
Abstract
Background:
Patients with end-stage liver disease (ESLD) have complex needs and may benefit from palliative care (PC), which is often underutilized or delayed.
Objectives:
To characterize patients with ESLD who received inpatient PC consultation and to explore differences in characteristics between those who received PC consultation before (pre-Pall) or after (post-Pall) PC participation at weekly liver transplant (LT) Patient Selection Committee (PSC) meetings.
Design:
Single-center retrospective cohort study.
Setting/Subjects:
Hospitalized patients with ESLD who received inpatient PC consultation between February 2017 and February 2019 at an academic LT center in the United States.
Measurements:
PC referral reasons and timing, code status, hospice referrals, discharge location, and mortality.
Results:
Two hundred five patients were included. The primary reason for PC was goals of care (88.8%; n = 182). Most (86.8%; n = 178) were Full Code at hospital admission, while 81% (n = 166) were do-not-resuscitate at discharge. Nearly one quarter (22.9%; n = 47) sought life-prolonging care at discharge, while 41.5% (n = 85) were discharged with hospice, and 34.1% (n = 70) died before discharge. By the end of the study, 85.9% (n = 176) were confirmed as deceased. Median time from PC to hospice referral was 12 days [95% confidence interval [CI]: 8–23]. Median time from PC consult to death was 13 days [95% CI: 9–17] and from hospice referral to death was 7 days [95% CI: 4–13]. There were no statistically significant differences between the pre- and post-Pall groups related to PC referral patterns or outcomes.
Conclusions:
Most PC contacts occurred near end of life, and many led to comfort-focused care. Late referrals may be due to reliance on inpatient consults during acute illness. PC presence at PSC meetings represents an important step in collaboration with LT teams but did not lead to direct impact on PC referral patterns or outcomes.
Key Message
This retrospective study on palliative care referrals and outcomes for patients with end-stage liver disease shows that inpatient consultation generally occurs near the end of life, often just prior to a shift in care goals, which highlights the limitations of a primarily inpatient-based care model.
Introduction
End-stage liver disease (ESLD) represents cirrhosis with one or more disease-defining complications, specifically hepatic encephalopathy, jaundice, refractory ascites, and variceal hemorrhage. 1 Both the prevalence and mortality of advanced liver disease continue to rise,2–4 and despite an overall increase in rates of liver transplant (LT), 5 long-term survival is limited for patients who cannot undergo LT.1,2,6,7
Patients with ESLD often have unpredictable clinical trajectories and complex advance care planning (ACP) needs, which could benefit from palliative care (PC), independent of LT status and overall prognosis. 8 Current literature supports a model of PC delivered concurrently with potentially curative measures.9,10
While population-based studies have demonstrated a modest increase in inpatient PC utilization for patients with ESLD,11,12 the proportion of patients with ESLD who receive PC consultation remains quite low.11–16 PC referrals often do not occur until end of life (EOL), if at all,13,17 even for patients ineligible for LT,14–16 and most contacts occur in an inpatient setting.13,15–17 Many factors may contribute to delayed referral and reliance on inpatient PC, including lack of evidence-based guidance on the optimal timing of PC referral 18 and limited access to outpatient PC for noncancer diagnoses.19,20
It is essential to understand existing PC utilization patterns to identify opportunities for practice change. The primary aim of this retrospective cohort study was to characterize patients with ESLD hospitalized at a large academic LT center in the United States who received inpatient PC consultation over a two-year period. Our secondary aim was to explore differences in characteristics between those who received PC consultation before (pre-Pall) or after (post-Pall) PC participation at weekly LT Patient Selection Committee (PSC) meetings.
Methods
Study design
This was a retrospective cohort study of adults (age ≥18) with ESLD hospitalized at The Ohio State University (OSU) Wexner Medical Center between February 5, 2017, and February 4, 2019. We followed death as an outcome until January 17, 2020 (censoring as of January 18, 2020). We identified patients by the presence of International Classification of Diseases (ICD)-9 and ICD-10 codes associated with both cirrhosis and PC, then confirmed the presence of at least one disease-defining complication of ESLD (ascites, jaundice, hepatic encephalopathy, and/or variceal hemorrhage) via manual chart review (Table 1). We included incarcerated patients who otherwise met the inclusion criteria. We excluded pregnant patients, those with hepatocellular carcinoma (HCC) without defined ESLD, and hospitalized patients with ESLD who did not receive a completed PC consultation. We also excluded patients who had contact with PC prior to the study timeframe. The OSU Institutional Review Board approved this study.
ICD-9 and ICD-10 Codes Used for Cohort Discovery
Setting
This study was conducted at a large academic tertiary care transplant center in which the program demonstrated a 35% increase in LT volume from FY17 to FY19. When hospitalized, patients with ESLD may be admitted to general medicine, a dedicated hepatology service, or to the intensive care unit. Patients under consideration for LT are discussed at a weekly multidisciplinary PSC meeting, which has included a PC physician since February 5, 2018. During this meeting, the PC physician is available to provide feedback on topics that arise during discussion, including pain and symptom management, goals of care, and hospice referral.
Within our health system, inpatient PC consultation is available daily, and the consult teams include board-certified PC physicians, nurse practitioners, social workers, and pharmacists. Typical inpatient consultation includes an initial assessment by a PC physician, with attention to symptoms, identification of surrogate decision makers, and evaluation of patient and family understanding of their diagnosis, prognosis, and treatment options. Follow-up visits are conducted by a PC nurse practitioner, physician, or social worker as indicated. At our institution, outpatient PC is available for patients with cancer, but these services are not readily available for patients with ESLD without active malignancy.
Outcomes and variables
Study data were collected and managed using REDCap electronic data capture tools hosted at OSU.21,22 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture, (2) audit trails for tracking data manipulation and export procedures, (3) automated export procedures for seamless data downloads to common statistical packages, and (4) procedures for data integration and interoperability with external sources. We utilized the first hospital admission that contained a PC contact during the study time period, and we collected data from the electronic medical record (EMR) including patient demographics, etiology of liver disease, lab values (total bilirubin, creatinine, INR, sodium) to calculate Model of End-Stage Liver Disease (MELD) score 23 at admission and discharge, date of hospital admission and discharge, hospital length of stay, and transplant status (Table 2). We also recorded ACP information (code status and presence of health care power of attorney [HCPOA] at admission and discharge), the date and reason for PC consultation, discharge location (home, skilled nursing facility [SNF], long-term acute care hospital [LTACH], or deceased in hospital), date of hospice referral (if applicable), and details of death (location, date, and cause) (Table 3). For incarcerated patients, the discharge location was a correctional facility, with hospice designation as applicable. We used publicly accessible obituaries to supplement death data if unavailable in the EMR or if death occurred after hospital discharge. For those who died after their hospitalization, we recorded death dates that occurred up to 11 months following the study period.
Patient Demographics and End-Stage Liver Disease Characteristics
Presented as n (%) for categorical variables and either mean (SD) or median [min, max] for continuous variables as indicated.
Calculated using Fisher’s exact test for categorical variables and either a two-sample t test or Wilcoxon Rank-Sum test for continuous variables.
Missing data: MELD score unable to be calculated for eight patients within total cohort (four from pre-Pall and four from post-Pall).
Missing data: MELD score unable to be calculated for 49 patients within total cohort (22 from pre-Pall and 23 from post-Pall).
Four patients within the total cohort had been previously transplanted but were not re-referred.
LT, liver transplant; MELD, Model of End-Stage Liver Disease; SD, standard deviation.
Advance Care Planning, Palliative Referrals, and Disposition
Presented as n (%).
Calculated using Fisher’s exact test for categorical variables and either a two-sample t test or Wilcoxon Rank-Sum test for continuous variables.
Includes DNRCC-A and DNRCC, which are the code status options per Ohio Revised Code. 24
Patients could complete HCPOA during encounter even if they had a previous document on file.
In the full cohort, 16 patients consulted for medication management, six for end-of-life care, and one for preparedness planning for LT.
Missing data: three discharge locations unknown.
DNRCC, do-not-resuscitate comfort care; HCPOA, health care power of attorney.
Statistical analyses
Descriptive statistics were analyzed for all variables at admission. Fisher’s exact tests for categorical variables and t tests for continuous variables that were normally distributed or Wilcoxon Rank-Sum tests for continuous variables that were not normally distributed were used to test for differences between the pre-Pall group, defined as those who received inpatient PC consultation before the establishment of PC presence at PSC on February 5, 2018, and the post-Pall group, defined as those who received their PC consultation on or after that date. For the outcome of time-to-death, patients were not included if they were either lost to follow-up or were alive at the end of the study. For the outcome of time-to-hospice referral, patients were not included if they were lost to follow-up, the study ended, or the patient experienced death. Kaplan–Meier curves were tested for differences using the log-rank test. P values below 0.05 were considered statistically significant, and all confidence intervals were reported at their nominal levels. All analyses were performed using Stata version 15.1 and R version 4.0.0.
Results
Study cohort development
Initial cohort discovery yielded 694 patient records; however, 464 were excluded (duplicate charts, multiple encounters for the same patients, patients with cirrhosis without ESLD-defining complications, HCC without ESLD, or absence of completed PC consultation) (see Fig. 1). There were 230 unique patient encounters in the study period. We excluded patients whose first PC contact occurred prior to the study period (n = 25), yielding a final cohort of 205 patients. Eight patients had more than one PC encounter within the study period, so we utilized the first hospitalization for data analysis.
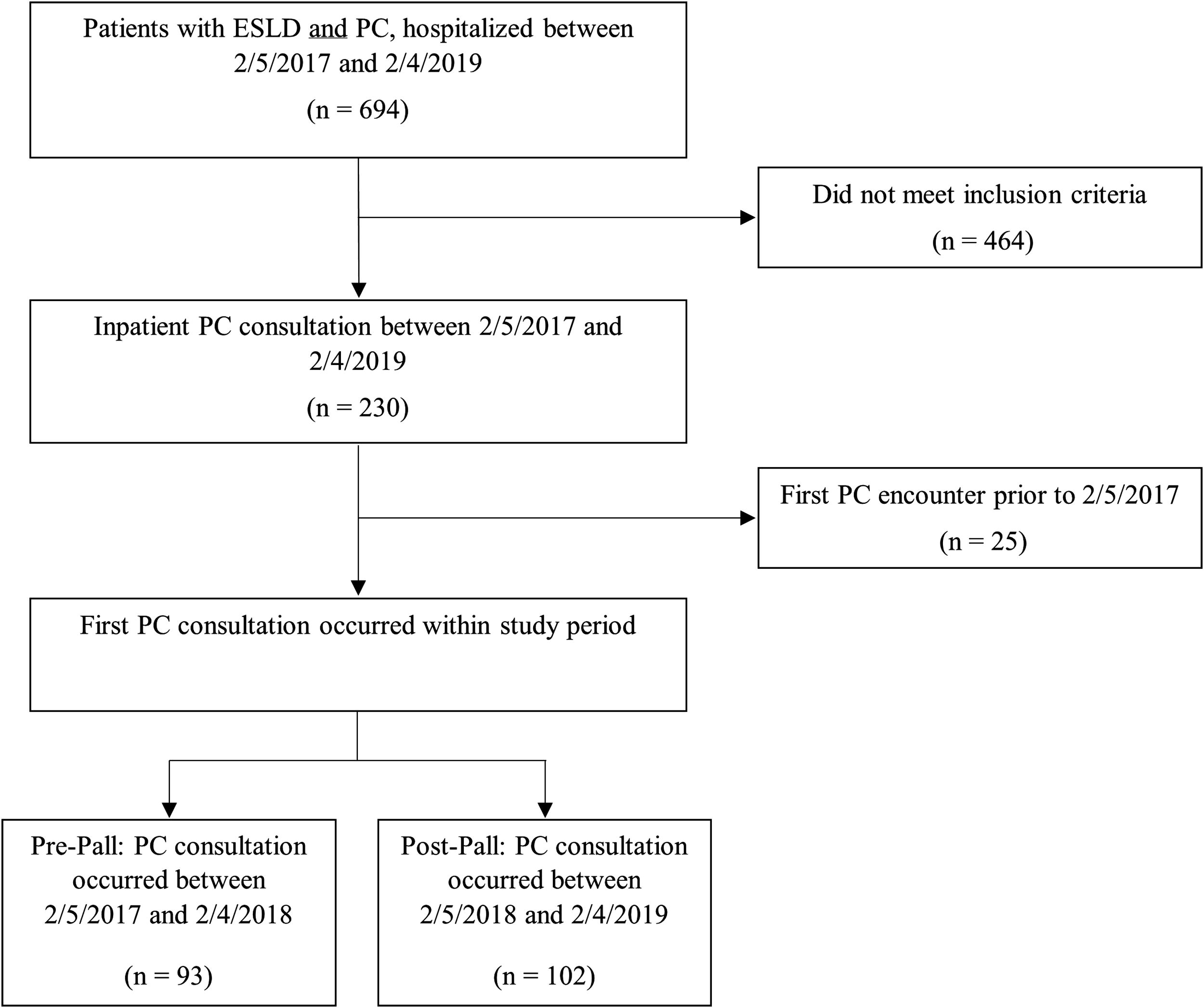
CONSORT diagram. Study cohort development. We included patients with ESLD (cirrhosis with at least one disease-defining condition of hepatic encephalopathy, jaundice, varices, and/or ascites) who had an inpatient PC consultation during hospitalization in the study period. We excluded pregnant patients, patients with acute liver failure without known ESLD, and those with HCC without a confirmed diagnosis of ESLD. ESLD, end-stage liver disease; HCC, hepatocellular carcinoma; PC, palliative care.
Demographics and disease characteristics for full cohort
The mean age was 61 (standard deviation [SD] 12.2) years at time of admission, and the cohort was 61.5% male (n = 126) (Table 2). The most common liver disease etiologies were alcoholic liver disease (37.1%, n = 76), metabolic dysfunction-associated steatohepatitis (23.4%, n = 48), and viral hepatitis (18%, n = 37). Median MELD score at admission was 26 [min, max: 7, 40] and at discharge was 29 [min, max: 6, 40]. Due to missing data, MELD scores were unable to be calculated for eight patients at admission and 49 patients at discharge. Median length of stay for the studied hospitalization was 12 days [min, max: 1, 98]. Thirty-nine patients (19%) had been referred for LT evaluation prior to time of PC contact.
PC referral patterns and patient outcomes for full cohort
The majority (88.8%; n = 182) of referrals were for “goals of care,” with three referrals specifying “concurrent care” in the reason for consult (Table 3). The proportion of patients with an active HCPOA form increased from 23.9% (n = 49) at admission to 38.0% (n = 78) by discharge. Most patients (86.8%; n = 178) were Full Code at admission, but by the end of hospitalization, 19% (n = 39) remained Full Code, with the majority (81%; n = 166) having the code status do-not-resuscitate comfort care—arrest (DNRCC-A), reflecting the decision to forgo resuscitative attempts at cardiac arrest but to continue disease-directed therapies, or do-not-resuscitate comfort care (DNRCC), reflecting the decision to receive comfort measures only. 24 Among patients who died during the study hospitalization (n = 70), code status at time of death was DNRCC-A (2.9%, n = 2) or DNRCC (97.1%, n = 68). Two patients (2.8%) transitioned from Full Code to DNRCC-A, 58 patients (82.9%) transitioned from Full Code to DNRCC, and 10 patients (14.3%) transitioned from DNRCC-A to DNRCC.
At the time of discharge, 22.9% (n = 47) of patients continued to seek life-prolonging care and were discharged to prior residence or a medical facility (SNF or LTACH). Three patients (1.5%) were missing data related to discharge location. Over half (50.7%; n = 104) of the cohort had a hospice referral placed following PC contact, and of those patients, 85 (41.5%) discharged from the hospital with hospice services, 11 (10.6%) died prior to hospital discharge, and eight (7.7%) were unable to have hospice enrollment confirmed. Median time from PC consult to hospice referral was 12 days [95% CI: 8–23] (see Fig. 2). Seventy patients (34.1%) died prior to hospital discharge, and by the end of the study, 176 patients were confirmed as deceased (85.9%). Median time from PC consult to death was 13 days [95% CI: 9–17] (see Fig. 3). Median time from hospice referral to death was 7 days [95% CI: 4–13] (see Fig. 4).
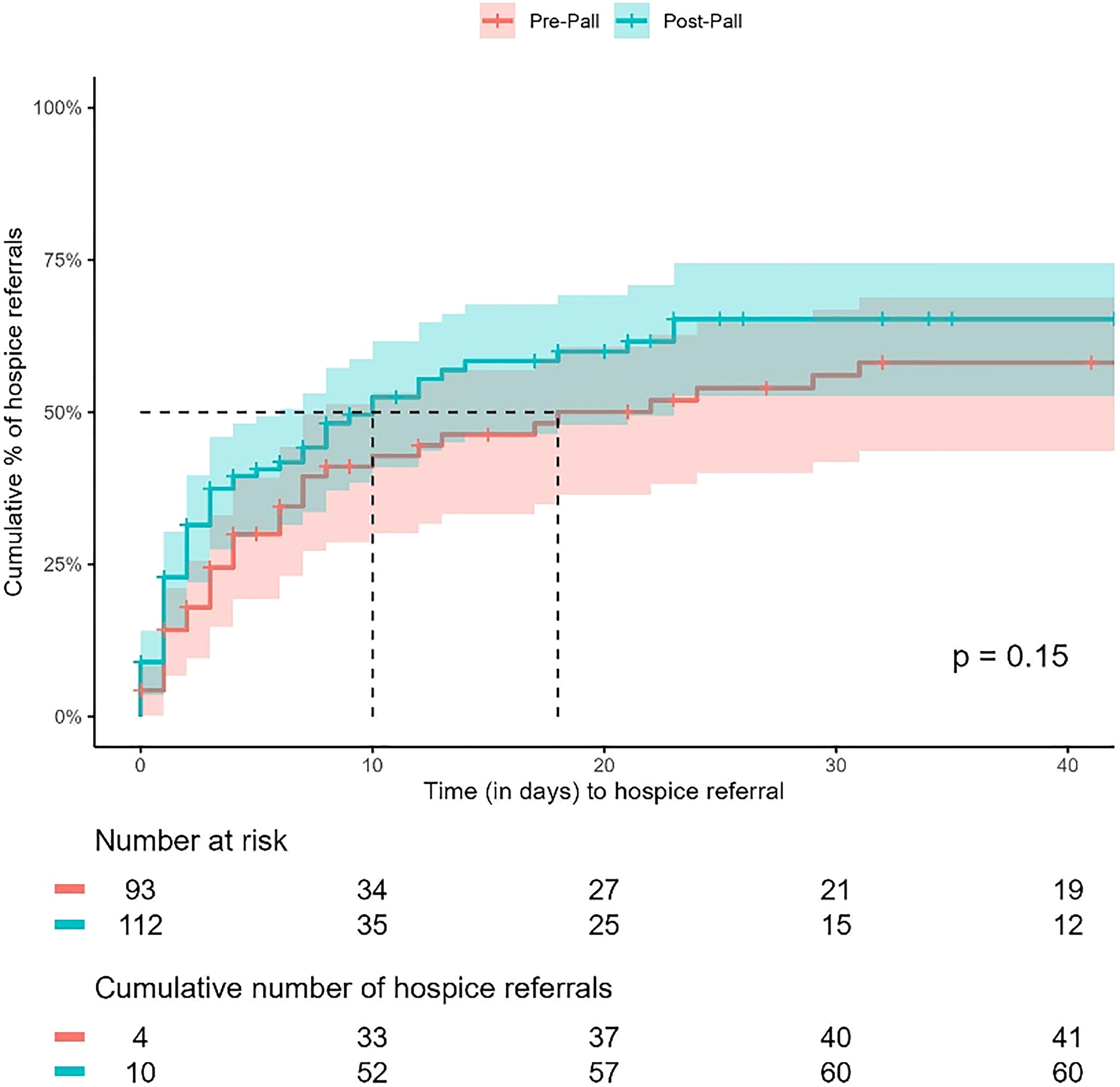
Time from PC consult to hospice referral by presence of PC at transplant PSC. Kaplan–Meier curves with outcome of median time from PC consult to hospice referral. The median time to hospice referral for the entire cohort was 12 days [95% CI: 8–23]. The median time from PC consult was 18 days [95% CI: 7–95] for the pre-Pall group and 10 days [95% CI: 5–21] for the post-Pall group (p = 0.15). CI, confidence interval; PSC, patient selection committee.
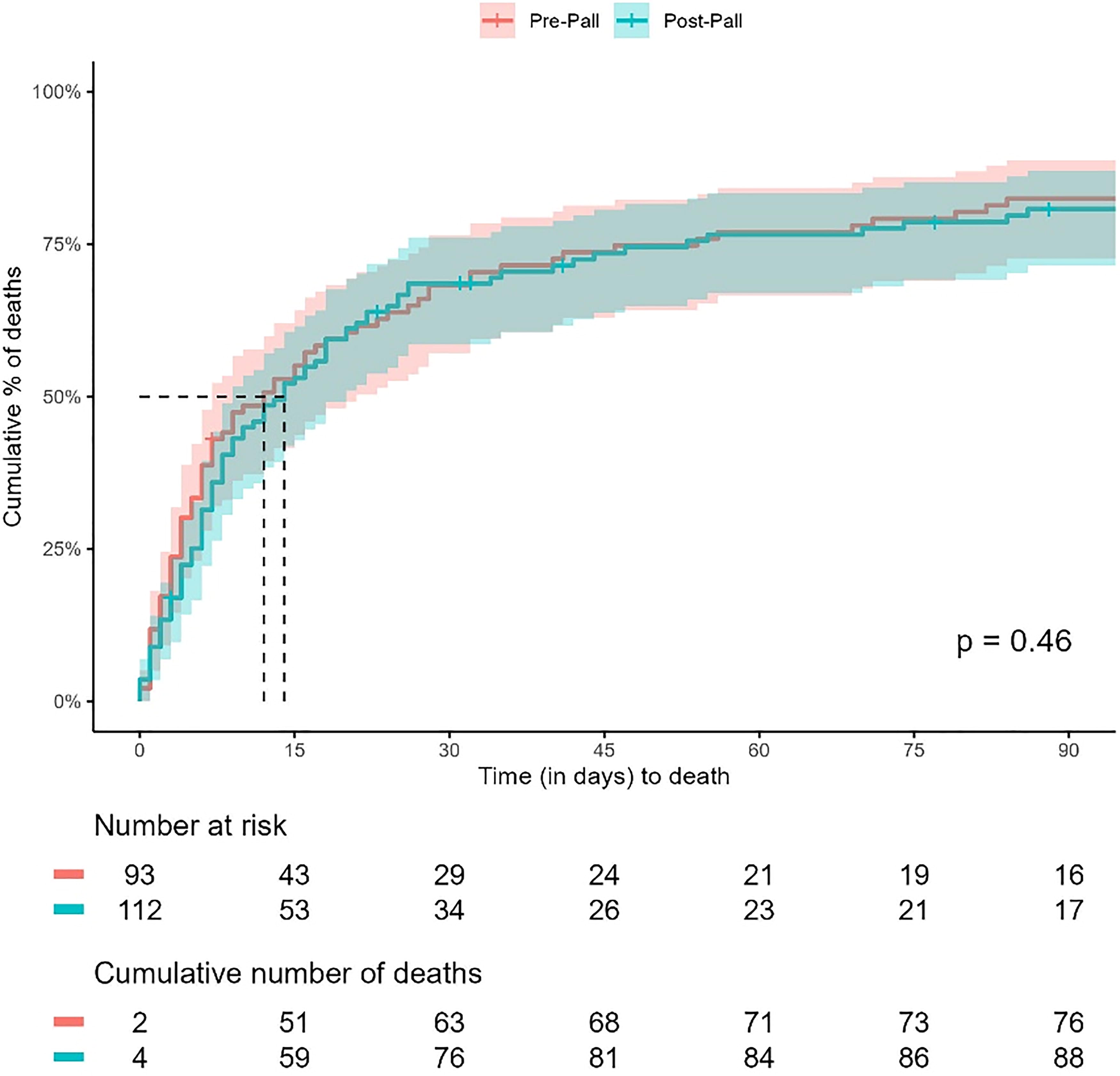
Time from PC consult to death by presence of PC at transplant PSC. Kaplan–Meier curves with outcome of median time from PC consult to death. The median time for the entire cohort was 13 days [95% CI: 9–17]. The median time from PC consult to death was 12 days [95% CI: 7–20] for the pre-Pall group and 14 days [95% CI: 8–18] for the post-Pall group (p = 0.46).

Time from hospice referral to death by presence of PC at transplant PSC. Kaplan–Meier curves with outcome of median time from hospice referral to death for the 104 patients with a hospice referral. The median time for the entire cohort was 7 days [95% CI: 4–13]. The median time from hospice referral to death was 4 days [95% CI: 3–13] for the pre-Pall group and 11 days [95% CI: 5–14] for the post-Pall group (p = 0.10).
PC utilization related to representation at transplant PSC
There were 93 patients in the pre-Pall group and 112 patients in the post-Pall group. Median time from PC consult was 18 days [95% CI: 7–95] for pre-Pall and 10 days [95% CI: 5–21] post-Pall (p = 0.15) (see Fig. 2). Median time from PC consult to death was 12 days [95% CI: 7–20] for pre-Pall and 14 days [95% CI: 8–18] post-Pall (p = 0.46) (see Fig. 3). Median time from hospice referral to death was 4 days [95% CI: 3–13] for pre-Pall and 11 days [95% CI: 5–14] for post-Pall (p = 0.10) (see Fig. 4). Additional comparisons between pre- and post-Pall are reported in Tables 2 and 3.
Discussion
In this retrospective cohort study, we found that utilization of PC at our institution trends toward EOL, with most patients discharging with hospice or dying in the hospital following PC contact. We propose two major factors that contribute to these patterns—limited evidence-based guidelines on optimal timing for PC integration and limited access to outpatient PC for patients with ESLD, leading to a reliance on inpatient PC contact.
Our finding of median time of 13 days from PC consult to death and 7 days from hospice referral to death is comparable with other studies for patients with ESLD,13,15,16 with our results falling in the middle of the existing paradigm of early versus late consultation for ESLD. For patients with ESLD, Barnes et al. defined early PC referral as one that occurred at least 30 days prior to death, 10 and Holden et al. defined late referrals as those occurring within one week of death. 25 Notably, the definition of early contact in ESLD is still late compared with conventions in other life-limiting illnesses. For patients with heart failure, late consults have been defined as occurring within 30 days of death, 26 while for patients with pancreatic cancer, late PC consultation has been defined as that which occurs within 30–90 days before death.27,28 This timeframe is further supported by Potosek et al., who noted that after hospice referral, patients with ESLD had an average survival of 29 days, as compared with the overall mean hospice length of stay of 59 days. 6 Patients with ESLD can face an unpredictable terminal phase of illness, making it challenging to deliver ideally timed early PC. 1 Likewise, LT providers have reported challenges in prognostication at EOL and a lack of clear referral criteria as major barriers to earlier PC involvement. 18 It remains to be seen whether emerging evidence-based guidance on PC integration will be sufficient to overcome these barriers and historical practice patterns.
We also suggest that the lack of outpatient PC contributes to the pattern of late contact. For patients with ESLD, hospitalization is often prompted by life-threatening decompensation events. Even if a consult occurs early in the hospitalization, it follows that many ESLD PC contacts occur in proximity to EOL, as supported by our study. Ideally, upstream PC would be supported by access to outpatient specialist PC for patients with noncancer diagnoses, but these resources are limited, even at large academic transplant centers. Despite increasing demand, implementation and adequate scaling of sustainable outpatient PC is often hindered by cost, finite resources, and a limited workforce. 19 Further, the existence of a dedicated ambulatory PC alone does not guarantee optimized utilization. Health systems with established outpatient PC, including for patients with advanced cancer, still struggle with adequate referrals, often owing to logistical barriers and perceived time cost to patients. 29 However, there is ongoing work examining solutions for expansion of access to PC in the outpatient setting, including enhanced delivery of primary PC by trained hepatology teams 30 and application of an embedded care model in which PC providers are colocated within a specialty hepatology clinic.31,32
Our study does suggest that the PC interventions were found to be of longitudinal benefit within our health system. Twenty-five patients were excluded due to having had first contact with PC prior to the study, representing patients who had PC consultation earlier in their disease trajectory. Furthermore, eight patients had PC contact across multiple hospitalizations during the study period. Importantly, while a substantial proportion of patients died or transitioned to comfort care following PC contact, nearly one quarter of the studied patients continued to seek life-prolonging measures even after PC referral, in that they did not transition to comfort care, did not engage with hospice, and lived to hospital discharge. These consultation patterns seem to indicate that there is a perceived benefit of earlier PC referral at our organization, though systems-level factors still lead to later consults.
At our institution, we have developed an active relationship with our transplant hepatology colleagues, the cornerstone of which is the presence of a PC representative at the weekly LT PSC meetings. This collaboration has facilitated communication between the PC and LT teams and suggests an openness within our health system to earlier PC involvement. However, there were no statistically significant differences detected between the cohort of patients who received PC consultation before and after PC presence at transplant PSC. Although this may be related to small sample size, as reflected in broad confidence intervals, and the delay between a new intervention and practice patterns, it may also indicate that PC presence at PSC alone is not sufficient to independently change practice patterns and outcomes. In a large cross-sectional survey study, Ufere et al. found that a majority of surveyed hepatologists and gastroenterologists agreed that patients with ESLD should have access to PC and would benefit from PC delivered earlier in the course of their illness, but only a small number reported actively collaborating with these services for their patients. This reflects that sustained practice change will likely require a multipronged approach beyond simple recognition of the value of PC. 33
Even with increased attention to improving outpatient PC access, there will be considerable lag time before substantial changes to care are realized. Until robust outpatient PC is more widely available for ESLD patients, it is imperative to optimize existing inpatient care delivery models. Recent studies have proposed and examined triggers for PC consultation, with one study demonstrating increased PC utilization and increased ACP through triggered PC consultation when patients met at least two of the following criteria: Child-Pugh Class C cirrhosis, two or more liver-related admissions in the preceding six months, current alcohol use, and unsuitability for LT workup. 34 Other proposed triggers include recurrent decompensation-related readmissions,10,35 as well as MELD score ≥20 or inoperable HCC. 36 Future work is needed to examine the longer-term impact of these case-finding measures.
This study has limitations, namely that it was a descriptive retrospective observational study, was not powered at the outset, and may be underpowered to detect differences in the pre- and post-Pall groups. We attempted to standardize our manual chart abstraction to reduce subjectivity and inter-rater variability, and our data collection relied on accurate coding and documentation. Furthermore, death data were inconsistent and not always readily available. We reported on hospice referrals but were not able to confirm enrollment with hospice after hospital discharge. As this was a single-center study at a large academic LT center in the United States, these results may have limited generalizability. However, this study describes the experiences of one of the largest cohorts of its kind and builds upon the growing body of literature identifying the many unmet needs of this patient population. This work will serve as a foundation for future prospective studies aimed at identifying and addressing these unmet PC needs of ESLD patients earlier in the disease process.
Conclusions
This study of PC referral patterns and outcomes for patients with ESLD revealed that despite some evidence of acceptance of more upstream integration, most referrals occurred near EOL and were closely followed by a shift to comfort care. Late referrals may result from a lack of evidence-based guidance on optimal timing, as well as from limited access to outpatient PC, leading to reliance on inpatient consults during acute illness. The presence of a PC representative at PSC represents our evolving collaboration within the LT space but has not yet yielded evidence of direct impact on practice patterns. Effective integration of PC into the care of patients with ESLD will require sustained culture and practice shifts over time and will likely vary widely depending on the health system, culture, and care environment. Future studies should focus on the optimization of existing care structures and the development of novel models for the integration of PC into the care of this patient population.
Footnotes
Acknowledgments
The authors would like to thank the faculty and staff of the OSU Center for the Advancement of Team Science, Analytics, and Systems Thinking in Health Services and Implementation Science Research (CATALYST).
Authors’ Contributions
Each author approved the final submitted draft of the article. Study concept and design: B.L.W., J.A.B., L.A.F., and S.G.K. Data acquisition, analysis, and interpretation: B.L.W., A.R.K., J.A.B., S.E., L.J.R., J.L.E., H.L.M., and G.D.T. Drafting and critical revision of the article for important intellectual content: B.L.W., A.R.K., J.A.B., S.E., C.B., L.J.R., J.L.E., H.L.M., G.D.T., J.L.A., E.S., L.A.F., A.S.M., and S.G.K.
Author Disclosure Statement
The authors declare that they have no relevant financial relationships to disclose.
Funding Information
This project and publication were supported, in part, by Award Number UM1TR004548 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center for Advancing Translational Sciences or the National Institutes of Health. The project described was also supported by the Ohio State University College of Medicine Center for Faculty Advancement, Mentorship, and Engagement FAMEPRO clinical scholarship program.