristics is its unpredictable prognosis. HF is currently divided into three phenotypes, based on ejection fraction (EF) values: HF with reduced EF (HFrEF)-(EF ≤ 40%), mildly reduced EF (HFmEF)-(EF 41%–49%), and preserved EF (HFpEF)-(EF ≥ 50%). 1
Traditionally, the disease trajectory of HF is depicted as a descending sawtooth curve (Fig. 1), corresponding to frequent exacerbations, which almost invariably lead to hospital admission.2,3 Deaths may occur suddenly, even in stable phases of the disease, and seldom unexpectedly or during an exacerbation causing progressive clinical deterioration. Moreover, comorbidities play a role in disease progression. 4
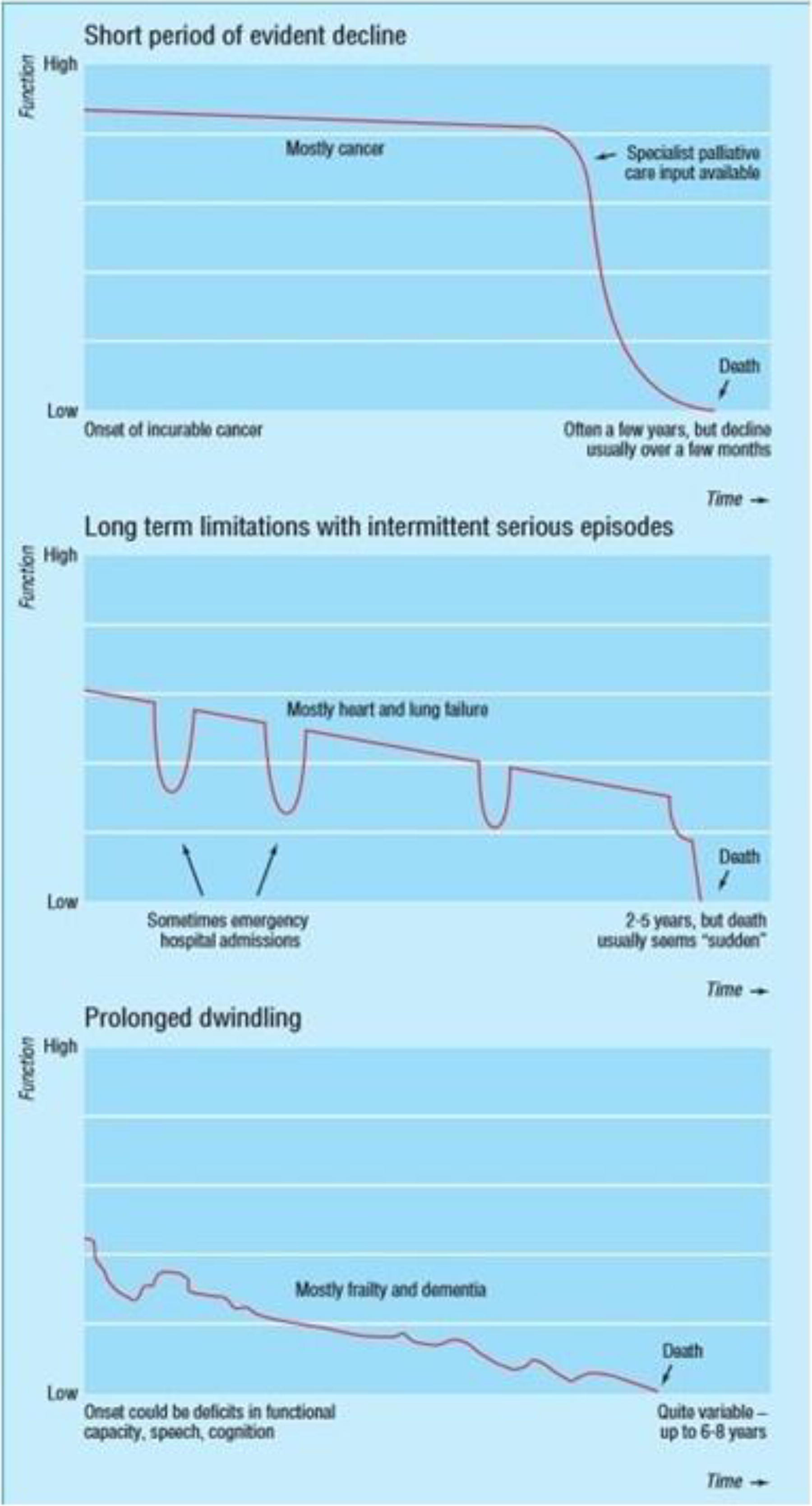
Illness trajectories. See the text for details. From Murray et al., 2 with permission.
Based on the guidelines and various HF-related studies,5,6 the clinical trajectory of patients with HF is similar to that of other organ failures such as chronic kidney disease (CKD) or chronic obstructive pulmonary disease (COPD).2,3 Therefore, in cases of organ failure, identifying the optimal time to initiate palliative care (PC) intervention is difficult because of the unstable pattern of the illness.
In the study by Murray et al., 2 two other disease trajectories are illustrated (Fig. 1). The first describes the cancer trajectory, featuring a relatively long period of stability, followed by a short period of decline, which rapidly leads to death. The decline is depicted as a “knee,” presenting a time in which the clinical conditions worsen and the PC needs substantially increase. However, the relatively long initial period of clinical stability allows the early identification of palliative needs and initiation of the discussion on the end-of-life care. The second trajectory describes what happens in older patients with neurological diseases, such as dementia, or more broadly, those with frailty. The curve typically presents a progressive dwindling decline in performance status, with a starting point that is already low. Death frequently follows an infection or a bone fracture, mainly femoral.
The functional status of HF on the “traditional” curve of disease trajectory is expressed as the New York Heart Association (NYHA) classes or Quality of Life (QoL) on the vertical axis and time from diagnosis to death on the horizontal axis. (Fig. 1)
Murray et al. have further described four “dimensional patterns” of needs (social, psychological, physical, and spiritual) with different behaviors. 3 These dimensional patterns show different trends, depending on various diseases: in organ failure, the physical, psychological, and social need curves follow the sawtooth pattern, whereas the spiritual need curve is dwindling. In patients with cancer, the physical and social need curves have the same morphology of clinical evolution, whereas the social and spiritual need curves display an undulatory trend. In patients with frailty or dementia, the physical need curve is dwindling, while the curves of the other trajectories are gradually declining.
These general trajectories may show distinct patterns depending on the cultural, social, and geographical characteristics. However, this “traditional” picture refers to a unique HF clinical pattern, a concept long outdated since the current HF classification was proposed and validated. 6 Patients with HFrEF demonstrate varying epidemiology, clinical picture, and characteristics compared with patients with HFmEF or HFpEF, even if their prognoses are similar. 7 Compared with patients with HFrEF, patients with HFpEF are older and are affected by a higher burden of symptoms and noncardiac comorbidities, such as CKD, COPD, anemia, diabetes, thyroid dysfunction, stroke, peripheral arterial disease, psychiatric illness, cancer, and frailty. 7 Consequently, they die more often of noncardiac causes, such as organ failure or infection. These differences indicate that patients with HFpEF may need more specific PC and a high-frequency multidisciplinary approach.
Older populations may require the involvement of geriatricians, social workers, and psychologists in determining the PC approach to tailor care for each patient’s individual needs. However, the disease trajectory and prognosis of patients with HFrEF are changing because of the recent pharmacological and nonpharmacological therapeutic approaches 6 and digital medicine, 8 which substantially improve the survival and QoL of patients with HFrEF. The unpredictability of the prognosis remains a challenge; however, it is becoming clearer recently.
We aim to explore the evolving disease trajectory and prognosis of patients with HF, particularly focusing on the impact of HF phenotypes and comorbidities on clinical outcomes. In addition, we seek to assess the influence of recent therapeutic advances on the prognosis and QoL of the patients and to address the challenges of predicting prognosis and tailoring PC interventions to individual patient needs, especially in older populations.
Available disease-modifying treatments
Recent advances in HFrEF treatment completely differ from those of HFmEF, HFpEF, or other organ failures. The “four pillars” therapy (1. angiotensin-converting enzyme inhibitors or sacubitril/valsartan, 2. beta-blockers, 3. mineralcorticoid receptor antagonists, and 4. sodium–glucose cotransporter 2 inhibitors [SGLT2i]) is currently the cornerstone of treatment, as it is associated with a lower risk of hospitalization and mortality6,9 (also of arrhythmic origin). 9 Therefore, the decreased mortality associated with the use of the four pillars of HFrEF therapy partially depends on lower sudden (mostly arrhythmic) cardiac death. 10
Cardiac implantable electronic devices (CIEDs), implantable cardioverter defibrillators (ICDs), and cardiac resynchronization therapy (CRT) are the secondary fundamental treatments for the primary prevention of sudden cardiac death (SCD) 11 and improvement of QoL and survival. 12
Mitral regurgitation (MR) is frequent in patients with HF and can occur isolated or associated with tricuspid regurgitation (TR).13,14 They both exhibit a high 1-year mortality.15,16 Transcatheter repair of MR demonstrated reduced hospitalization and mortality,17,18 whereas transcatheter repair of TR improved only the QoL. 19
In certain patients with diffuse coronary disease and reduced EF, not amenable to percutaneous intervention, aortocoronary bypass and surgical reconstruction are viable alternatives. 20 As destination therapy (DT), mechanical circulatory support using left ventricular assist devices (LVAD) can improve survival in patients for up to 73% at 24 months following an implant. 21 Patients with last-generation LVAD implants as a bridge to transplants have the same 2-year survival, similar to those with LVAD as DT (76.8%), and significant improvement in QoL, expressed as NYHA class. 22 The final treatment approach is a heart transplant, which has a 5-year survival of 70% and a 10-year survival of 52%. 23
Patients with HFmEF, and particularly those with HFpEF, cannot rely on treatments that reduce mortality, and only SGLT2i demonstrated lower hospitalization rates and improved QoL. 24 Therefore, the disease trajectories of HFmEF and HFpEF are similar to that of the “traditional” one. 25
Data from real-world settings
The aforementioned treatment approaches for patients with HFrEF are not often applied in clinical practice, particularly the four classes of guideline-directed medical therapy (GDMT),26,27 CRT, 28 and ICD implantation. 29
The four classes of GDMT are prescribed for less than 10% of patients, 27 despite the increased uptake of SGLT2i. 27
CRT implants are not often used in Europe, being indicated for 25%–47% of patients with class I indication. 30
ICD implants are rarely used for the primary prevention of SCD; in the Swedish Registry, they are only indicated for 15% of patients with class I indication. 29
The annual report from the Society of Thoracic Surgeons Interagency Registry for Mechanically Assisted Circulatory Support (Intermacs) included data for 27,314 patients receiving continuous-flow durable LVAD during 2012–2021. 31
The number of patients referred for LVAD therapy has recently increased; however, disease severity is also increasing, patient needs are mostly unmet, and referrals are usually delayed. 21
In the broadly available registry from the United States, during 1991–2019, the number of heart transplants increased by 62%, and 24% of patients on the waiting list died or were delisted because of clinical deterioration. In the same period, the 1-year waitlist survival increased significantly up to 70%, particularly in the last 3 years, where the median time to transplant was 104 days. However, >50% remained on the waiting list without receiving a transplant. 32
PC and patients with HF
In an American Heart Association (AHA) Scientific Statement, 33 reproduced by McIlvennan and Allen (Fig. 2), 34 the traditional disease trajectory has been associated with a PC curve, which starts at the incidence of HF and progressively increases parallel to disease-modifying therapies up to the advanced phase when the decision to choose between the LVAD implant/heart transplant or the end-of-life treatments needs to be made.

Disease trajectory of heart failure with associated types and intensities of available therapies and palliative care. See text for details. CHF: chronic heart failure; MCS: mechanical circulatory support. From McIlvennan and Allen, 34 with permission.
Despite the wide underutilization of therapies effective in reducing mortality and hospitalization, a desirable increase in their implementation is possible for HFrEF treatment.26,28,35 Therefore, the illness trajectory will change, transforming from the original Murray pattern to multiple and unpredictable patterns, each influenced by the various treatments. (Fig. 3).
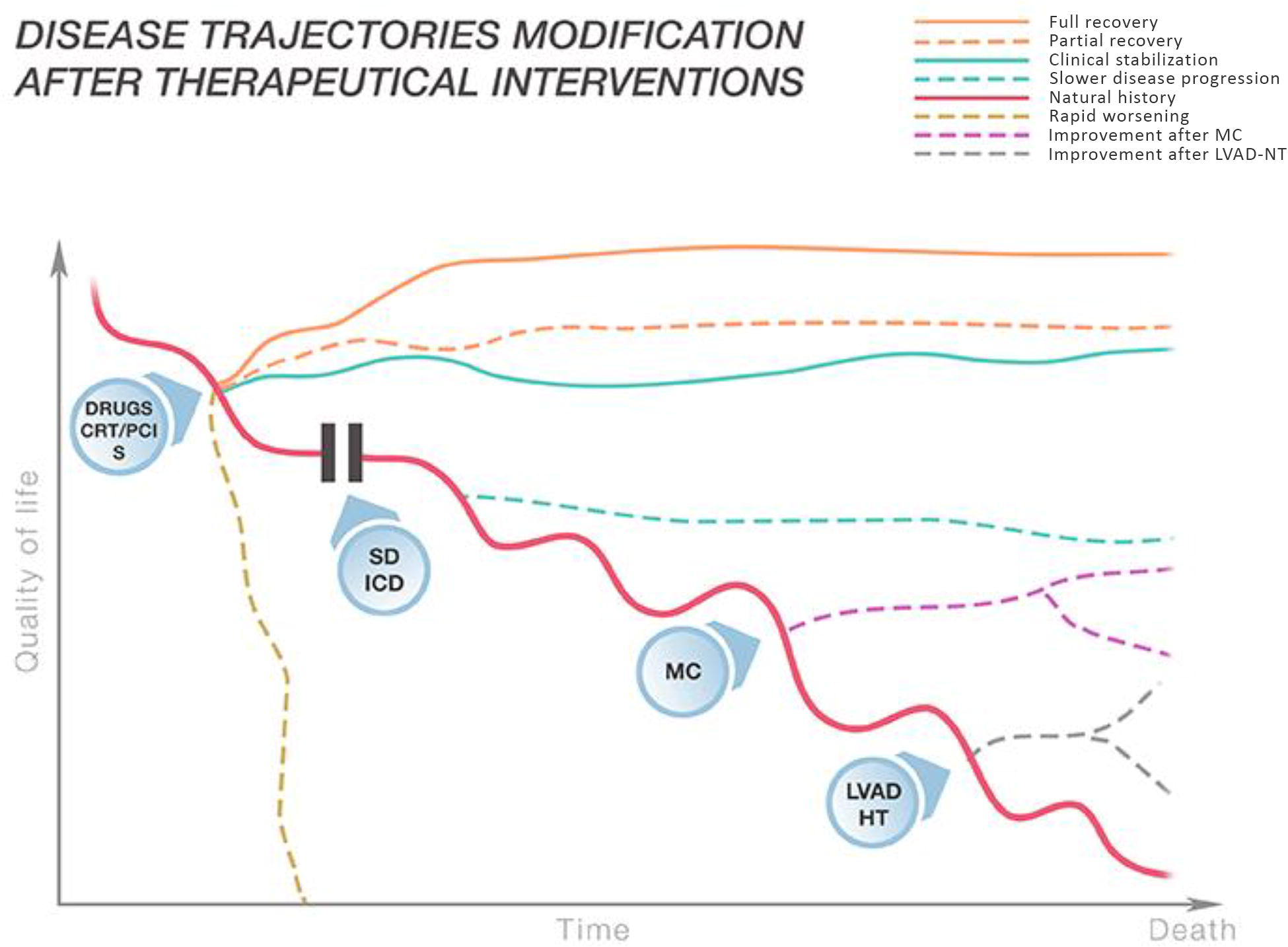
Different disease trajectories in heart failure and reduced ejection fraction related to different treatments. See text for details. CRT: cardiac resynchronization therapy; PCI: percutaneous coronary intervention; S: surgery; SD: sudden death; ICD: implantable cardioverter defibrillator; MC: MitraClip; LVAD: left ventricular assist device; HT: heart transplantation.
The inspiration to create this figure came from a similar figure proposed by Mullens et al. on optimizing the implementation of CRT in patients with HF. 28 The figure demonstrates that after the onset of HF, implementing the four GDMT classes in a short time (2–4 weeks), 36 coronary revascularization, and CRTP or CRTD implantation when indicated, may lead to various outcomes, from a complete and stable recovery to rapid deterioration and death. In certain cases of HF, ICD implantation is indicated to reduce the risk of sudden death. In the case of clinical worsening, transcatheter edge-to-edge mitral repair should be considered, especially in the presence of secondary severe MR. 18 In cases of advanced HF, LVAD implantation 21 (as a bridge to heart transplant or as DT) and heart transplant 22 may improve clinical status and prognosis. These different clinical pictures may influence the initiation of PC.
PC approach in HF
How will the PC approach be modified by these changes? And most importantly, what will be the optimal timing for initiating PC?
The World Health Organization (WHO) document on PC states: “Early delivery of palliative care reduces unnecessary hospital admissions and the use of health services. It prevents and relieves suffering through the early identification, correct assessment and treatment of pain and other problems, whether physical, psychosocial, or spiritual.” 37 This can be applied to patients with HF. 38
The American College of Cardiology/AHA guidelines 39 and the European Society of Cardiology–Heart Failure Association (ESC-HFA) position article 40 both define early PC in HF and state that PC should be integrated into the treatment of all patients with HF, whereas the European Society of Cardiology Guidelines (ESC) 8 recommend PC referral only in advanced HF and at the end of life.
However, in patients with HF, the practical meaning of “early” is not clear, despite recommendations that PC should be applied following the initial diagnosis of HF. 33
Overall, the number of patients who need PC differs substantially from the number of those who actually receive it, particularly in patients with cardiovascular diseases. PC referral is delayed for patients with HF, compared with cancer patients (12.4% vs. 30%, respectively). 41
Moreover, there are many barriers to the early implementation of PC in patients with HF, including:36,42
“Lack of awareness among policy-makers, health professionals, and the public about what palliative care is, and the benefits it can offer patients and health systems; cultural and social barriers, such as beliefs about death and dying; misconceptions about palliative care, such as that it is only for patients with cancer, or for the last weeks of life.”
39
The unpredictability of prognosis and the difficulty of discussing it with the patients and their families.
42
The stigma attached to the term “palliative” is greater among cardiologists than oncologists.
43
The lack of PC specialists. The HFA/ESC position statement on advanced HF states that PC should start only in advanced phases of disease and at the end of life.6,44
These barriers could paradoxically increase in the light of the expected potential improvement of prognosis. The different trajectories illustrated in Figure 3 outline the incoming difficulties of early PC. Cardiologists are not usually trained to initiate an early PC approach. 45 They believe that PC should be implemented at the end of life; the new and effective therapies may ultimately delay the initiation of PC. However, primary PC competence should be required for all healthcare professionals handling patients with severe diseases, 46 including clinical cardiologists.47,48 They should possess the knowledge and basic skills required for PC to assess and treat the most distressing symptoms (especially pain, anxiety, and depression), during the whole disease trajectory, starting at the early phases.
PC specialists can be involved in more advanced phases of illness or in the presence of refractory symptoms, when spiritual or existential difficulties arise, or during times when there is need of assistance in more complex medical decision-making processes, and in the resolution of conflicts between patient/family and the healthcare team.
Cardiologists should actively participate in shared decision making, process in-depth discussion on prognosis, treatment goals, and patient preferences, as well as implement advance directives related to end-of-life choices (including the need for cardiopulmonary resuscitation and policies on device therapy and discontinuation).39,48,49 Education on PC has been proposed to be included in the advanced HF and transplantation cardiology fellowship. 48
The lack of PC specialists further increases the delay in initiating treatment. This may be overcome by involving other adequately trained professionals, such as social workers and PC nurses. Another effective approach is the integration of PC specialists into the HF treatment team to take care of the patient at the early stages of the disease, enhancing the cultural contamination between cardiologists and PC specialists. This approach should be a permanent and early step in assembling the HF team, supporting the discussion on Advance Care Planning, end-of-life decisions, particularly about withholding/withdrawing life-sustaining treatments. 45
PC implementation in the early stages of HF may substantially improve the functional status and QoL of the patients, even those classified as NYHA functional class II.50,51 This is true for all patients with HF, including those with HFpEF, who represent about 50% of all patients. 7 However, only 5% of patients with HFrEF and 4% of patients with HFmEF and HFpEF receive PC annually. 52 Patients with HFrEF receive PC 6 weeks sooner than patients with HFmEF and HFpEF at 5 years of follow-up. 53
In this series, time from PC consultation to death was 4.80 months for patients with HFrEF, 4.95 months for patients with HFmEF, and 5.02 months for patients with HFpEF. 52 Therefore, the new different trajectories, shown in the Figure 3, do not change the need for the early implementation of PC at the point where disease trajectories begin to diverge. However, involving and improving the competency of cardiologists in primary PC would be a new and valuable opportunity to handle patients with HF holistically.
Unlike the former single HF trajectory, the novel multiple HF trajectories will influence various PC approaches for patients with HF. Following initial evaluation, a personalized PC program will be developed, which will be modified over time according to the clinical and psychological needs of each patient.
Unlike what is presented in Figure 2, the new proposed multiple patterns of the disease (Fig. 3), because of the full implementation of GDMT and nonpharmacological treatments, make personalization of PC possible and enable its modulation based on the progression of HF, following the different clinical trajectories. This approach can be adapted to all four components of Murray’s trajectory, the social, psychological, physical, and spiritual trajectories. 3
Recently, Zhang et al. analyzed the different and multiple trajectories of patients with acute HF at different times after discharge (38.9% with HFrEF). 52 They described six different individual trajectories, from “persistently good” to “persistently poor,” based on the Kansas City Cardiomyopathy Questionnaire-12. The trajectory at 1 year after discharge predicts the survival at 3 years after discharge. Various factors determine the poor survival at 1 year after discharge: advanced age, multiple socioeconomic risk factors, chronic HF, higher levels of N-terminal pro-brain natriuretic peptide at admission, depression, cognitive impairment, and each additional HF rehospitalization. Zhang et al. included patients with all HF phenotypes, including reduced, mildly reduced, and preserved EF. However, only patients with HFrEF may highly benefit from the aforementioned therapeutic approaches, compared with patients with HFmEF and HFpEF, for whom only SGLT2i may reduce hospitalization and improve QoL without affecting mortality.
Early palliative intervention could reduce HF transitions, in particular frequent hospitalization, and invasive procedures, such as mechanical ventilation or CIED implantation and improves QoL. 54 Therefore, the quality of care improves, hospice use increases, the older patients may receive increased home care, and the social and economic costs decrease. 54
Conclusions
The novel therapeutic approaches for HF discussed in this study highlight the clinical specificity and peculiar needs of patients with HF. The changing model of disease trajectories of patients with HF provides opportunities for the early implementation of PC.
Palliative intervention should not be limited to end-of-life care, and the barriers to its implementation should be overcome through strong communication between PC specialists and cardiologists and the development of specific PC programs during cardiology fellowships. 49 PC requires further diversification for type, quality, and frequency of intervention, with particular attention to social, physical, psychological, and spiritual challenges.
Acknowledgments
The authors would like to thank Editage (www.editage.com) for English language editing and Lorenzo Donati for graphical assistance.