
Abstract
Background:
Despite the global acceptance of palliative sedation, China’s engagement in this field remains comparatively restricted. There exists a scarcity of information regarding the attitudes and experiences of hospice nurses concerning palliative sedation.
Objectives:
This survey aimed at investigating the attitudes of Chinese hospice nurses toward palliative sedation, as well as their practices in palliative sedation.
Design:
A cross-sectional descriptive study.
Setting/Subjects:
In 2023, the survey on palliative sedation was introduced during the opening ceremony of the largest National Symposium on New Advances in Hospice Nursing in China. Subsequently, the study questionnaire was disseminated through email to a cohort of 806 hospice nurses attending the conference.
Measurements/Results:
The statistical analysis was based on 641 valid responses. Among them, 508 had no experience with palliative sedation, while only 133 had such experience. Around 92.5% of hospice nurses with experience in palliative sedation agreed with the physician’s instructions to begin palliative sedation. Nurses were present at the start of sedation in nearly all cases (97.0%), and most doctors (79.7%) and family members (82.0%) were also present. However, 8.3% of them perceived that there was no difference between palliative sedation and euthanasia. Furthermore, 13.5% of participants believed that the purpose of palliative sedation was to hasten death.
Conclusions:
Hospice nurses play a crucial role in the process of palliative sedation, yet they also face significant challenges. It suggests that there is an urgent need in China for the development of consensus or guidelines for palliative sedation to clarify the roles of team members, including hospice nurses.
Key Message
This cross-sectional descriptive study describes the attitudes and experiences of hospice nurses regarding palliative sedation in China. The results indicate that 92.5% of hospice nurses with experience in palliative sedation agreed with the physician’s instructions to begin palliative sedation and they play a crucial role in the process of palliative sedation.
Introduction
Palliative sedation is a measure of last resort used at the end of life to relieve severe and refractory symptoms. It involves administering sedatives to reduce patients’ level of consciousness and thereby alleviate their suffering. 1 In the literature, the prevalence of palliative sedation varies, possibly due to a lack of reliable definitions, variations in settings, and the high heterogeneity of patients involved in the studies. Overall, the literature data indicate that approximately 25%–33% of patients receiving hospice care require some form of palliative sedation. 2
In accordance with the definition of the World Health Organization (WHO), a team approach should be utilized to address the needs of patients and their families in hospice care. 3 Particularly, when preparing to implement contentious treatments such as palliative sedation,4,5 a team approach is of utmost importance. Nonetheless, in the majority of international studies, the focus of palliative sedation has predominantly centered on the practices and attitudes of physicians.6–8 Conversely, there have been only a few studies exploring the perspectives of hospice nurses until now.
Research findings indicate that, it is noteworthy nurses routinely play an integral role in the process of palliative sedation, encompassing the evaluation of the patients’ distressing symptoms and the selection of medications and administration routes, as well as the assessment of patients’ responses to palliative sedation.9,10 When they participate as members of a team, their role transforms from supporting physicians and patients to actively performing sedation. 11 However, other studies found that nurses, more frequently than physicians, reported the use of palliative sedation with the intention of hastening a patient’s death.12,13 In addition, a proportion of nurses (15%) reported experiencing emotional burden when administering palliative sedation to patients with advanced cancer. 14
Taken together, these studies underscore the important role that hospice nurses assume in palliative sedation and highlight the potential stress they may encounter. Based on these findings, the development of consensus or guidelines specifically tailored for hospice nurses engaged in palliative sedation could enhance their practices, ultimately contributing to an improved overall quality of patient care.11,15
While palliative sedation has gained widespread acceptance in the world, China’s experience in this domain remains relatively limited. Consequently, the principal aim of this research is to examine the attitudes of Chinese hospice nurses toward palliative sedation, as well as to explore their experiences and practices within the realm of palliative sedation.
Method
Design
A cross-sectional descriptive study was performed in 2023 using a web-based structured questionnaire.
Study population
The study aimed to assess the attitudes and experiences of Chinese hospice nurses involved in palliative sedation. However, determining the exact number of hospice nurses engaged in palliative sedation was challenging due to the unavailability of a comprehensive database with contact information for hospice nurses in China. Consequently, random sampling was not feasible. The Hospice Committee of the Chinese Nursing Association, as an authoritative academic organization for hospice nurses, annually hosts the largest National Symposium on New Advances in Hospice Nursing. This symposium provides a crucial platform for exploring the development of hospice care.
In 2023, before this conference, we contacted the chairmen of hospice committees in each province of China. Representatives from each province were appointed to participate in this significant meeting. Given that the participating nurses represented various hospice organizations from different hospitals across the country, they were considered representative of the broader population. During the opening ceremony of the conference, the study was introduced. Ultimately, the study questionnaire was disseminated through email to a cohort of 806 hospice nurses attending the conference.
Survey development and data collection
Drawing upon insights derived from both literature analysis and clinical experiences in palliative sedation, a web-based structured questionnaire was developed. A panel of leading experts in palliative sedation, encompassing an ethicist and a medical sociologist, as well as two physicians and two nurses, meticulously reviewed the initial drafts of the questionnaire. Three revision rounds were performed to ensure the applicability and completeness of the questionnaire. When the items were ready, the questionnaire was pilot tested with a cohort of 50 hospice nurses, who were asked to evaluate its clarity of terms, length, and specificity. After the pilot test, a revised version of the questionnaire was developed, and subjected to a second review by the expert panel.
The questionnaire was divided into two sections, comprising a total of 71 items (Supplementary Data S1). The first section, consisting of 19 items, was designed to collect baseline data from hospice nurses participating in the survey, including inquiries about their experience with palliative sedation. If a hospice nurse lacked such experience, the questionnaire concluded for that participant.
Conversely, if the nurse had experience in palliative sedation, they proceeded to complete the second section of the questionnaire. The data in this section are collected concerning the most recent patient nursed by the hospice nurse during the process of sedation. This includes assessment and indications, decision-making, drug selection, titration, and monitoring, as well as ethical issues. Questions were posed in a neutral manner. The majority of questions had dichotomous response options (yes or no, supplemented with “I don’t know”). On average, respondents are expected to allocate approximately 5 to 10 minutes for the completion of this questionnaire.
The data collection took place between July and September 2023. Two research assistants were responsible for downloading and checking the questionnaire data from the web. Questionnaires with up to 10% invalid entries were excluded.
Ethical considerations
This study received approval from the Institutional Review Board of Beijing Tsinghua Changgung Hospital (No. 23224-4-01). Written informed consent was waived due to the anonymous nature of the data collection process. Participants’ submission of the survey questionnaire was considered to be their informed consent.
Statistical analysis
Continuous variables were expressed as mean ± SD (x ± s) OR medians (25th to 75th interquartile range). Differences between groups were analyzed by Student t-test method. Categorical variables were described as percentages and analyzed using chi-square (χ2) test or Fisher’s exact test, as indicated. Univariate and multivariate logistic regression analyses were employed to explore the factors associated with the experience of palliative sedation. The p value reported was two-sided and value of <0.05 was considered statistically significant. All the analyses were performed with the statistical software packages R 4.2.1(http://www.R-project.org, The R Foundation) and Free Statistics software versions 1.9.
Results
Characteristics of participants
The characteristics of the participating hospice nurses are presented in Table 1. A total of 641 hospice nurses filled out the questionnaire, resulting in a response rate of 79.5%. Analyses were conducted based on participants with less than 10% missing data (n = 641) (Supplementary Table S1).
Characteristics of Participants
To systematically depict China’s socioeconomic development across different regions, the country is divided into four main economic regions: Eastern, Central, Western, and Northeastern. Eastern China leads in national economic contribution, accounting for over half of the total economy, closely followed by the Central region, with Western and Northeastern China trailing behind.
In China, hospitals are the primary types of medical institutions. They are classified into three levels according to the “Hospital Grading Management Standards,” with level 3 being the highest.
Of the 641 hospice nurses participating in the survey, 508 had no experience with palliative sedation, while only 133 had such experience. The participants were predominantly female, with an average age of 35.9 ± 7.4 years. Eastern China, recognized for its economic prowess, had the largest number of participants. In addition, over half of the participants were affiliated with tertiary hospitals. Multivariate logistic regression analysis showed that years of experience in hospice (OR = 1.08, 95% CI [1.02, 1.14], p < 0.05), learning of guidelines on palliative sedation (OR = 2.36, 95% CI [1.31, 4.27], p < 0.05), and participation in relevant training programs (OR = 2.35, 95% CI [1.31, 4.21], p < 0.05) are associated with the experience in palliative sedation (Supplementary Table S2).
Assessment and indications
Table 2 outlines the basic characteristics of 133 patients who received palliative sedation. Among these patients, 92.6% were in the terminal stage of cancer, and 69.9% of them had experienced refractory symptoms before the initiation of palliative sedation. Figure 1 provides a clear representation of indications for palliative sedation, with the top three being pain (48.1%), existential distress (18%), and delirium (8.3%).

Main refractory symptoms requiring sedation in 133 sedated patients in the study.
Assessment and Indications
Missing cases for age, n = 82.
Missing cases for diagnosis, n = 6.
Decision-making
Table 3 contains information concerning the decision-making process for palliative sedation. According to the information from participants, among the 133 cases of palliative sedation, 42.1% were initially proposed by physicians, 24.8% were suggested by family members, 15.0% were initiated by patients themselves, and 8.3% were suggested by nurses. A total of 70.7% of nurses were involved in discussions regarding the initiation of palliative sedation, with 92.5% of them concurring with the physician’s criteria for palliative sedation. Furthermore, within the 133 cases, 54.1% of patients requested hastened death, and 39.8% of patients engaged in discussions about euthanasia with nurses.
Decision-Making
Drug selection, titration, and monitoring
Figure 2 depicts the drug selection process during palliative sedation, with 69.9% of patients receiving opioids, indicating the highest proportion. An analysis of the reasons for using opioids revealed that 80.50% of cases utilized opioids for pain relief, 14.5% for sedation, and 4.5% to alleviate respiratory distress symptoms (Table 4).
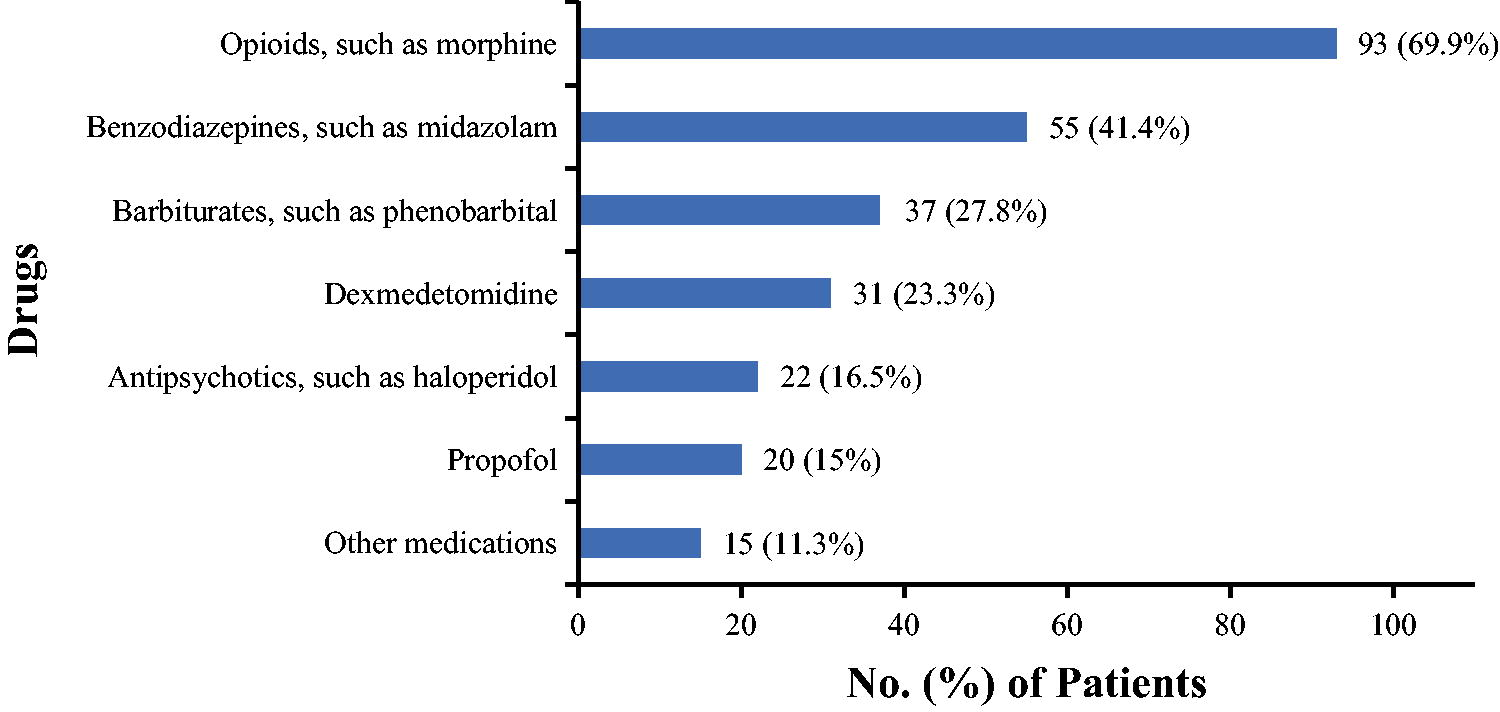
Sedative drugs administered to 133 patients in the study.
Drug Selection, Titration and Monitoring
Missing cases for “What is the interval between between the decision to use palliative sedation and the start of sedation (in hours),” n = 5.
Missing cases for “How long did it take to achieve the desired level of sedation after initiating palliative sedation (in hours),” n = 6.
Missing cases for “What was the duration between the initiation of palliative sedation and the patient's death (in hours),” n = 18.
At the onset of sedation, nurses were present in nearly all cases (97.0%), and most physicians (79.7%) and family members (82.0%) were also present. In 74.4% of cases, doctors remained present until the desired level of sedation was achieved. A significant majority (94.0%) of participants believed that both physicians and nurses should be responsible for monitoring the depth of sedation, while only 6% of respondents believed it should be the sole responsibility of either physicians or nurses.
Refractory symptoms were effectively managed in 91.7% of cases, with a median time of 2.0 hours (range, 1.0–3.0) from the initiation of sedation to reaching the desired sedation level. The majority of respondents, comprising 85%, reported a perception of a high quality of patients’ death, while 90.3% of family members conveyed satisfaction with the procedure of palliative sedation.
Ethical issues
Table 5 outlines the ethical perspectives of participants concerning palliative sedation. Although 86.5% of participants maintained that palliative sedation was different from euthanasia, 8.3% of them perceived that there was no difference between palliative sedation and euthanasia. Furthermore, approximately 13.5% of participants believed that the primary objective of palliative sedation was to hasten death.
Ethical Issues
Discussion
Our research findings indicate that, while only a minority of hospice nurses in China possess experience in palliative sedation, they play a significant role in various phases of implementing palliative sedation. At the same time, they may also experience pressures during this process.
Assessment and indications
The previous articles have reported the main indications for palliative sedation.16–18 According to a systematic review by Maltoni et al., delirium (54%) stands out as the most prevalent indication among patients undergoing palliative sedation, followed by dyspnea (30%), existential distress (19%), and pain (17%) as other refractory symptoms in descending order. 16 Nevertheless, our study reveals that among patients undergoing palliative sedation, the foremost three refractory symptoms comprise pain (48.1%), existential distress (18%), and delirium (8.3%).
It is evident that substantial variability exists in the occurrence of pain and delirium, potentially linked to inadequate utilization of opioids in our country and the challenge of distinguishing delirium from agitation due to inadequate pain relief. 19 Moreover, our study, consistent with the aforementioned research, recognizes existential distress as one of the indications for palliative sedation. 20 Notably, both the 2009 EAPC guidelines and the 2024 Revised EAPC recommended framework also assert that palliative sedation can be judiciously employed for terminally ill patients with existential distress.21,22
Decision-making
In most instances, hospice nurses perceive themselves as providing support in the decision-making process rather than taking an active role. Among the 133 palliative sedation cases examined in this study, only 8.3% were suggested by nurses. A study conducted by Arevalo et al. indicated that only 16.16% of nurses were the first to propose the use of palliative sedation. 11 Another study by Inghelbrecht et al. in 2011 found that nurses participated in shared decision-making with physicians in 23% of cases. 12 Variations in nurses’ participation in shared decision-making across different countries and studies highlight potential discrepancies in the development of hospice care, indicating substantial opportunities for improvement in China.
Regarding euthanasia, nurses generally reported that these discussions were initiated by the patients, particularly in hospital settings. In our study, 54.1% of patients requested hastened death, and 39.8% of patients discussed euthanasia with nurses. A study by Arevalo et al. found that 55.17% of patients discussed euthanasia with nurses. 11 In this situation, most nurses believed that patients should receive adequate palliative care before considering euthanasia. 23
Drug selection, titration, and monitoring
In the field of palliative sedation, most guidelines and articles recommend the use of midazolam as the primary sedative.1,17,21 A systematic review conducted by Bodnar et al. revealed that up to 70% of drugs utilized in palliative sedation were midazolam, owing to its rapid onset, short peak time, and an effectiveness rate ranging from 83% to 87%. 24 However, in our study, 69.9% of patients were administered opioids, followed by midazolam. This might be attributed to the prior use of opioids for pain or respiratory distress before initiating palliative sedation.
In various studies, the presence of doctors and nurses during the process of palliative sedation differs. According to this study, 79.7% of doctors were present after the initiation of sedation. Furthermore, 74.4% of them remained present until the desired level of sedation was achieved. This closely aligns with the findings of a study by Swart et al. 25 However, two other surveys targeting nurses yielded different results compared to our study.
Arevalo et al.’s research suggested that at the beginning of sedation, the presence of doctors was 45.22%, and when the desired sedation level was reached, only 11.05% of doctors were present. 11 Brinkkemper et al.’s study showed that at the beginning of sedation, the presence of doctors was 62.4%, and when the desired sedation level was achieved, 20.7% of doctors were present. 26 These disparities could stem from the diverse practices in hospice care worldwide, which include differences in teamwork, protocols for palliative sedation, and nursing responsibilities across different regions.
Ethical issues
While palliative sedation is widely accepted in the field of hospice care, 27 it remains a contentious subject within the realms of law, clinical practice, and ethics.5,28–31
Different hospice nurses hold varying perspectives on palliative sedation. In some studies, nurses did not consider palliative sedation to hasten death, as its primary goal is to alleviate intolerable suffering rather than shorten a patient's life.32,33
Nonetheless, in two Belgian studies, some nurses believed that palliative sedation could accelerate death.12,34 Consistent with the findings of these two studies, our study reveals that 13.5% of participants believed that the purpose of palliative sedation is to hasten death, and 8.3% felt that there was no distinction between palliative sedation and euthanasia. This indicates that hospice nurses may bear emotional burdens during palliative sedation, 14 which may place them in ethical dilemmas, 35 thereby impacting the implementation of palliative sedation. Further research is necessary to ascertain if other team members encounter comparable pressures.
Study limitations
Our study has some limitations. First, due to the absence of a comprehensive database containing contact information for hospice nurses in China, random sampling was not feasible. However, since the participants in this research came from various hospice organizations across the country, it is considered that the participants are still representative. Second, this research focused only on the attitudes and practices of nurses regarding palliative sedation. A more comprehensive picture of the practice of palliative sedation could be obtained comparing views of other health care professionals involved in palliative sedation. Third, we observed that there are five variables with missing values, with the highest missing rate at 61.7%. This phenomenon can be attributed to these variables being optional questions, allowing respondents the choice to either answer or skip them.
Conclusion
Hospice nurses play a crucial role in the process of palliative sedation, yet they also face significant challenges. It suggests that there is an urgent need in China for the development of consensus or guidelines for palliative sedation to clarify the roles of team members, including hospice nurses.
Footnotes
Acknowledgments
The authors thank all the nurses who participated in the study and the contact persons for their contributions to this study. The authors thank the Free Statistics team for providing technical assistance and valuable tools for data analysis and visualization. Furthermore, the authors thank Dr. Liu Jie (People’s Liberation Army of China General Hospital, Beijing, China) for helping in this revision.
Authors’ Contributions
Y.F. and G.J.L. were equally leading in conceiving the project. M.M.C. and H.Y.A. performed the data collection and data analysis. M.M.C. was responsible for the drafting of the article. Y.F. and G.J.L. supervised the study and made critical revisions to the article for important intellectual content. All authors agreed on the final article, and had made substantial contributions in all phases of the research process.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.