
Abstract

Dear Editor:
Hospice care has expanded greatly since the start of the Medicare hospice benefit in the early 1980s. 1 Admission diagnoses have expanded beyond cancer to include a constellation of conditions including dementia. Hospice care still suffers from late referrals. 2 It is difficult to meet the goals of interdisciplinary care of the patient and family, addressing physical, psychological, spiritual, and social suffering, if the patient dies within several days of admission.
A physician must refer an appropriate patient to hospice, certifying that the patient has a life expectancy of six months or less if the condition follows an expected trajectory without aggressive medical interventions (such as hospitalization) and that the patient chooses to forgo those interventions. Many physicians are reluctant to suggest to a patient that hospice care is an option. There is a myriad of reasons why that might be so, but I believe ignorance of the totality of hospice care is part of the problem. I believe that a change in nomenclature could help address this problem. I propose that hospice care should be identified as Declining Phase or Terminal Phase hospice care.
Figure 1 depicts the two phases of hospice. In the Declining Phase, patients will usually have a gradual deterioration in function requiring more and more care. With this overall loss of function, there is a decrease in quality of life. These patients have recognized that they have prioritized quality of life over quantity of days to be lived. But they still want more quantity, more days on this earth. The primary goal in hospice is to relieve suffering, but a secondary goal is to prolong life when acceptable quality remains. We commonly continue g-tube feedings in home hospice and treat infections with antibiotics. Medical management of heart failure is expected, and medications are rarely discontinued as long as the patient can still swallow. Though the hospice literature often states that life prolonging treatments are not continued, it is done all the time.
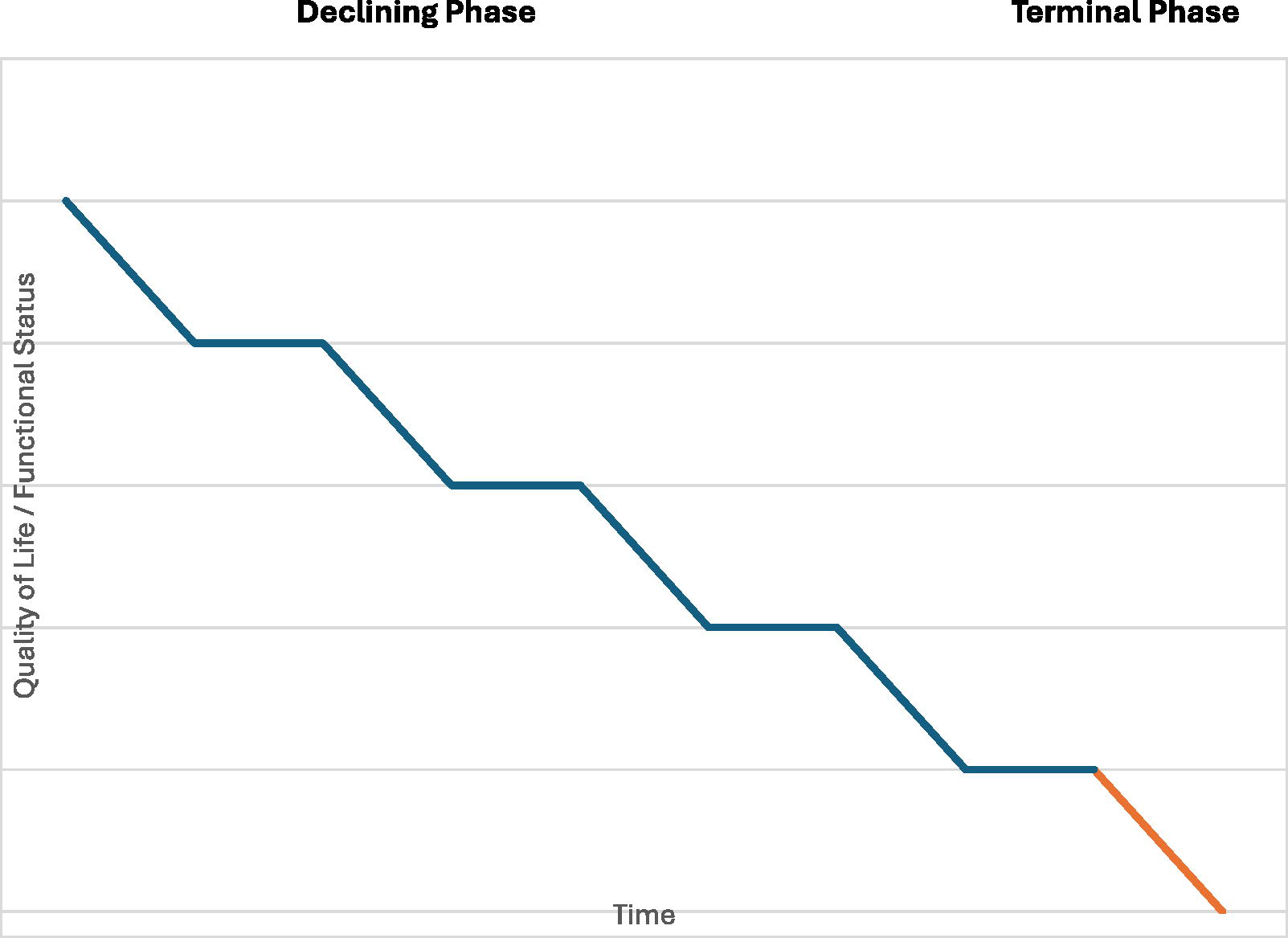
A typical progression of a hospice patient’s quality of life or functional status over the last six months of life. The blue segment of the graph represents Phase 1 of Hospice care, and the orange segment represents Phase 2.
As many patients progress and their bodies fail, they may enter the Terminal Phase of hospice care. This phase is identified by the patient and family and is that time when the quality of life is so poor, there is no goal to increase the number of days alive. We typically refer to this as a time for comfort meds only. This is a personal decision that some patients may not choose until they are semi-comatose and unable to tolerate nutrition or oral medications. Other patients may choose to forgo life-prolonging treatments much earlier. The Terminal Phase usually lasts days to weeks and based upon referral patterns, this is what many doctors seem to believe is the entirety of hospice care.
If, upon referral to hospice, a doctor was routinely asked “Is this a Declining Phase or Terminal Phase referral?” it would encourage discussion, education, and possibly a better understanding of the full scope of hospice care. If the nomenclature became widespread, it would also help patients and families better understand, appreciate, and accept earlier hospice referrals.
Authors Disclosure Statement
The author has no conflict of interests and no financial disclosures.
Finding Information
No funding was received for this article.