
Abstract
Introduction:
The needs of patients living with malignant neoplasm, and those of their families and care partners, require a multidimensional and interdisciplinary approach. By systematically assessing these needs with validated tools, healthcare professionals can identify and monitor therapeutic objectives, interventions, and results.
Objective:
At the Catalan Institute of Oncology (ICO), we set out to update the ICO Toolkit—a set of instruments for assessing the physical, emotional, and social needs of palliative care patients.
Methods:
We conducted a non-systematic review of the most common instruments currently used for multidimensional assessment of cancer patients nearing the end of life and then applied the Delphi method to achieve consensus on the instruments to be included in the updated ICO Toolkit-2. Initial consensus was obtained via interobserver agreement within a discussion group of experts, drawing on their daily clinical practice, and the published evidence. The Delphi method was then used to survey a representative sample of 22 experts from the ICO’s three interdisciplinary palliative care teams.
Results:
The final 19 instruments selected for the ICO Toolkit-2 achieved a degree of consensus of 90%–100%.
Conclusions:
The updated ICO Toolkit-2 facilitates a multidimensional, systematic, objective, and measurable assessment of the needs of malignant neoplasm patients throughout their cancer journey. Uptake of the new toolkit could improve the care and support provided to patients and their families and care partners.
Introduction
Palliative care is an acknowledged part of cancer control. It goes beyond prevention or cure to ensure the needs of all patients are met and has evolved from an end-of-life focus to improve quality of life across the cancer continuum. 1 Cancer remains deadly—for every new case of cancer, there are half as many deaths—but treatment breakthroughs continue to lower the risk of mortality and improve long-term survival.2–6 Palliative care is therefore essential in cancer care: Patients will live longer and have complex needs.
Accurate and early assessment is central to successfully addressing the problems and concerns that underlie patients’ needs. 5 Moreover, palliative care intervention has proven benefits for symptom control and survival.7–9 Specific assessment instruments for different symptoms can improve detection and outcomes, such as in the case of pain or depression.10,11 Such instruments can enable the various professionals and teams involved in patient care to share objective and reliable information at all stages. 12 Unfortunately, palliative care assessments are often neither systematic nor comprehensive, suggesting that clinicians may choose not to use the instruments or not be aware of them.11,13 To bridge this gap, in 2010 we designed a set of instruments at the Catalan Institute of Oncology (ICO) for the multidimensional assessment of patients with advanced cancer. 14 We named this set of instruments the ICO Toolkit.
ICO treats 45% of the cancer population in Catalonia, Spain. The interdisciplinary team, comprising three palliative care services, takes a comprehensive approach to treating cancer patients and supporting their families and care partners. As a result, ICO became an ESMO Designated Center of Integrated Oncology & Palliative Care i in 2007 and has since been reaccredited (currently valid until 2025). The original ICO Toolkit, published in 2010, was developed via a consensus process involving professionals from three of ICO’s main centers. 14 The kit included assessment instruments as well as specific questions that clinicians found most useful in palliative care assessments. It enabled clinicians to assess patients’ physical, psychological, and social symptoms and their needs.
Twelve years later, we have access to new instruments and new knowledge on the complex needs of palliative care patients living with advanced cancer. We have therefore updated the original kit with additional instruments and assessment domains (e.g., existential) to keep step with developments in the field.
By promoting best practices that draw on cancer treatment innovations, healthcare professionals can help meet the emerging needs of advanced cancer patients. This paper outlines the degree of consensus for the instruments in the updated ICO Toolkit-2, all of which facilitate a relevant, systematic, and comprehensive palliative care assessment. Moreover, our recommendations and their justifications provide a single point of reference for clinicians nationally and in the wider medical community.
Aim
To update the ICO Toolkit—a set of instruments for assessing the physical, emotional, and social needs of palliative care patients—and ensure palliative care clinicians in Spain, and in the wider medical community, are empowered to conduct a systematic and multidimensional assessment of the needs of malignant neoplasm patients and those of their families and care partners. Though our paper looks at palliative care in Spain specifically, multidisciplinary palliative care assessments are similar in all settings, and the ICO Toolkit-2 is therefore relevant to all professionals in this field, irrespective of their geographical location.
Target population
The ICO Toolkit-2 provides evidence-based recommendations for validated tools that interdisciplinary palliative care providers can use to address the needs of patients with malignant neoplasms and those of their families and care partners.
Design
Developing the recommendations
From March to October 2021, ICO conducted a non-systematic review of the most common instruments and scales for multidimensional palliative care assessments. Our findings informed the design of the new version of our toolkit: the ICO Toolkit-2. The draft updated toolkit was sent to our panel of experts for their consideration, and the agreed-upon tools were further supported with the evidence-based recommendations outlined in this paper.
Since our study did not involve patients, Institutional Review Board (IRB) approval was neither sought nor required.
Panel selection and composition
All members of the palliative care teams in ICO’s three main centers were invited to participate.
Approximately 4 weeks prior to the distribution of the Delphi survey, an invitation e-mail was sent to all potential participants outlining the objectives of the study. Any participant who actively declined at this stage was removed from future correspondence. We then issued our survey via Google Forms (this free, open-source survey software ensures anonymous participation). Before completing the survey, recipients were informed that their decision to participate would be interpreted as informed consent. Our selection criteria required that participants be healthcare professionals in the interdisciplinary palliative care team in any branch of the Catalan ICO. They must provide clinical palliative care to cancer patients and their families and care partners, hold the relevant knowledge and experience, and be willing to participate. The research team is responsible for data confidentiality and will safely store the data for 5 years after publication of the results.
The final panel comprised 12 palliative care physicians, 6 nurses, 3 psycho-oncologists, and 3 social workers. Two of the psycho-oncologists hold a PhD, and the other holds a master’s degree. Medical professionals with a master’s degree in palliative medicine were considered specialists in this area. ii
Delphi method
We applied the Delphi method to achieve consensus on the candidate instruments for the updated ICO Toolkit-2. We recommended 19 validated instruments to our experts in the first survey round. We asked two questions: the first gauged the degree of consensus [using a seven-point scale from 1 (strongly disagree) to 7 (totally agree)] on the clinical relevance of the instrument for assessing a specific domain or symptom (e.g., the CAGE Test to detect alcohol-related disorders in adults); the second allowed the experts to make additional comments.
A subsequent round provided summary feedback to participants on the average response to each question, as well as each panelist’s specific response. In accordance with the Delphi method, only those questions that did not achieve consensus in the first round were submitted for further response.
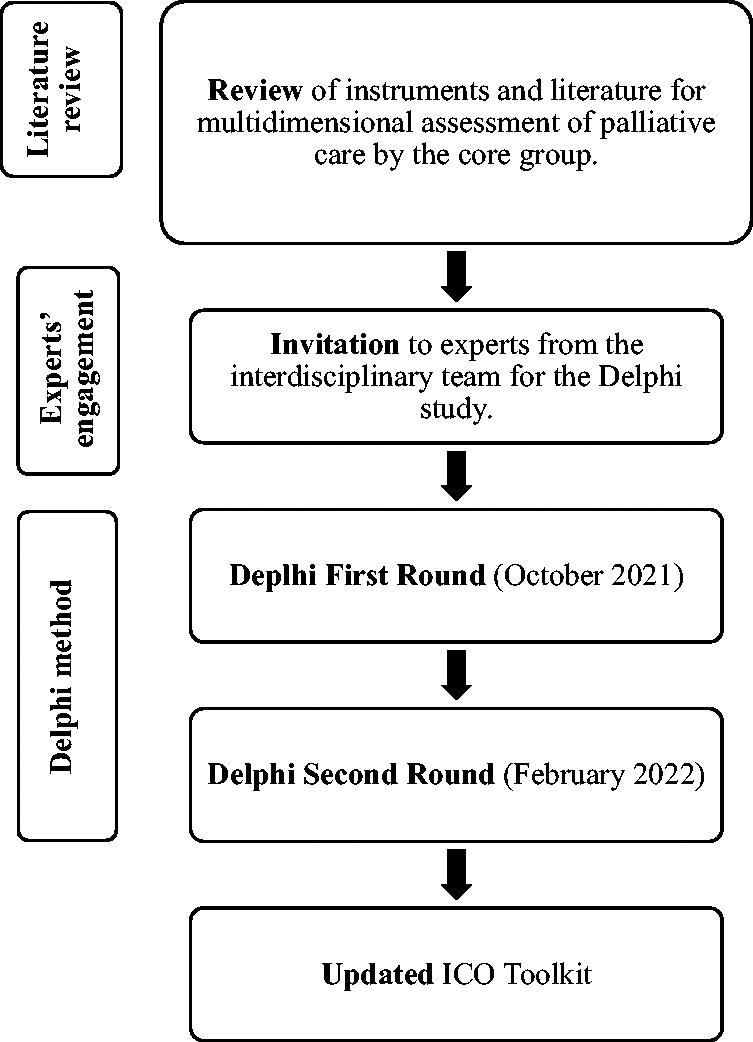
The following PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses)-type flowchart outlines our process:
Results
Delphi method results
In the first round, the questionnaire was answered by 22 of the 24 invited panelists, comprising 6 men and 18 women in age brackets of 30–40 years (25%), 40–50 years (50%), or over 50 years (25%). One panelist had fewer than 5 years’ experience in palliative care, while almost three quarters of panellists had more than 10 years’ experience. Figures 1 and 2 provide further details on the participants’ disciplines and professional experience.

Delphi participants’ disciplines.

Delphi participants’ professional experience.
Of the 19 tools recommended initially, 15 achieved strong consensus while 4 achieved an intermediate degree of consensus.
In the second round, the questionnaire was answered by 16 panelists and only included the four recommendations that did not achieve strong consensus in the first round. Three of these attracted strong consensus in the second round while the other maintained an intermediate degree of consensus. The results of the first and second rounds of the Delphi method are presented in Figures 3 and 4, respectively. Figure 5 shows the final results of the Delphi method.
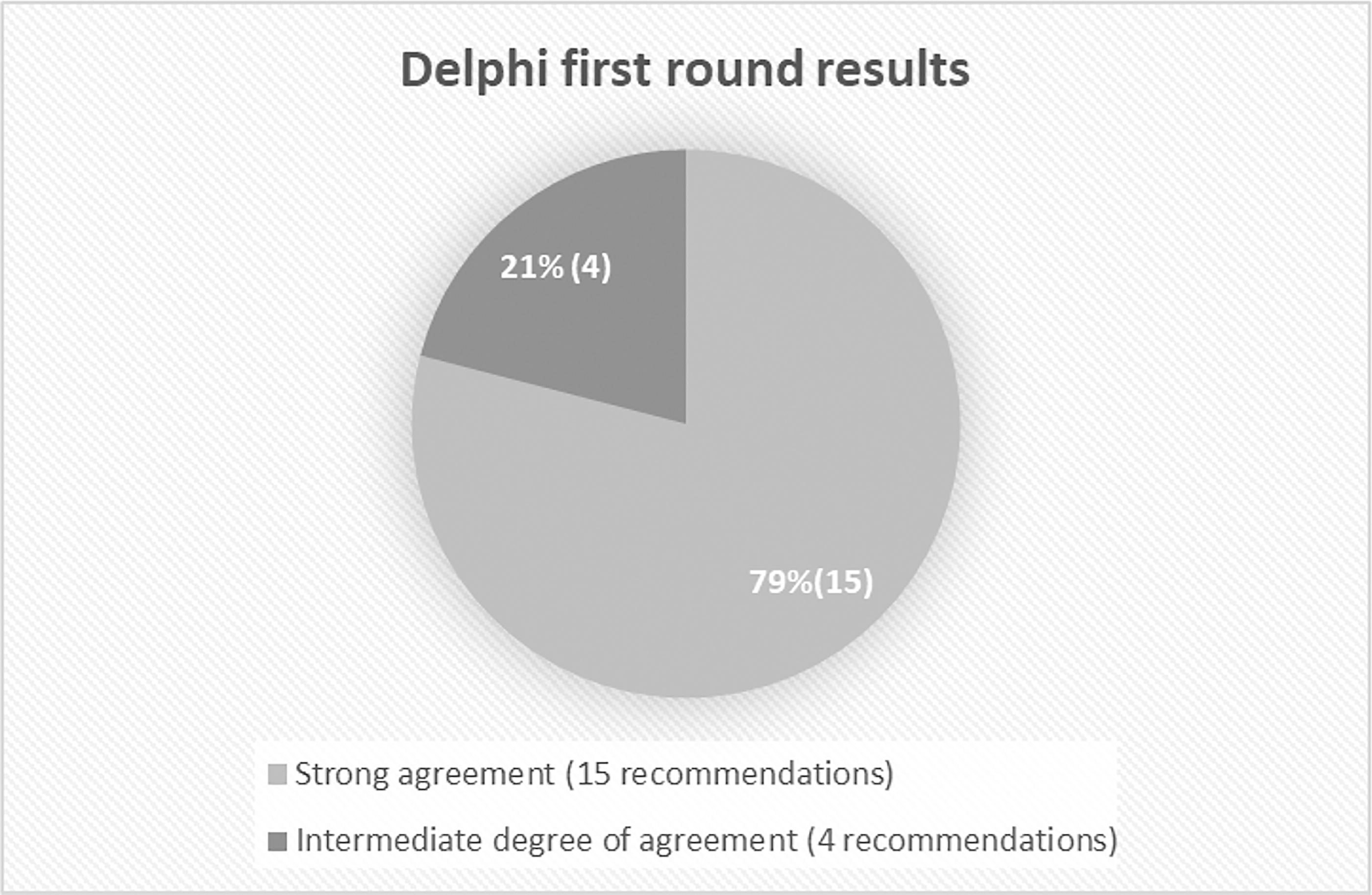
Delphi first round results.
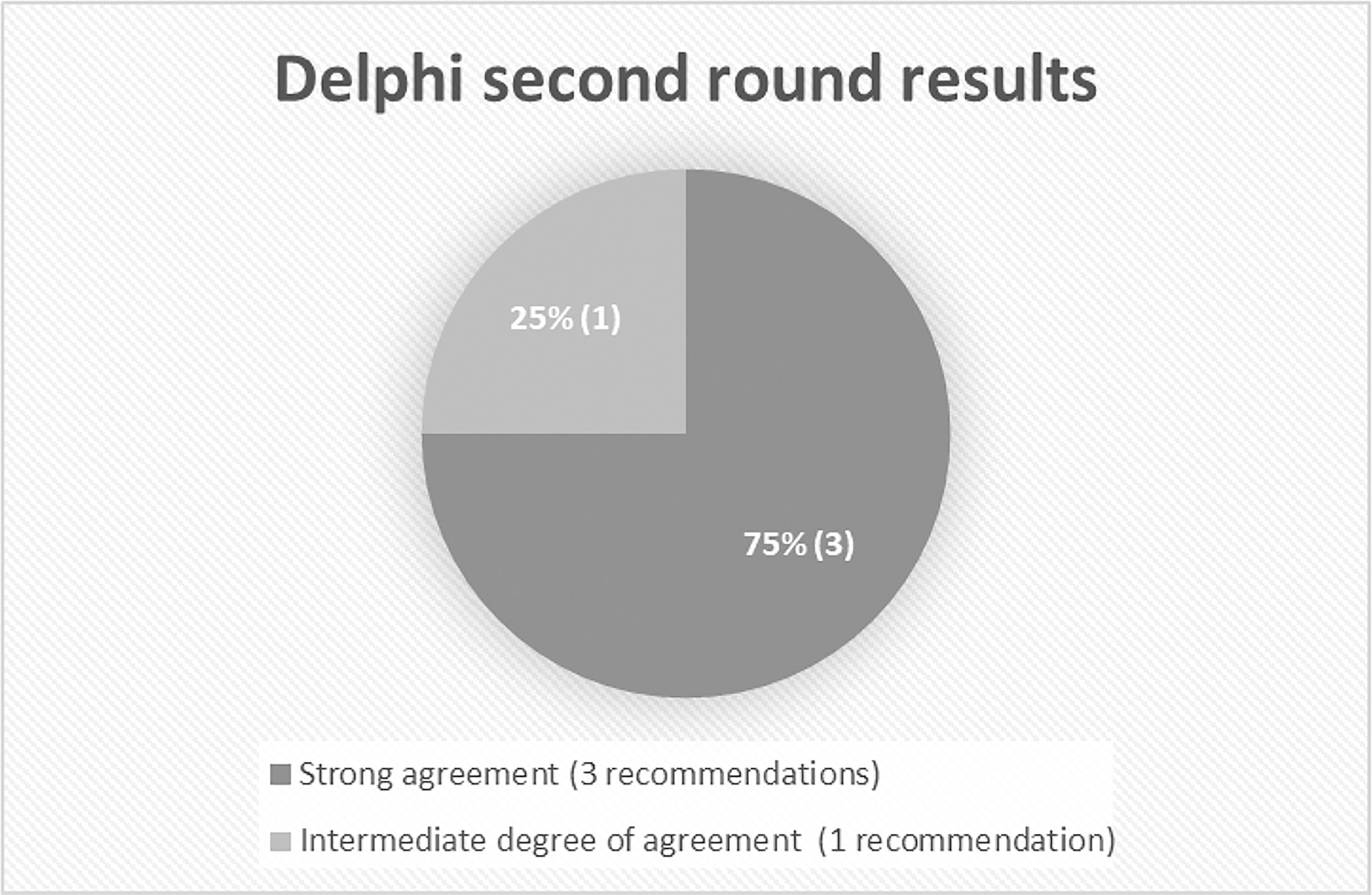
Delphi second round results.
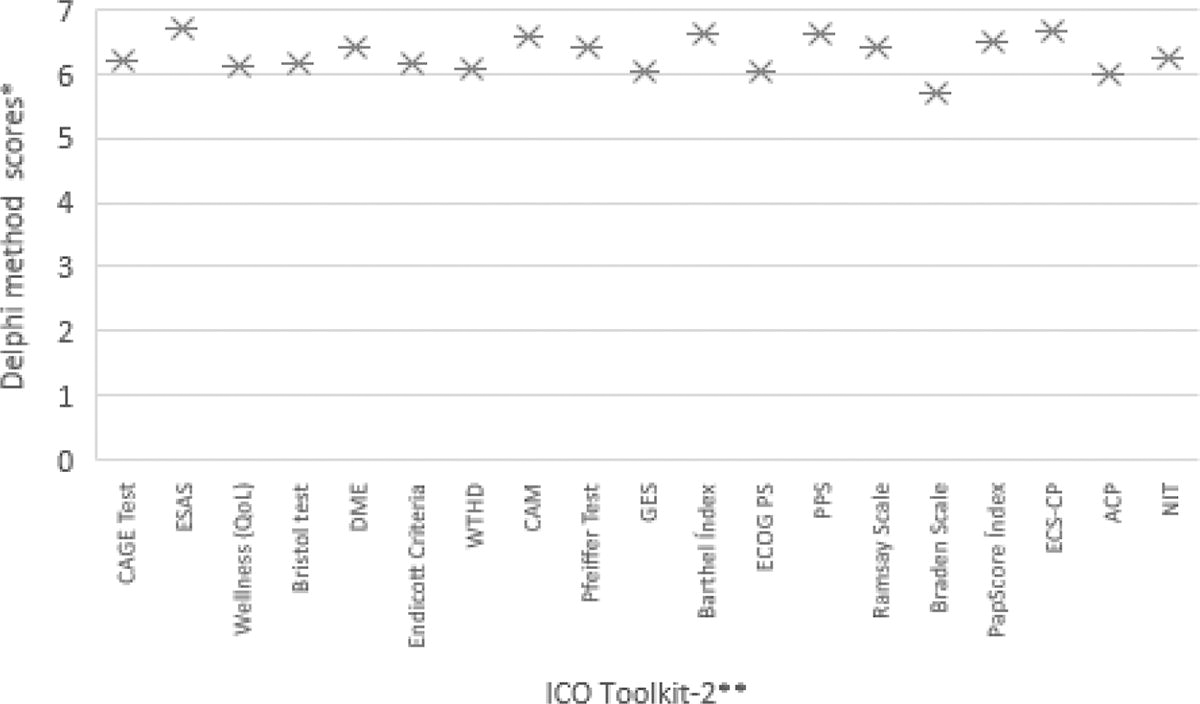
Delphi final results. *The score was assessed on a scale from 0 to 7, where 0–1 = totally disagree, 2–3 = disagree, 4–5 = somewhat agree (intermediate), 6 = strongly agree, and 7 = totally agree. **ESAS, Edmonton Symptom Assessment System; QoL: quality of life; DME: Emotional Disorder Detection. Questionnaire; WTHD: wish to hasten death; CAM: Confusion Assessment Method; GES: Grupo Espiritualidad de la SECPAL-Scale developed by the Spirituality Group of the Spanish Palliative Care Society; ECOG PS: Eastern Cooperative Oncology. Group Performance Status; PPS: Palliative Performance Scale; ECS-CP: Edmonton Classification System. for Cancer Pain; ACP: advanced care planning; NIT: diagnostic and therapeutic intervention levels. The following instruments were not part of the original toolkit: Braden Scale, DME, WTHD, RamsayScale, ACP, NIT.
We will now outline the tools contained in the updated ICO Toolkit-2, including the degree of consensus and justification for each recommendation.
Recommendations: the ICO toolkit-2
The recommendations that follow make up the ICO Toolkit-2. We have grouped the recommendations in a way we feel best supports healthcare teams in assessing patients, starting with the physical dimension before addressing emotional, cognitive, and spiritual needs. This is the order typically used when taking the patient’s history.
Some specific assessment stages contain multiple recommendations. For example, Sign and Symptom Assessment comprises four recommendations: a more generalized screening instrument is recommended first, followed by instruments with a narrower focus. The three recommendations under Functional Assessment follow the typical order in which the tools are used in clinical practice at the Catalan ICO, for example.
Healthcare professionals should feel free to approach the recommendations in a different order if doing so would better serve the needs of their patients. While the conversation with the patient may lead them in one direction or another, referring back to the toolkit will help ensure that the assessment is systematic and that all needs are addressed.
Antecedents assessment
Symptom and sign assessment
Functional assessment
The ECOG PS Scale assesses changes in the patient’s ability to perform the activities of daily living, with scores ranging from 0 (fully active) to 5 (dead).27,31
The PPS measures the functional impairment of a palliative care patient across five domains: ambulation, activity level and evidence of disease, self-care, intake, and level of consciousness. 28
Though the available scales were developed with different objectives, they are equally valid and reliable and may be used interchangeably.30–33
Emotional assessment
Cognitive assessment
Spiritual assessment
The GES scale has factorial validity, clear evidence of reliability (α = 0.72), and a coherent relationship with other measures of spirituality, depression, anxiety, and resilience.
The Spirituality Group recommends that use of the scale be limited to experienced professionals with knowledge of the GES model and an empathic and trusting relationship with the patient. Candidate patients are those with advanced or terminal illness and an awareness of the possibility of imminent death.43,45
Sedation assessment
One objective of such scales is to assess the quality of palliative sedation. 47 The Ramsay sedation scale sometimes falls short for intensive care unit patients but is nonetheless frequently used in palliative care, alongside other tools such as the Richmond Agitation Sedation Scale.47,48 A systematic review found no clear evidence on the overall quality or effectiveness of palliative sedation and concluded that work is needed to identify assessment parameters. 47 Since the Ramsay scale is relatively easy to use and commonplace in palliative care, it achieved a high degree of consensus from our experts.
Prognosis assessment
Advanced care planning assessment
Diagnostic and therapeutic intervention
Improve the cost-effectiveness of end-of-life care, based on the available scientific evidence. Reduce the variability of approaches between ICO teams. Facilitate a comprehensive and multidimensional approach to the end-of-life process in patients with malignant neoplasm. Establish assessment criteria for end-of-life patients.
The Catalan Institute of Oncology Diagnostic and Therapeutic Intervention Levels
Patients nearing the end of life may receive different diagnoses and be subject to different therapeutic approaches depending on the disease stage, type of complication, or even the treating professional they encounter at any given time. In the Diagnostic and Therapeutic Intervention Levels, the patient’s assigned level is recorded, and all healthcare providers agree on the clinical approach in the event of complications. The patient’s level may vary over the course of their hospitalization.
In palliative care, the concept of limitation of therapeutic effort (LTE) means not taking heroic or disproportionate measures for patients with a poor short-term prognosis or poor quality of life.60,63,64 Limiting therapeutic effort may involve withholding or withdrawing certain treatments. It may also mean that healthcare teams proactively offer or modify measures based on the current therapeutic goals and the resources available. ICO’s Diagnostic and Therapeutic Intervention Levels, developed in Spanish, help ensure practical application of LTE for patients with malignant neoplasm. 60 Bioethical principles must be considered when LTE is adopted.
Discussion
The ICO Toolkit-2 is a significant step forward from the original toolkit, with several new recommendations included:
Recommendation 5 on the Braden Scale. Recommendation 9 on the Emotional Disorder Detection Questionnaire. Recommendation 11 on the WTHD. Recommendation 15 on the Ramsay Scale. Recommendation 18 on shared decision-making/advanced care planning. Recommendation 19 on the ICO Diagnostic and Therapeutic Intervention Levels.
The instruments in the original toolkit were selected by a working group comprising five doctors, four psycho-oncologists, and four social workers, with no nursing representation. The 24 professionals involved in the Delphi process for the ICO Toolkit-2 included six nurses selected from ICO’s three main centers. This adds a valuable additional dimension to the toolkit, given the involvement of nurses throughout the patient care journey—particularly in palliative care—in supporting families and care partners.
Cancer patients in palliative care have multifaceted needs. These needs, and those of their families and care partners, are likely to change over the course of treatment. Though several instruments exist for conducting a multidimensional assessment, there is little guidance currently on how and when to implement them.
Like its predecessor, the idea behind the ICO Toolkit-2 is to facilitate a systematic palliative care assessment that comprehensively addresses patients’ needs. The toolkit format pools our recommendations in one place, giving healthcare professionals a central point of reference and clear guidelines to aid their decision-making around patient care and follow-up.
Lastly, the toolkit goes beyond the physical dimension, with instruments to assess emotional, cognitive, and spiritual needs. This provides scope for encompassing unique social and cultural factors that may, in turn, determine which recommendations are most appropriate on an individual basis.
Conclusions
The updated ICO Toolkit-2 supports clinicians to conduct a systematic, multidimensional assessment of patients with malignant neoplasm in palliative care. With the toolkit, clinicians can objectively identify and measure the needs of these patients and those of their families and care partners. Furthermore, they can record the results of interventions to aid both clinical practice and research.
Use of the toolkit nationally, and by the wider medical community, may go some way to ensuring consistency of care for patients with malignant neoplasms receiving palliative care. Decisions on whether to apply the toolkit should be made in agreement with all healthcare professionals involved in patient care.
The recommendations should be updated in response to new palliative care instruments and tools that become available.
Footnotes
Acknowledgments
The authors thank Kelsie Pettit DipTrans MCIL for external editing services and English language support. The authors also thank the three Palliative Care Services of the Catalan Institute of Oncology—L’Hospitalet de Llobregat, Badalona, and Girona—for their participation.
Author Disclosure Statement
The authors declare they have no conflicts of interest to disclose.
Funding Information
The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.