
Abstract
Children with non-curative brain tumors have a predictable and burdensome neurological decline. Care provision for these children falls in the gap where the acute inpatient services intersect with community-based providers. These children commonly receive care in the community; however, their neurological decline often outpaces engagement with community-based providers. Children with non-curative brain tumors are commonly referred to specialist palliative care services and need timely availability and access to this support. The purpose of this scoping review was to explore the evidence related to standards, guidelines, and models of palliative care provision for children with non-curative brain tumors, and to examine the facilitators and barriers to the implementation of, and access to, these services. Using a narrative synthesis method, a scoping review was conducted according to the Joanna Briggs Institute methodology using six electronic databases (Medline, Embase, Web of Science, Pubmed, CINAHL, and Cochrane Database of Systematic Reviews) from January 2013 to May 2023. A total of 2404 studies were screened for eligibility and 31 were selected for data extraction. There are no international models or standards of care for providing palliative care for children with non-curative brain tumors. Instead, palliative care is delivered at an institutional level, potentially leading to variability in the care that is provided. This variability can threaten the quality of life of these children and their families. Variability in care provision could be minimized by development of standardized palliative care provision. Any proposed standard for palliative care provision for children with non-curative brain tumors should include early integration of palliative care, and allocation of resources to enable training to operationalize referrals to palliative care teams and multidisciplinary care provision across settings, especially home-based care.
Introduction
Brain tumors are the second most common pediatric malignancy and the leading cause of cancer-related death in children.1–3 The prognosis of pediatric brain tumors depends on various factors including tumor type, stage, site, age at diagnosis, and when treatment, if any, was commenced. 4 Diffuse midline gliomas account for 10%–20% of all pediatric brain tumors 5 and are the most aggressive primary brain tumors associated with the highest mortality rate.6–8 Despite global efforts to investigate the efficacy of different therapies, there remains a lack of curative therapeutic modalities rendering them non-curative with significant symptom burden.9,10
Pediatric brain tumors impose a high disease burden on both children and their families. 11 For non-curative brain tumors such as diffuse midline glioma, children can experience a predictable and marked neurological decline as the tumor progresses. 12 This includes difficulties with mobility and communication, altered consciousness, dysphagia, and breathing difficulties as the child nears the end of their life. 12 Parents of children with non-curative brain tumors must witness and attend to their child’s increasing medical and psychosocial needs with this neurological decline and do so, mostly in an outpatient community setting.11,13 Parents are also faced with additional responsibilities such as simultaneously caring for other children, working and managing finances contributing to often immense distress among parents.11,13
In order to optimize the quality of life of children with such life-limiting conditions and their families, referral to a specialist pediatric palliative care service is recommended. 14 Despite the recognized benefits of palliative care services, 15 they remain underused, with some studies reporting an uptake of less than 50%.16–19 There also remain ongoing reports of unmet emotional and prognostic informational needs of children and caregivers.20,21
Timely access to palliative care for children with non-curative brain tumors can be challenging. This is because children with non-curative brain tumors face a unique disease trajectory: there is often a delay in diagnosis in a previously typically developing child, with the progressive global deterioration occurring largely in an outpatient community-based setting, leading to a poor quality of life.12,22 Children with diffuse midline gliomas have an overall median survival of less than one year, even with the use of radiotherapy.9,23–25 This means that the pace of their decline is faster than for children with primary non-malignant conditions who usually have established community-based providers but slower than for children with other advanced cancers, where support is commonly provided by acute health services. Children with non-curative brain tumors and their families find themselves in a gap. After the initial diagnostic period in an inpatient acute health setting, they are primarily cared for in outpatient community-based settings; they rely on allied health supports that shift from being provided in the inpatient acute health settings to the community-based sector with respect to care provision and funding. 26 The intersection between these two sectors can be particularly difficult to navigate.
Children with non-curative brain tumors usually do not have established relationships with allied health (e.g., occupational therapy, speech therapy, physiotherapy, social work, dietetics, psychology, child life therapy) providers in the community as their premorbid level of functioning is usually within the typically developing range. Further, their functional impairment and evolving disability changes and often outpace the response of the community services. As a result, there is a significant risk that these children will have unmet functional needs despite predictable evolving needs that impact their overall quality of life.
There is a paucity of information about current practices of palliative care specific to non-curative brain tumors where there is a time-pressure to navigate this intersection between acute inpatient and community-based allied health providers. Research to date has explored the experiences of these children, their place of death or broadly discussed palliative care, however, no studies have reported on models of palliative care for children with pediatric non-curative brain tumors.11,27–31 Standards, guidelines, and models of care provide clarity about roles and responsibilities and promote timely, streamlined, and consistent care provision that can address the challenges experienced by children with non-curative brain tumors. 32
The primary objective is to review the literature on standards, guidelines, and models of palliative care for children with non-curative brain tumors. This review will focus on the supportive care and non-medication based symptom management component of palliative care. The secondary objective is to explore the facilitators and barriers to establishing, delivering, and accessing palliative care services for this population.
Methods
The review was conducted in accordance with the Joanna Briggs Institute scoping review methodology. 33 This framework comprises four stages as outlined below and the study protocol was published in Figshare. 34
Search strategy
Medline, Embase, Web of Science, Pubmed, CINAHL, and Cochrane Database of Systematic Reviews were searched. The Medline search strategy, including all identified keywords, was adapted for each included database (see Supplementary Tables S1 and S2). Studies published from January 2013 to May 2023 were included. Non-English studies were excluded. Materials not formally published in academic journals, such as government reports and guidelines (gray literature) were searched on Guideline Central 35 and The National Institute for Health and Care Excellence. 36 Google Scholar was searched using Harzing’s Publish or Perish software program 37 and the first 200 publications from January 2013 to September 2023 were retrieved.
Eligibility criteria
The inclusion criteria were: (i) articles relating to children and adolescents between the ages of 0–18 years; (ii) sources of evidence published worldwide between January 2013 to September 2023; (iii) articles that explored standards or models of palliative care, guidelines/recommendations, barriers, and/or facilitators to providing and accessing palliative care services for pediatric non-curative brain tumors; and (iv) articles in which the reported experiences of patients/parents/health care professionals included facilitators and barriers to the provision of and access to palliative care services for pediatric non-curative brain tumors. The exclusion criteria were: (i) articles that only included an adult population (over the age of 18 years); (ii) non-English articles; (iii) articles that included general palliative care with no specific mention of non-curative brain tumors; and (iv) articles that only included medication-based symptomatic management in palliative care.
Study selection
All identified citations were collated and uploaded initially onto Endnote 20, 38 and then Covidence.39,40 After the removal of duplicates, titles, abstracts, and full texts were screened by two independent reviewers (M.B. and P.S.) against the inclusion and exclusion criteria. The titles and abstracts of the references of the articles that were selected for data extraction were also screened and the full texts of any mutually selected studies were screened for selection for data extraction. Any disagreements during the selection process were discussed and resolved by consensus agreement.
Data extraction
M.B. and P.S. extracted data using a tool developed by the research team (see Supplementary Table S3). Data included information about study participants, concept, and context, as well as the key findings for each study that were relevant to the objectives of this review.
Data analysis and presentation
Data were descriptively analyzed and are presented graphically or in a tabular form.
Results
Study characteristics
As illustrated in Figure 1, the search strategy elicited 4561 articles. Following the removal of duplicates, 2404 underwent title/abstract screening, of which 2004 articles were excluded. A further 369 articles were excluded in full text screening due to: insufficient details (n = 36), adult patient population only (n = 45), palliative care was not specific to non-curative brain cancers (n = 249), focus was medication-based symptom management component of palliative care (n = 29) or an English translation was not available (n = 10).
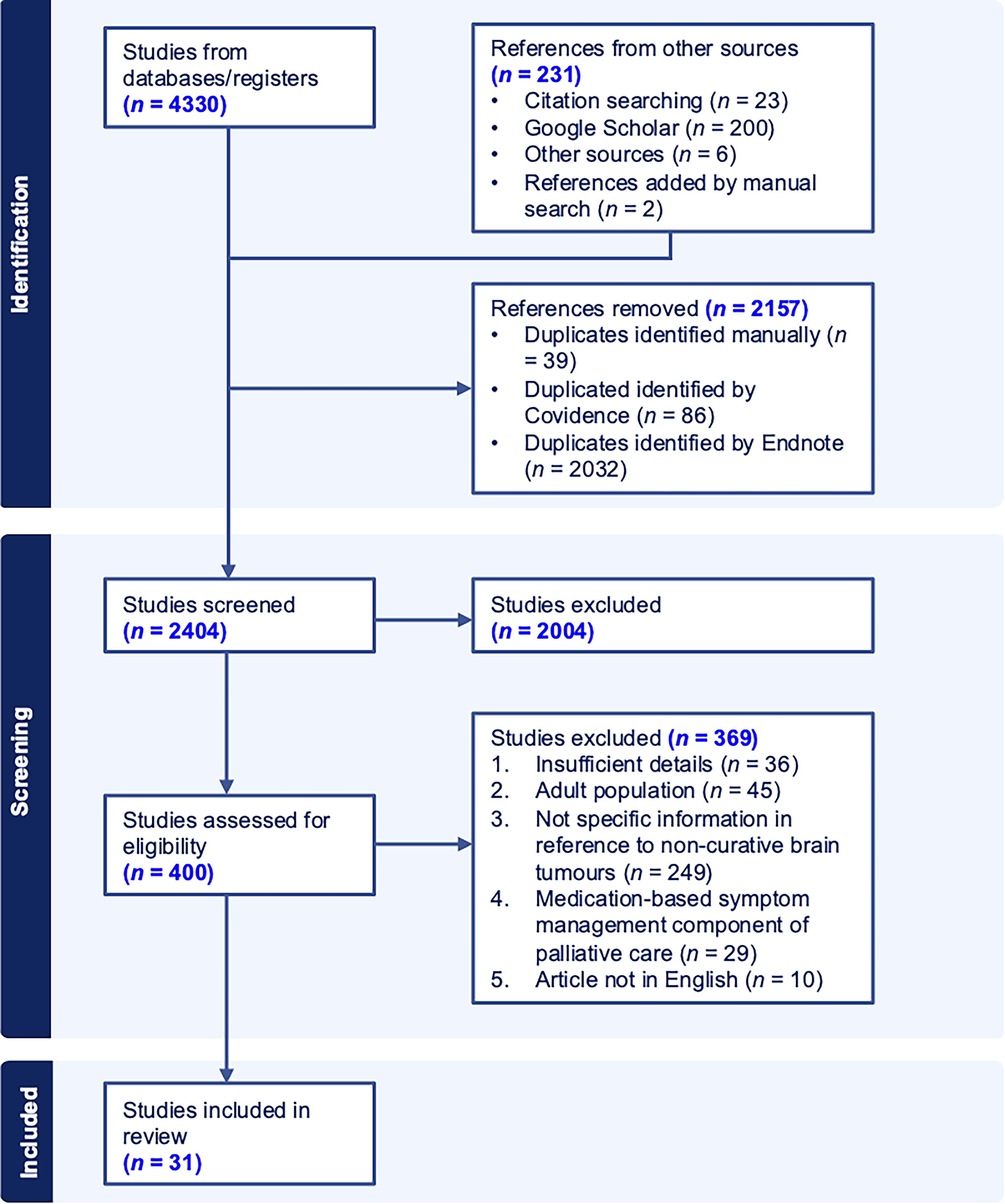
Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram for the selection process.
Supplementary Table S4 illustrates the study characteristics. Of the 31 articles, 15 were observational studies.12,14,21,38,41–51 The study design was not specified for two studies which were a journal abstract and a book chapter.52,53 Most of the studies were based in the United States (n = 15).14,41,44,49,50,54–62 See Supplementary Table S5 for population characteristics.
Members of the palliative care team
Seven of the studies were narrative reviews and did not involve health care professionals.54,55,58,59,62–64 Of the remaining 24 studies, 18 specified the types of clinicians involved in the delivery of palliative care (Fig. 2).12,14,21,41,42,45–48,50,54–57,61,64–66 Of the health care disciplines, allied health was most frequently involved while nursing was least frequently involved.12,21,41,42,46,48,50,54–57,61,64–66 When a frequency count of the types of health care professionals was performed, physician/neurologist/neurosurgeon/pediatrician were most frequently mentioned in the delivery of palliative care.45,46,48,50,54–56,61,65 Of the allied health care professionals, social workers were most frequently mentioned.21,41,46,50,54,55,65,66 One study mentioned the involvement of a palliative care team but did not specify the types of health care professionals that were involved. 42
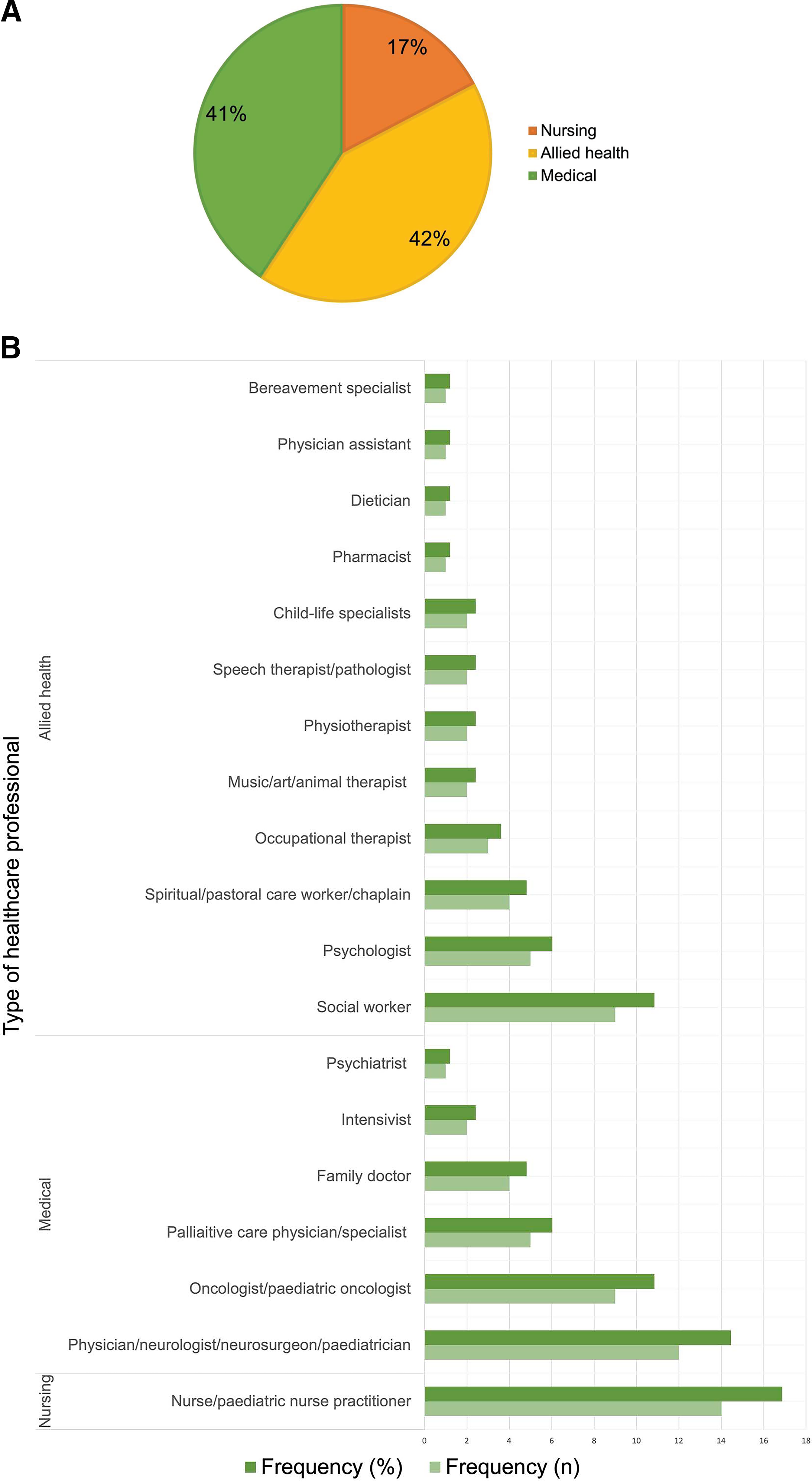
Health care professionals involved in the delivery of palliative care.
Palliative care models
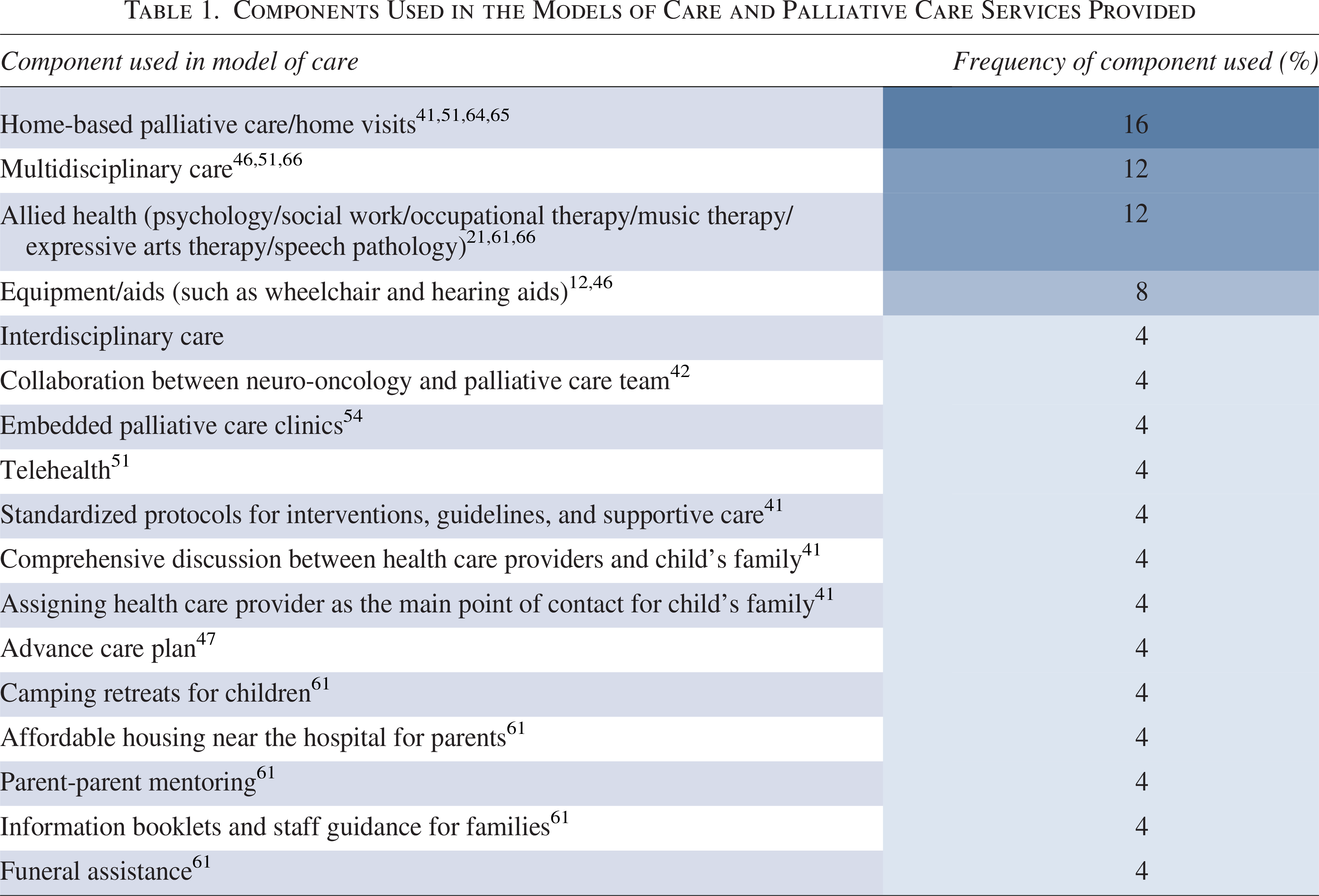
Thirteen of the 31 studies reported a model of care, an end-of-life program, and/or palliative care services that were provided.12,21,41,42,46,47,51,54,55,61,64–66 These models of care, programs, and services comprised of different components (Table 1), with home-based palliative care or home visits by the health care staff being the most frequently reported component.41,51,64,65
Components Used in the Models of Care and Palliative Care Services Provided
Barriers and facilitators to establishing and accessing models of care
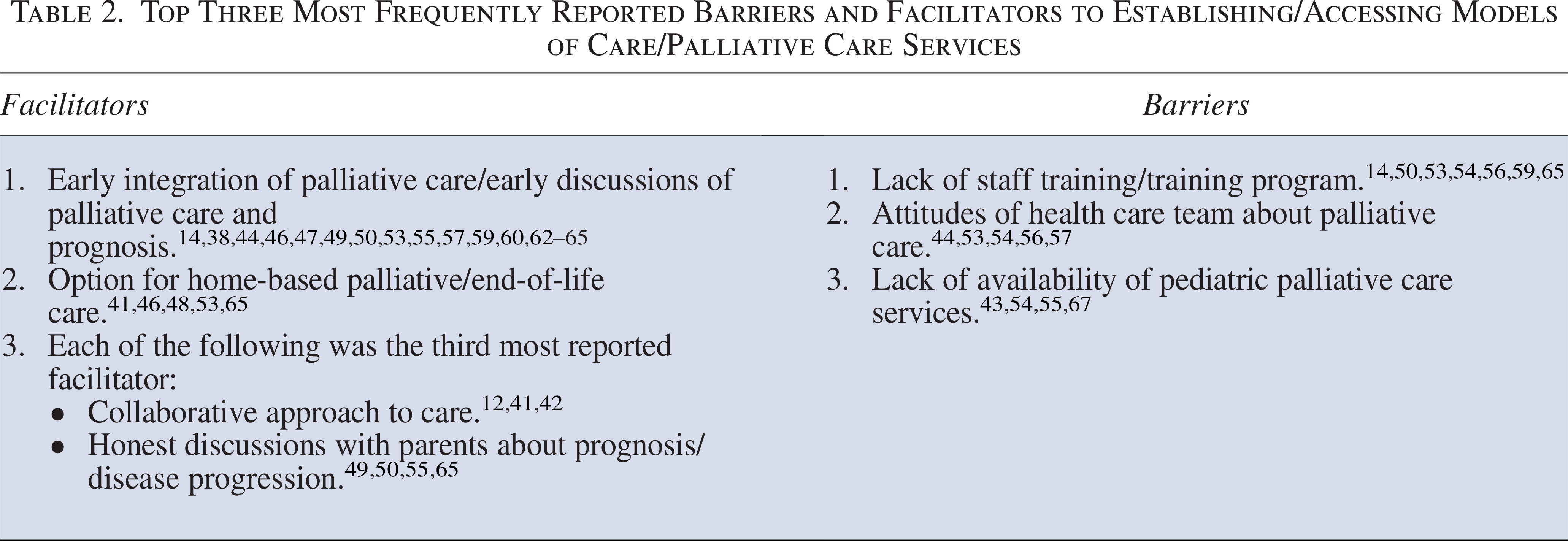
Twenty-eight of the 31 studies reported barriers, facilitators, or both, to establishing and/or accessing models of care and/or palliative care services (Supplementary Table S4).12,14,21,38,41–44,46–50,52–57,59–67 Early integration of palliative/end-of-life care and discussions about prognosis, palliative care and/or end-of-life care was the most frequently reported facilitator (Table 2).14,38,44,46,47,49,50,53,55,57,59,60,62–65 Lack of staff training/training programs was identified as the most frequently reported barrier (Table 2).14,50,53,54,56,59,65
Top Three Most Frequently Reported Barriers and Facilitators to Establishing/Accessing Models of Care/Palliative Care Services
Guidelines/recommendations for establishing standards of care
Twenty of the 31 studies provided guidelines and/or recommendations for establishing standards of care (Supplementary Table S4).12,14,21,38,44,46,48–62,65–67 The most frequently reported guideline/recommendation was a collaborative approach by health care professionals, interdisciplinary and/or multidisciplinary care.49,50,53,58,59,65,66
Discussion
This scoping review is the first to explore international literature to identify the models and standards of palliative care available for children with non-curative brain tumors.
Main findings
In line with recommendations from the World Health Organization on palliative care, 68 a multidisciplinary approach and specifically the involvement of allied health was one of the most used components of palliative care for children with non-curative brain tumors.21,46,51,61,66 The benefits of multidisciplinary collaboration are well-known69–74 and our review indicates that implementation of multidisciplinary palliative care for children with non-curative brain tumor is institution-specific with the composition of disciplines providing palliative care varied between institutions.12,41,42,45,51,66 A child with a non-curative brain tumor may be referred to a palliative care team at one institution, where team members have a completely different composition of disciplines compared to if they were referred to a palliative care team at another institution; there is currently a lack of established national and international standards and models of care for this care provision.
Institution-specific implementation leads to variability in the provision of palliative care services12,41,42,45,51,66,75; any child with palliative care needs may receive different services depending on the institution they attend rather than based on their needs. The impact of this variability is brought into sharp relief for children with non-curative brain tumors. For this cohort, their neurological decline across the cognitive, communication, and motor domains is slower than for children with other advanced cancers, but quicker than children with non-malignant conditions, and their care is predominantly in the community with a degree of time-pressure to refer to community-based allied health providers. Variation in palliative care provision may leave these children vulnerable to not being able to access community-based allied health services in a timely manner. The risk that their changing needs outpaces engagement of community-based providers may hinder the opportunity to enhance their quality of life. Services for these children and their families must be responsive and resourced to meet their changing functional needs. These potential challenges can be addressed by the development of a standard of care incorporating features that this review has identified. In what follows is discussion about features that should be included in a standard for palliative care provision for children with non-curative brain tumors.
A proposed standard for palliative care provision for these children should include an early introduction to palliative care.14,38,44,46,47,49,50,53,55,57,59,60,62–65 Early introduction to palliative care could be achieved through routine referral to palliative care services at time of diagnosis. 67 This approach avoids delays which is imperative for children with non-curative brain tumors due to their short life expectancy.8,76 However, there remains discrepancy between introducing palliative care to families and making a referral to a palliative care team: while most clinicians mention palliative care at the time of a child’s diagnosis of diffuse midline glioma, 77 several studies reported late referrals to palliative care teams.14,38,53 The reason for this discrepancy may relate to the common barriers to establishing models of care identified in this review. Specifically, a lack of clinician comfort or confidence in operationalizing the referral to a palliative care team, and/or the availability of pediatric palliative care services.
Surprisingly, clinicians caring for children with non-curative brain tumors continue to describe negative perceptions surrounding palliative care,54,56,57 with ongoing fears that early referral to palliative care teams will increase parental distress.56,57 This is despite the well-known positive attitudes of parents toward an early introduction to palliative care teams.75,78 Parental preferences are clear: they prefer early, honest, and reciprocal communication79–81 about disease prognosis and progression.49,50,55 If this is provided, parents are accepting of referral to palliative care teams. 75 However, there remains a lack of trained staff to have these honest sensitive conversations,54,65,75,82 with no evidence-based curriculum on how to train health care students on engaging in difficult conversations.56,61 The need for communication skills training to address difficulties in communicating about palliative care is known prompting development of communication skills training programs.56,57 However, the impact of such training programs on operationalizing referrals to palliative care teams remains unknown.
Lack of availability of palliative care services and limited resources and infrastructure are other frequently reported barriers related to establishing a model of care for palliative care provision for children with non-curative brain tumors.43,54,55,67 This included lack of health care and administrative staff, financial resources, and the availability of a clinic space.54,59 To address this, Massie et al. 14 proposed prioritizing referrals based on needs rather than at the time of diagnosis, however, this may challenge the benefits of early and standardized referrals to palliative care which minimizes delays in accessing this service. Alternatively, Brock et al. 54 proposed collaboration within institutions to share resources through a dual-consultation model in which palliative care physicians consult alongside oncologists in order to use the existing oncology clinic space and administrative staff alongside other resources. 54 However, while there are benefits to this collaborative care, it localizes palliative care input within the outpatient clinic rather than enabling home-based care.
This review identified that pediatric palliative care teams should be resourced to provide ongoing reviews of children with non-curative brain tumors across inpatient and community-based settings, with the ability to flex their involvement given the dynamic and rapidly evolving needs of these children over a timeframe that often outpaces engagement with other community-based allied health services. Importantly, being able to provide end-of-life care at home was one of the three most frequent facilitators to establishing/accessing models of care and palliative care services.41,46,65 This aligns with literature describing home as the preferred location of end-of-life care for many families.15,77,83–86 While palliative care is not limited to the provision of end-of-life care, facilitating a child’s care at home has demonstrated benefits of reduced stress levels for families, ability for siblings to attend school, improved quality of life of patients, and reduced caregiver burden.15,77,83 For children with non-curative brain tumors, successful care at home often involves the prescription and supply of specialized equipment for personal care, communication, and functional independence. This adaptive equipment is needed before the child approaches their end of life and needs continuous review and adaption over a short period as they continue to decline. This clinical reassessment relies on outpatient and community-based therapists as these children often remain at home through this decline.
Home-based care can be facilitated by palliative care review in embedded clinics, free-standing clinics, home visits, and via telehealth.41,54,64,65 The Pediatric Advanced Care Team at Boston Children’s Hospital is an example of a floating pediatric palliative care model that can support children and families who prefer care at home. 54 The Pediatric Advanced Care Team comprises two pediatricians, two social workers, pediatric nurse practitioners, and nurses who provide inpatient and outpatient services as well as home consultations. 54 The ability to access the Pediatric Advanced Care Team in different settings means that the necessary support and skills needed for effective palliative care for end-of-life care at home can be delivered. 77 Indeed, the identification of home-based palliative care as the most frequently reported component of the models and services of palliative care suggests that this is a feasible and effective approach.41,51,64,65 However, we note that this team does not include clinicians who can prescribe or supply the specialized equipment children with non-curative brain tumors need before they approach their end of life.
To help resource palliative care teams, it is necessary to clarify the role of clinicians in the provision of palliative care for children with non-curative brain tumors. Although this review identified what health care professionals are involved in the provision of palliative care for children with non-curative brain tumors, only one study detailed the role of the clinicians. Arland et al. 41 clearly described two clinicians were involved in reviewing the child’s care plan, an outpatient nurse was assigned the task of contacting the family on a weekly basis and a pediatric nurse practitioner was responsible for liaising with the hospice nurse and hospice pharmacy to discuss the use of intravenous medications for the child. By detailing the roles of each clinician, resources can be assigned accordingly which can not only avoid delays in the delivery of care but can also increase efficiency, ensure correspondence can be made, and allow for outstanding tasks to be followed up appropriately. Greater transparency of established models of care will enable evaluation and benchmarking to maximize the efficiency and quality of this care.
Strengths and limitations of the review
This review included global literature to help shed light upon the standards and models of care utilized in different settings, however, caution must be exercised in extrapolating these findings. Most of the studies were based in North America41,50,54,56,57,59,61,62,67,75,78,87 so findings may only be relevant to high-resource countries. Factors such as similar socioeconomic status, resources, hospital facilities, and public and private health care across these high-income countries allow for this.88–90 However, it is important to recognize that even in this context, there may be differences within and between high-income countries in how health care is delivered more generally. 91 This may include service funding structures, such as government or private funding, which can influence the applicability of findings within different health services as well as limiting the development and implementation of national standards and models of care. 91 We recognize that due to limited resources and accessibility, establishing palliative care services might be challenging in low-income countries. 68 To better understand the extent of global current practices, more evidence-based benchmarking is needed on how care is provided in different settings such as socioeconomic differences, city versus regional/rural accessibility, and private versus public health care systems. Further studies are also required to establish the efficacy of implemented models of care. This is especially important considering all studies were qualitative and did not include validated measures of the reported outcomes or the efficacy of the reported data.12,14,21,38,41–67
What this study adds
This review identified that provision of palliative care for children with non-curative brain tumors is largely institutionally driven and that the lack of standardized protocols and guidelines threatens timely and effective palliative care provision.12,14,21,38,41–67 Identification of the most frequently utilized components of palliative care in this population can help guide clinicians and policymakers to develop models, standards and guidelines of palliative care for children with non-curative brain tumors. Importantly, resources are required to develop and evaluate communication skills training to help operationalize referrals to palliative care teams, so that palliative care services can provide care both in acute health and community-based settings; this care needs to be responsive to the dynamic and changing needs for children with non-curative brain tumors which often outpaces engagement with other community-based providers.
While children with non-curative brain tumors were our population of focus, the findings of this scoping review may be relevant to a broader group. These findings may be applicable to any patient population that has palliative care needs and evolving disability regardless of diagnosis, who have care provided at the intersection between inpatient and community-based providers, and where timely access to palliative care services is challenging.
Conclusion
This scoping review revealed that there are no international or national models of care or guidelines to standardize the provision of palliative care to children with non-curative brain tumors. As a result, there is a variability in the level of and type of palliative care services that are delivered between institutions. Benchmarking current practices of palliative care provision in different settings is the next step to enhancing the sources for evidence thereby providing the opportunity to conduct quality assessment of evidence through systematic reviews. Future research should explore the outcomes of palliative care models that have integrated the most frequently reported facilitators to inform clinicians of their utility in practice. Evaluating the efficacy and outcomes of current models will help inform the much-needed standards of care for children with non-curative brain tumors and their families.
Authors’ Contributions
M.B., S.R., P.S., M.M., and S.V. conceptualized the study. M.B. and P.S. conducted the search, including screening, data extraction, and reporting of the findings. M.B. wrote the first draft of the article. All authors contributed to revision and editing and approval of the final submitted version. All authors accept responsibility for the decision to submit for publication.
Footnotes
Acknowledgment
The authors would like to collectively acknowledge Poh Chua, Librarian at The Royal Children’s Hospital, for her expertise and time in guiding this review.
Author Disclosure Statement
The authors declare that there is no conflict of interest.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. M.M. is supported by a Victorian Cancer Agency Fellowship.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.