
Abstract
Yellow nail syndrome (YNS) presents a therapeutic challenge due to its elusive etiology and lack of effective treatments. We present a case of a 77-year-old female with YNS-associated lymphedema who experienced significant symptomatic relief with subcutaneous drainage therapy, a novel intervention not previously described in YNS. Despite prior failed conventional therapies, she achieved remarkable weight loss, improved mobility, and stable biochemical parameters. Subcutaneous drainage therapy, though traditionally utilized in cancer-associated lymphedema, demonstrates promise as an alternative palliative treatment for refractory cases of lymphedema to improve quality of life.
Introduction
Yellow nail syndrome (YNS) is a rare clinical entity characterized by the development of yellow dystrophic nails, respiratory tract disease, and/or lymphedema. Diagnosis requires meeting two of the three criteria while excluding other potential causes. First reported by Heller in 1927, 1 YNS has an estimated prevalence of less than 1/1,000,000, presenting more commonly after 50 years of age, and affecting each sex equally.2,3
The etiology of YNS remains unclear. The most commonly accepted explanation is a dysfunction of the lymphatic system and impaired lymphatic drainage, leading to clinical symptoms.2,3 YNS has been associated with certain malignancies, autoimmune diseases, and immunodeficiency disorders.4–6 Furthermore, a link between titanium dioxide exposure, a common food additive, and YNS has been suggested in previous case studies.7,8
There is no cure for YNS. Treatment, therefore, is focused on symptom management. With respect to YNS-associated lymphedema, which affects 30–80% of YNS patients, 9 typical management includes wearing compression garments, applying bandages, manual lymphatic drainage, diet modifications such as a low-fat diet, and exercises to mobilize lymph.9,10 Pharmacologic therapies such as diuretics, 10 and somatostatin analogues, 11 such as octreotide, are often tried but with intermittent and unreliable success. 9 Surgical options are available but often have limited applicability and efficacy. 12 Prognosis is variable and often depends on the degree of symptoms and timing of diagnosis. Often, a patient’s symptoms recur despite ongoing treatment. 9
Herein, we describe a case of YNS-associated lymphedema treated with a novel technique—subcutaneous drainage therapy—as an alternative therapy to traditional methods. To the best of our knowledge, this technique has not been reported in patients with YNS and can be a therapeutic option for patients with refractory lymphedema.
Case Description
A 77-year-old female with diagnosed YNS was assessed in a respirology clinic for shortness of breath. She was diagnosed 10 years prior when she presented to her dermatologist with longitudinally curved, dystrophic, yellow fingernails, and bilateral lymphedema of the legs. Shortly after, she began to experience ongoing dyspnea secondary to asymmetrical bilateral pleural effusions (Fig. 1). She would go on to require multiple thoracenteses and a right-sided pleurodesis for recurrence.
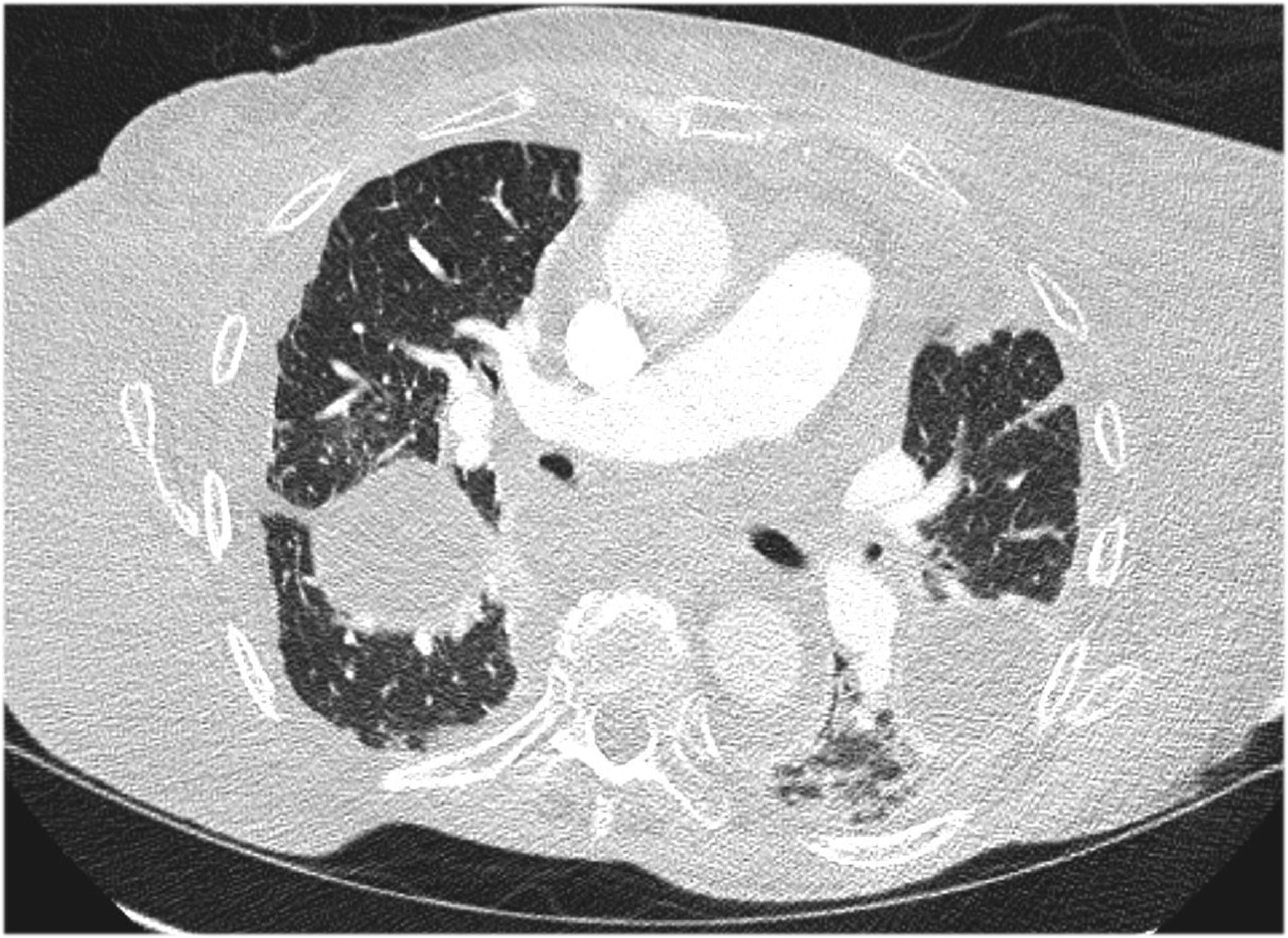
A computed tomography slice of our patient demonstrating loculated pleural fluid in the upper lung zones bilaterally alongside an increase in septal markings.
Her other past medical history included recurrent chest infections with prior radiographical findings of bronchiectasis on CT of the chest assumed to be related to her clinical syndrome, hypertension, hemorrhoids, diverticulosis, prior cholecystectomy, prior tubal ligation, and prior bunionectomy. Her home medications were furosemide, salbutamol, ipratropium, and nebulized N-acetylcysteine. She did not have any known significant occupational exposure history and had previously worked as an executive assistant and as a teacher. She endorsed an approximate five pack-year history of smoking but quit 40 years before her visit.
Her lymphedema had previously been treated by a multidisciplinary lymphedema clinic with compression banding, compression stockings, and lower extremity strengthening exercises. However, she was now requiring use of a walker to ambulate because of the extent of her lymphedema alongside the limitations of her other medical comorbidities.
On assessment, she was found to have gross nonpitting peripheral edema and a positive Stemmer sign (where the examiner cannot pinch the skin of the dorsum of the foot or hand). She demonstrated no evidence of cardiac or liver dysfunction on exam and testing.
She was initiated on octreotide for her lymphedema and a long-acting-beta-agonist/long-acting-muscarinic combination inhaler given her history of bronchiectasis. She would go on to require antibiotic treatment for multiple infectious bronchiectasis exacerbations and was subsequently started on home oxygen.
Her lymphedema was temporarily controlled with octreotide but was difficult to tolerate due to nausea and had to be discontinued. Over time, her lymphedema progressed in severity to the extent that she was no longer able to ambulate. A decision was made in conjunction with her respirologist to admit herself to the nearest community hospital to facilitate a surgical consultation given that she was failing medical therapies. In hospital, she was seen by multiple subspecialty surgical services who deemed that she was not a candidate for lymphatic-venous bypass or vascularized lymph node transplantation. She was discharged a few days later and referred back to the initial multidisciplinary clinic and was restarted on compression therapy.
She went on to develop abdominal distension and ascites thought to be due to lymphedema in the lower extremities that extended into the abdomen and tracked into the pleural space through a diaphragmatic defect. Abdominal fluid sampled was concordant with chylous ascites with a lymphocytic predominant (92%), high protein concentrated (42 g/L), and milky fluid with high triglyceride levels (13.2 mmol/L). Cytology demonstrated scattered reactive mesothelial cells and fluid culture was negative with a negative gram stain. The patient’s compression therapy was discontinued at this time with concern that it could be further exacerbating her ascites.
Her ascites was not controlled with repeat paracenteses and a medium-chain triglyceride restricted diet. She would go on to require a tunneled indwelling abdominal catheter which only partially improved her symptoms.
The lymphedema became progressively onerous to the patient. A palliative care consultation was pursued to assess whether there was a role for subcutaneous drainage of the lymphedema, a procedure used by palliative care clinicians to enhance quality of life in patients with life-limiting illness. The patient described copious weeping from a spontaneous punctate break in the skin of her right leg; guided by the weight of the baby diapers that she used to collect the fluid, it was estimated that she drained 5–7 L of fluid with significant improvement in her mobility. This supported consideration of subcutaneous drainage therapy.
The technique that was used consisted of placing two 19-gauge metal butterfly needles subcutaneously into each leg using sterile technique. The choice of placement was guided by the softness and severity of the edema, avoiding any areas with thickened skin. To facilitate the patient’s mobility one needle was placed in the anterior thigh area and one in the lateral calf bilaterally. Small urine drainage bags (with a one-way stopcock) that can be strapped to the leg, were attached to each needle using a special connector tube. The needles and insertion sites were secured using a transparent film dressing.
Two subcutaneous needles were inserted in each leg to allow the patient to strap the bags to her legs and maintain mobility; when she was sitting or lying down, she rested the bags on the bed or floor. Following the initial insertion most of the drainage seemed to flow around the needle sites rather than directly into the urine bags. Therefore, subsequent insertion was modified to use the needles to form drainage tracts with drainage of lymph fluid targeted into dressings or into larger drainage bags attached via adhesive and bands. Needles remained in situ for a period of 48–72 hours or as tolerated by the patient before being removed. After the initial treatment and two modified needle insertions, she had lost 75 lbs from a 170-lb baseline over a one-month period (Fig. 2). As a result, her mobility was much improved, enhancing her quality of life. She was psychologically buoyed by this success after losing hope of any improvement. Her serum electrolytes and albumin levels remained stable (Table 1). She eventually died a few months after initiating therapy from complications of a fall likely related to years of deconditioning due to immobility.

Photos of before and after subcutaneous needle drainage therapy. After photos were taken approximately three months after initiation of drainage therapy.
Biochemical Profile Including Electrolytes, Kidney Function, and Albumin Before and After Subcutaneous Drainage Therapy
Discussion
Subcutaneous drainage therapy can serve as an alternative and effective means for symptomatic management of lymphedema in patients refractory to conservative and pharmacologic therapies. To our knowledge, this is the first case study describing subcutaneous drainage therapy in a patient with YNS.
Subcutaneous drainage therapy has been employed for palliative intent in patients with cancer-associated lymphedema refractory to pharmacologic and compression therapies. First described in 2004 by Clein et al., 13 there have been many case reports describing its utility in improving symptoms and quality of life in cancer patients.14–22 One study performed in multiple centers with 31 patients utilized a standardized questionnaire to evaluate quality of life improvement with subcutaneous drainage therapy in cancer patients undergoing palliative treatment. 16 The results suggested that subcutaneous drainage therapy improved quality of life and appearance in patients impacted with severe, debilitating, life-limiting illness. Although utilized in a different population, these results are concordant with our patient’s experience with subcutaneous drainage therapy.
There has not been a standardized approach to delivering subcutaneous drainage therapy. Some studies have advocated for the use of analgesia before needle insertion, 18 which was not utilized in our study, as the insertion pain is brief. Others have utilized a closed versus an open drainage system, with some arguing that an open system will encourage mobility during treatment. 18 Furthermore, the frequency and the duration of treatment has varied across previous studies. Currently, no standardized protocol exists that suggest the optimal implementation of subcutaneous drainage, and thus we recommend the approach described above as it was effective and found to be safe. Previous studies have also shown improvement in both the hospital setting and the home setting, suggesting versatility in use. 17 If used in the home setting, there is the need for patients to have some level of independence or allied health support, which may vary depending on regional access to resources, comorbidity burden, and functioning status of the patient.
Given that this modality penetrates the skin, there is some concern for infection risk. In a larger study with 31 patients, 2 patients developed cellulitis, which demonstrates a complication rate of 6%. 16 Other documented case reports have not reported localized or systemic infection associated with subcutaneous drainage therapy.14,15,17–22 One consideration is to use waterproof transparent film dressings below the area of leakage to prevent persistent wet skin and associated irritation. Patient discomfort and impact on mobility during subcutaneous drainage therapy is another potential concern. Given that the needles can be kept in situ for an extended period, mobilization can be cumbersome. Similarly to our case, some studies have argued for an open system with leakage into dressings directly with frequent dressing changes; 18 however, this patient found standard dressings were soaked through rapidly, requiring multiple dressing changes per day. As mentioned, she found that baby diapers over sterile gauze were more effective.
Previous studies with cancer patients have demonstrated that biochemical profiles often remain intact with the exception being albumin, 16 although greater fluctuations of albumin could be expected in this patient cohort due to a chronic state of inflammation, malnutrition, cachexia, and liver dysfunction in the setting of liver metastases. Electrolytes and a biochemical profile were monitored during subcutaneous drainage therapy in our patient with no destabilization in these values, including albumin.
Conclusion
Subcutaneous drainage therapy can serve as an effective alternative modality for treating lymphedema that is refractory to other therapeutic measures. This approach offers the potential for significant improvement in both symptoms and quality of life and should be considered within the broader spectrum of therapies for lymphedema.
Footnotes
Author Disclosure Statement
The authors have no financial or personal interests to disclose.
Funding Information
No funding was received for this article.