
Abstract
Background:
Utility values of responders and nonresponders are essential inputs in cost-effectiveness studies of radiation therapy for painful bone metastases but, to our knowledge, they have not been reported separately.
Objective:
We sought to determine the utility values of responders and nonresponders using data from a prospective observational study on bone metastases.
Methods:
The original prospective observational study was conducted at 26 centers in Japan. Of 232 enrolled patients, 181 whose pain scores at baseline were ≥2 were analyzed. Health-related quality of life (QOL) was measured using the EuroQol 5-dimensions 5-levels (EQ-5D-5L) instrument at baseline and 2- and 6-month follow-up assessments. At follow-up assessments, patients were categorized as responders or nonresponders. Pain response was assessed using the International Consensus Pain Response Endpoints.
Results:
Of the 181 patients analyzed, 133 (73%) and 84 (46%) were evaluable at the 2- and 6-month follow-up assessment, respectively. The EQ-5D-5L index score (utility) increased from baseline to the 2- and 6-month follow-up assessments; regarding opioid analgesic use, no clear trend was observed during the same period. The mean utility was significantly higher in responders than in nonresponders at both follow-up times. The mean daily oral morphine equivalent dose was significantly lower in responders than in nonresponders at both follow-up times.
Conclusion:
We determined utility values for responders and nonresponders. Pain response was associated with better QOL and less opioid use. Our utility values according to response status can be used for model input in future cost-effectiveness studies on radiation therapy for bone metastases.
Introduction
Bone metastases are associated with several morbidities, among which pain is well managed with radiation therapy. 1 Palliative radiation therapy is a standard treatment for painful bone metastases. 2 It relieves pain, 3 preserves or improves function, 4 and improves health-related quality of life (QOL),5,6 whereas it has limited toxicity. 7 The benefit of radiation therapy for painful bone metastases must be balanced with its associated increased cost. Cost-effectiveness is a major issue in palliative radiation therapy as well as in other areas of medicine. 8 The incremental benefit in cost-effectiveness analysis is frequently measured by quality-adjusted life-years (QALYs). 9 QALY is a measure that captures two features of health care interventions: survival and a specific type of QOL, utility. As palliative radiation therapy, in general, is not expected to prolong survival, 8 the potential incremental benefit of palliative radiation therapy may be solely due to the improvement in utility. The incremental cost-effectiveness ratio (ICER) is a statistic that summarizes the cost-effectiveness of an intervention compared to a control intervention. The ICER of an intervention, when QALY is used as a measure of effectiveness, can be interpreted as the incremental cost needed to obtain one additional QALY.
In cost-effectiveness studies of radiation therapy for painful bone metastases, patients with (i.e., responders) and without (i.e., nonresponders) pain response (i.e., pain reduction) should be assigned different utility values.10–14 Patients who receive radiation therapy, of whom approximately 60% have a response, 3 obtain benefit in utility from the therapy, while those who do not receive radiation therapy naturally do not obtain such benefit. For the analysis of this additional benefit of radiation therapy, utility values for responders and nonresponders are essential model inputs. In Markov models, frequently used in such studies,11–14 model inputs including utility values are mostly cited from published papers.11–13 In past studies on radiation therapy for painful bone metastases, utility values for pain responders and nonresponders were derived from,11,12 or traced back to, 13 a 2003 paper that studied a subset of patients with painful bone metastases in a Dutch randomized controlled trial. 15 In that 2003 paper, however, utility values seemed to be presented for patients who were both responders and nonresponders. 15 In another study that employed a Markov microsimulation model, survival was weighted using disability weights instead of utility values. 14 The disability weight for nonresponders was derived from the Global Burden of Disease study 16 for chronic low back and leg pain from musculoskeletal disorders; half of this value for nonresponders was assumed to be the disability weight for responders. 14 To summarize, utility values (or disability weight) for model input have been derived from data on patients who were both responders and nonresponders or derived from data on patients with other diseases. To our knowledge, utility values for responders and nonresponders to radiation therapy for painful bone metastases have not been reported separately to date. Our aim in this study (a secondary analysis of a previously published prospective observational study17,18) was to determine utility values according to response status.
Methods
Patients
The original prospective observational study was conducted at 26 centers, as previously reported.17,18 The original observational study had several objectives that included the clarification of the income and employment status of patients who received palliative radiation therapy, 17 the investigation of patient/treatment characteristics in current palliative radiation therapy practice, 18 and the study of QOL before and after radiation therapy. The present study was another preplanned analysis from the original observational study. Inclusion criteria in the original study were presence of (1) signed informed consent and (2) planned radiation therapy for bone metastases; the only exclusion criterion was being deemed unsuitable for participation by the treating physician. Between December 2020 and March 2021, 333 patients received radiation therapy for bone metastases (including painful and nonpainful bone metastases) at the participating centers, of whom 232 (70%) were enrolled in the study (Fig. 1). Of the 101 excluded patients, 11 (11%) refused to participate; the attending physician determined that the performance status of 68 (67%) was not good enough for the 6-month follow-up assessment; 13 (13%) patients with good performance status were not fit for the follow-up assessment; and 9 (9%) needed to start treatment before receiving an explanation about the study. 17 After further excluding 5 ineligible patients, 1 patient who withdrew from the study, 2 patients who did not receive the planned radiation therapy, 35 patients whose pain score at baseline was <2, and 8 patients for whom the EuroQol 5-dimensions 5-levels (EQ-5D-5L) data were missing at baseline, a total of 181 patients with painful bone metastases were included in the present analysis (Table 1). The sites of irradiated bone metastases (n = 248) were the spine (n = 124; 50%), pelvis, (n = 51; 21%), femur (n = 23; 9%), ribs (n = 14; 6%), humerus (n = 6; 2%), and other (n = 30; 12%). Among the 181 patients analyzed, the irradiated bone metastases were previously treated with surgery in 18 (10%) patients; unfortunately, however, the details of the surgeries were not collected. Bone metastases were treated with radiation therapy in 21 (12%) patients. The original prospective observational study was approved by the institutional review boards of the participating centers, and written informed consent was obtained from all patients. The study was registered with the University hospital Medical Information Network Clinical Trials Registry (URL: https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000048504) with the identification number UMIN000042491.
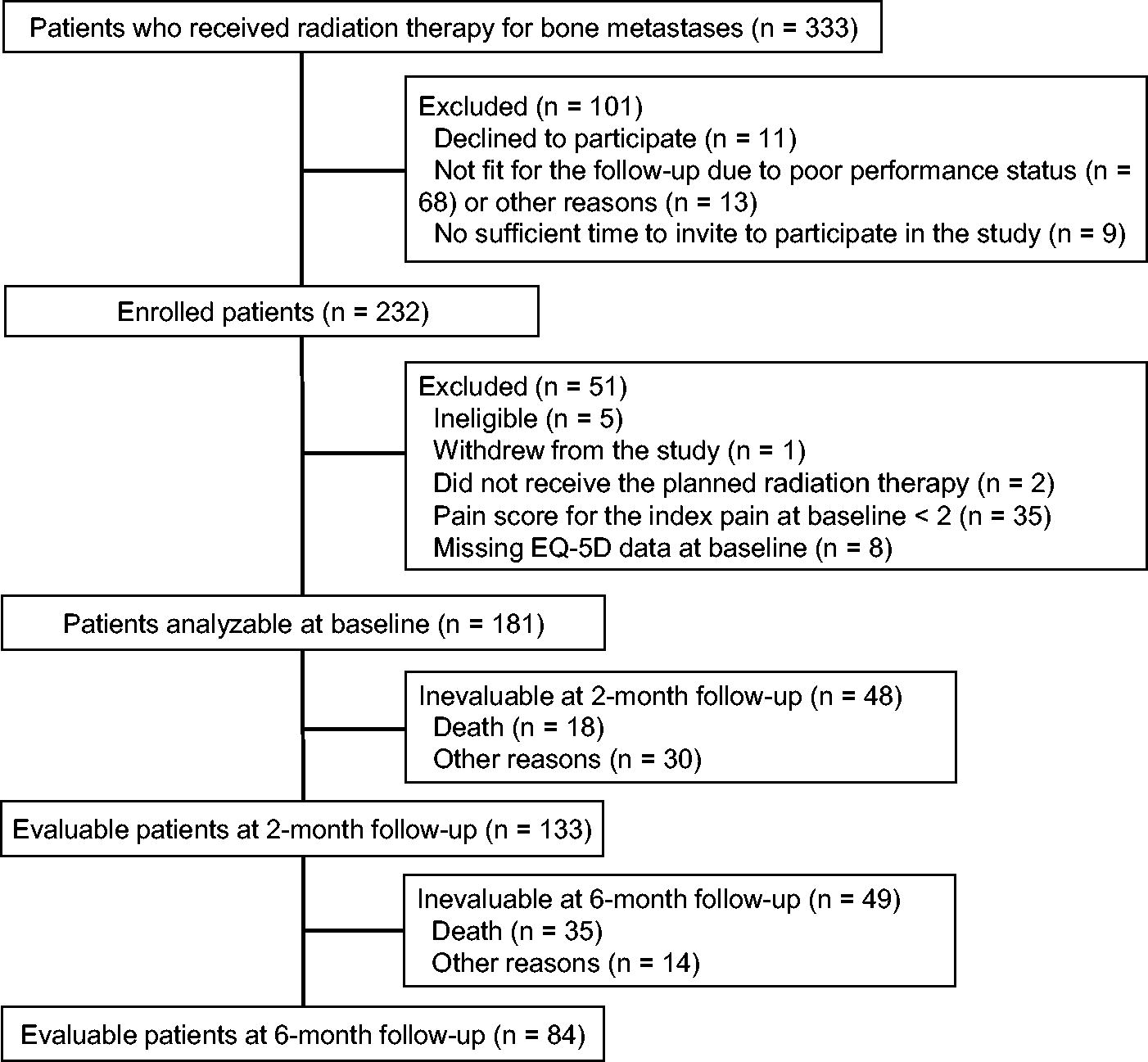
Flow diagram of the study cohort. Inevaluable status at 2 and 6 months was defined as at least one value of the five dimensions of the EQ-5D-5L being missing at such follow-up assessments.
Baseline Patient and Treatment Characteristics (n = 181)
Inevaluable status was defined as at least one value of the five dimensions of the EQ-5D-5L being missing.
Comparisons between evaluable and inevaluable patients were performed with the Wilcoxon rank sum test or the Fisher exact test.
P values were less than the Bonferroni-adjusted significance level of 0.0055 (0.05/9 characteristics tested).
SD, standard deviation; IQR, interquartile range; ECOG, Eastern Cooperative Oncology Group; NRS, numeric rating scale.
Evaluation
Utility was measured using the EQ-5D-5L at enrollment, 2-month follow-up assessment, and 6-month follow-up assessment. The EQ-5D-5L is a brief measure of health; the self-completion version was used for our study. 19 The EQ-5D-5L instrument consists of two parts: a descriptive classification system and a visual analogue scale (EQ VAS). 19 The EQ-5D-5L descriptive system comprises five health dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. Each dimension has five response levels of severity: no problems, slight problems, moderate problems, severe problems, and extreme problems. Patients are asked to indicate their health state by checking the box next to the most appropriate response level for each of the five dimensions. When more than one of the boxes was checked for a single dimension, the value for the dimension was treated as missing. 19 The responses for the five dimensions are combined into a 5-digit number describing the respondent’s health state (from ‘11111’ indicating no problems on any of the five dimensions to ‘55555′ meaning extreme problems) in all dimensions. 20 The responses for the five dimensions are converted into a single summary index score, called utility, on 0–1 scale, where 0 means death and 1 means perfect health. This conversion is based on the Japanese version of the EQ-5D-5L value set. 21 This value set reflects the preferences of the general population in Japan. The EQ-VAS is a vertical visual analogue scale where patients are asked to indicate their overall health on the day of questionnaire completion. The EQ-VAS scores are anchored on 100 (the best health you can imagine) and 0 (the worst health you can imagine).
Patients rated the intensity of their worst pain in terms of the index pain (the pain caused by the irradiated tumor) over the previous three days using an 11-point (0–10) numeric rating scale. Opioid analgesic consumption was recorded as the daily oral morphine equivalent dose at the participating centers. The pain response was assessed using the International Consensus Pain Response Endpoints (ICPRE). 22 Using the ICPRE, patients who received radiation therapy for painful bone metastases were categorized as responders or nonresponders. Responders included patients who experienced complete or partial responses. A complete response was defined as an index pain numeric rating scale score of 0 with no concomitant increase in the oral morphine equivalent dose. 22 A partial response was defined as a reduction of the index pain numeric rating scale score of ≥2 without an increase in analgesic use, or a reduction in analgesic use of 25% or more from the baseline without an increase in the pain score. Nonresponders included patients who experienced pain progression or indeterminate response. Pain progression was defined as an increase in the index pain score of ≥2 without reduced oral morphine equivalent dose, or an increase of 25% or more in the oral morphine equivalent dose without a decrease in the pain score. An indeterminate response was defined as any response not captured by the complete response, partial response, or pain progression definitions. 22
Statistical analysis
Baseline patient and treatment characteristics were presented according to whether the utility score was available at the two-month follow-up assessment. We dichotomized ECOG performance status (0, 1 versus 2, 3, 4) and the numeric rating scale index pain score (≥8 vs. ≤7)23,24 in tests comparing evaluable and inevaluable patients. The Wilcoxon rank sum test was used for continuous variables, and the Fisher exact test was used for categorical variables. All tests were two-tailed. Bonferroni correction was used to account for multiple comparisons. In the comparison of evaluable and inevaluable patients, P values less than the significance level of 0.0055 (0.05/9 characteristics tested) were considered significant. In the comparison of responders and nonresponders, P values less than the significance level of 0.0125 (0.05/4 variables tested at each follow-up assessment) were considered significant. Statistical analyses were performed with R version 4.2.2.
Results
Patients
Of 181 patients analyzed, 133 (73%) and 84 (46%) patients were evaluable at the 2- and 6-month follow-up assessments, respectively (Fig. 1). Baseline patient and treatment characteristics are shown in Table 1. Comparisons of evaluable and inevaluable patients showed that patients with worse performance status and those using more opioid analgesics at baseline tended to be inevaluable at 2 months (Table 1).
EQ-5D, responses, and opioid analgesic use
Distribution of EQ-5D-5L responses at baseline and follow-up assessments are shown in Table 2. Values of each of the five dimensions showed that patients tended to have less severe problems at follow-up assessments than at baseline. The EQ-5D-5L index score (utility) increased from baseline to the 2- and 6-month follow-up assessments; regarding opioid analgesic use, no clear trend was observed during the same period (Table 3, Fig. 2). Pain response (i.e., complete response or partial response) was confirmed in 70 (53%) of the 133 evaluable patients and 50 (60%) of the 84 evaluable patients at the 2- and 6-month follow-up assessments, respectively (Table 3). The EQ-5D-5L index score was significantly higher in responders than in nonresponders at both follow-up times (Table 4). Regarding the 70 responders at the 2-month follow-up, the mean EQ-5D-5L index score (utility) was 0.70 (median, 0.72; standard deviation, 0.24; interquartile range, 0.51–0.89) in 30 patients with a complete response and 0.69 (median, 0.72; standard deviation, 0.21; interquartile range, 0.60–0.84) in 40 patients with a partial response. The daily oral morphine equivalent dose was significantly lower in responders than in nonresponders at both follow-up times (Table 4). For the 70 responders at the 2-month follow-up, the mean daily oral morphine equivalent dose was 4.4 (median, 0.0; standard deviation, 13.8; interquartile range, 0.0–0.0) in 30 patients with a complete response and 16.9 (median, 0.0; standard deviation, 57.4; interquartile range, 0.0–15.0) in 40 patients with a partial response. Regarding the use of bone-modifying agents and steroids, there were no differences between responders and nonresponders.
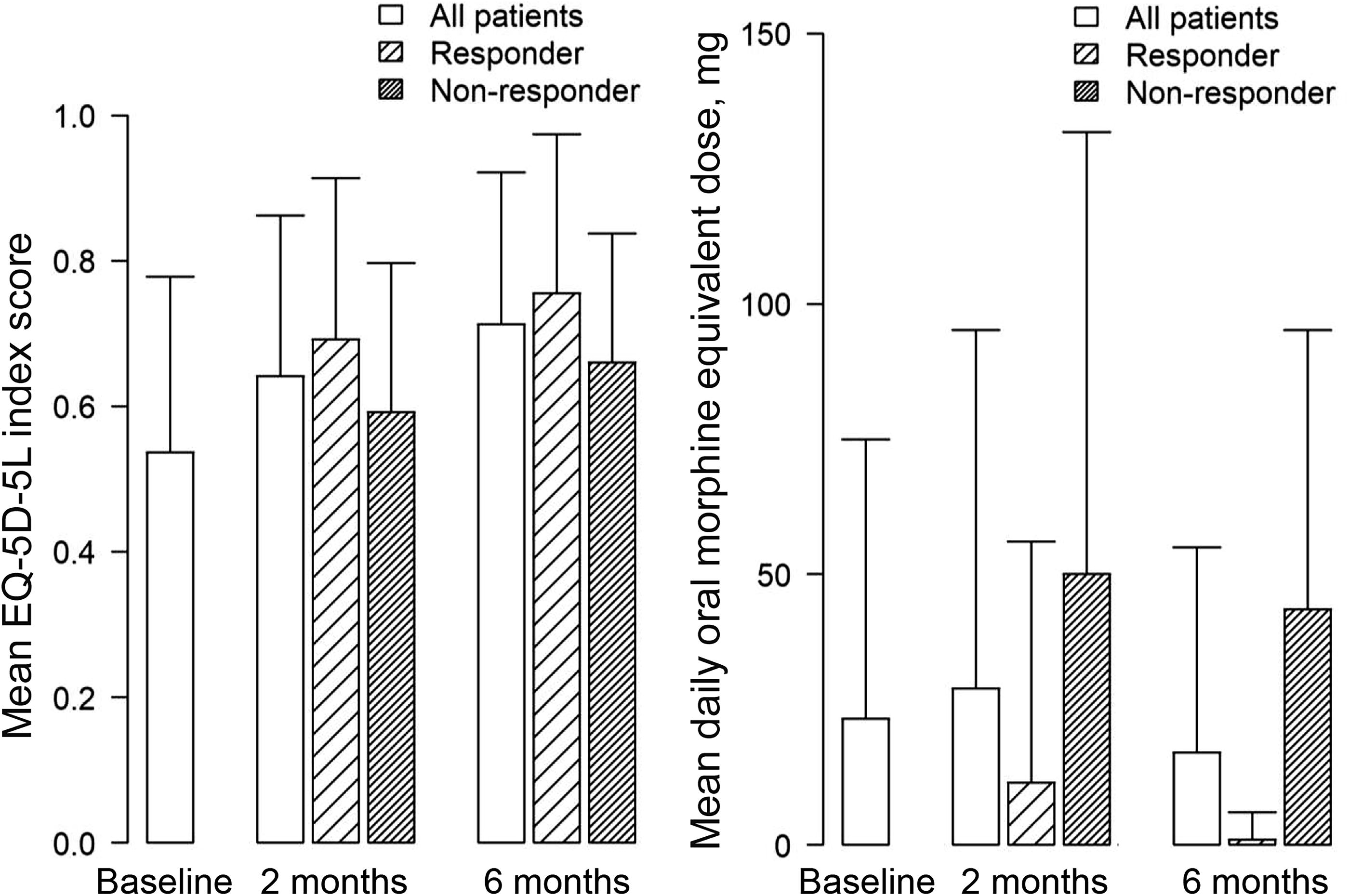
Mean EQ-5D-5L index score (utility) and daily oral morphine equivalent dose. Error bars indicate standard deviations.
Distribution of EuroQol 5-Dimensions 5-Levels Responses
Pain Response Status, Health Utility, and Opioid Analgesic Use
EQ-5D-5L, EuroQol 5-dimensions 5-levels; SD, standard deviation; IQR, interquartile range; VAS, visual analogue scale.
Health Utility and Drug Use at Follow-Up Assessments According to Pain Response Status
Comparisons between responders and nonresponders were performed with the Wilcoxon rank sum test or the Fisher exact test.
P values were less than the Bonferroni-adjusted significance level of 0.0125 (0.05/4 variables tested at each follow-up assessment).
EQ-5D-5L, EuroQol 5-dimensions 5-levels; SD, standard deviation; IQR, interquartile range.
Discussion
We determined utility values according to response status in patients receiving radiation therapy for painful bone metastases. The EQ-5D-5L index score (utility) was higher in pain responders than in nonresponders. This may suggest that palliative radiation therapy for painful bone metastases, through its pain-palliating effect, improves utility. The EQ-5D-5L index score is a single summary score attached to an EQ-5D profile according to a set of weights that reflect how good or bad a health state is according to the preferences of the general population of a country. 19 It is used in the calculation of QALYs, which informs economic evaluations of healthcare interventions. 19 The EQ-5D-5L index score is conceptually different from the EQ-VAS. While the EQ-VAS represents the patient perspective, the EQ-5D-5L index score represents the societal perspective and thus plays a vital role in health economics.
We also found that opioid dose was lower in responders than in nonresponders. This may be because the pain reduction achieved by radiation therapy reduced the necessity of analgesics in responders. Costs associated with analgesic use are another important model input in cost-effectiveness studies on radiation therapy for painful bone metastases.11–13 Opioid use is a key component of the management of cancer pain. 25 At least in Japan, the cost of opioids predominates in the overall cost of pain medication for cancer pain. Our findings regarding opioid use may be useful for model input in future cost-effectiveness studies of radiation therapy for painful bone metastases as well.
A limitation of this study is that there were substantial numbers of inevaluable patients at the follow-up assessments. High attrition rates have been an almost universal problem in studies on palliative radiation therapy.26,27 Besides patients who died before follow-up assessment, a nonnegligible number of patients was inevaluable. Those inevaluable patients likely would have had worse QOL if they had been evaluable than evaluable patients, given that patients with worse performance status and those using more opioids at baseline tended to be inevaluable. The potentially biased selection of evaluable patients might have influenced the study results in ways that we cannot measure. Another limitation was the relatively small sample size.
In summary, we determined utility values for responders and nonresponders using data from a nation-wide prospective observational study. Pain response to radiation therapy was associated with better QOL. The utility values reported for responders and nonresponders can be used for model input in future cost-effectiveness studies of radiation therapy for painful bone metastases. Another finding was that opioid dose was significantly lower in responders than in nonresponders. Costs associated with radiation therapy may, at least in part, be compensated by a reduced cost of analgesics in responders. Costs of analgesics may be an important factor to consider in a fair assessment of the balance between effectiveness and cost of palliative radiation therapy for painful bone metastases.
Footnotes
Authors’ Contributions
T.S., N.S., and T.T. are the guarantors of integrity of the entire study. T.S., N.S., T.T., and N.N. were responsible for study concepts and design. T.S. and N.S. carried out the literature research. T.S. and N.S. were responsible for the experimental studies/data analysis. T.S. carried out the statistical analysis. T.S. prepared the article. All authors edited and approved the final article.
Author Disclosure Statement
N.S. was a member of the advisory board and has received honorariums from Elekta K. K. K.I. has received payment or honoraria for lectures, presentations, or educational events from Varian Medical Systems K. K.
Funding Information
This work was supported by the Health Labor Sciences Research Grant from the Ministry of Health, Labor, and Welfare of Japan (21EA1010) and JSPS KAKENHI (24K10764).