
Abstract
Background:
Communicating with a parent or guardian after their child’s death is considered one of the most difficult tasks in medicine. While several frameworks have been developed to aid clinicians when delivering bad news, they are incomplete without the perspectives of bereaved family members. The GRIEV_ING Educational Intervention is one well-established framework for death notification that currently lacks feedback from bereaved family members.
Objective:
Bereaved parents have valuable insights for trainees learning to communicate with grieving families. Our aim was to elicit and analyze bereaved parent feedback on the GRIEV_ING framework.
Design:
Pediatric Critical Care Medicine and Pediatric Emergency Medicine fellows completed simulated conversations with standardized actors using the GRIE_VING framework. Conversations were audiovisually recorded for analysis by bereaved parent volunteers. Parent volunteers reviewed recordings of selected sessions and provided feedback on participants’ performances and the GRIEV_ING framework via semistructured interviews. These interviews were then qualitatively analyzed for common themes.
Setting:
A pediatric tertiary hospital in the United States.
Results:
Five bereaved parents provided feedback on the GRIEV_ING framework. From this feedback, we identified five themes that were important to bereave parents and were absent from the GRIE_VING framework: (1) Reassurance, (2) Avoiding False Hope, (3) Preparing for the Child’s Appearance, (4) Sacred Space, and (5) Offering Guidance.
Conclusions:
The five themes that emerged from interviews with bereaved parents demonstrate the importance of including family members when developing communication curricula. Eliciting feedback from bereaved parents added more nuance to the already well-established GRIEV_ING framework.
Key Message
Bereaved parent volunteers have valuable insights for trainees learning to communicate with grieving families. Yet their perspectives are often missing from educational interventions. We elicited and analyzed feedback from bereaved parent volunteers on the well-established GRIEV_ING framework for death notification.
Introduction
Communicating with a parent or guardian after their child’s death is considered one of the most difficult tasks in medicine. 1 Clinicians must clearly and empathetically explain the events surrounding the child’s death, respond to complex emotions, and give the family time with their child.2,3 The ability to do this with compassion can have a lasting impact on the grieving process.4,5 Indeed, surveys from bereaved parents acknowledge that the manner in which the news of their child’s death is delivered has long-lasting effects on their well-being.2,6
Given the relative rarity of pediatric deaths, providers can feel unqualified to lead these conversations. Prior education is therefore necessary to prepare clinicians. However, trainees predominantly learn through observation and role modeling from their supervising providers. The focus is often on the provider’s viewpoint, and the perspectives of patients and families can be lost. 7
Over the past decade, there has been a growing recognition of the need to include bereaved parents in pediatric training. From sharing their stories with providers, aiding in the development of bereavement programs, and acting as faculty facilitators in educational programs, parents have contributed to the education of both trainees and established clinicians.8–10
Bereaved parents are a vulnerable population, and their psychological safety should take precedence when involving them in educational endeavors. That said, bereaved parents have reported benefits, including helping other families, giving back to the institution where their child was cared for, and adding to their child’s legacy.8,11
We therefore aimed to elicit feedback from bereaved parent volunteers on a well-established educational intervention that lacked parental input.
Methods
The GRIE_VING educational intervention
We sought parental input on the GRIE_VING Educational Intervention, which was developed by Hobgood et al. in 2004. The intervention was designed to teach emergency medicine residents the skills needed to effectively and compassionately communicate with family members following a patient’s death, particularly in instances where the death is sudden or unexpected. 12 It has since been adapted to train anesthesiology residents, pediatric residents, and paramedics.13–15 During the intervention, trainees participate in a series of simulated conversations during which they are tasked with notifying a family member of their loved one’s death. The educational component is centered on the GRIEV_ING framework (G: Gather, R: Resources, I: Identify, E: Educate; V: Verify, _: Space; I: Inquire; N: Nuts and Bolts, and G: Give) (Table 1). 12
The GRIE_VING Framework Developed by Dr. Hobgood et al.
The GRIE_VING Educational Intervention has been shown to improve provider competence in delivering a death notification, both in its original form and subsequent adaptations. However, competency was defined as adherence to the GRIE_VING framework and was graded with the use of a checklist. 12 While the framework was based on a comprehensive literature review, it was developed by a clinician, for clinicians, and was validated by clinician-researchers. To our knowledge, the GRIEV_ING framework has not been evaluated by bereaved family members, who provide an important perspective as the population the framework is utilized with.
Pediatric Emergency Medicine and Pediatric Critical Care fellows at our institution participated in the GRIE_VING Education Intervention, and their simulated conversations were audiovisually recorded for review by bereaved parent volunteers.
Sampling strategy
Following approval from the University Hospitals Rainbow Babies and Children’s institutional review board, bereaved parents associated with the hospital system were first contacted by representatives from the Division of Pediatric Palliative Care. Only parents who had participated in one of the hospital system’s bereavement group activities in the last year were contacted. Parents whose child had died within the previous three years were not approached, both for the parents’ psychological safety and to avoid their recognition of a research participant.
Information regarding the research and its potential role was provided. If parents were interested in participating, the research team contacted them via email with further details and obtained written consent. Parents were given the option to participate in person or virtually, based on their comfort level. Parents were also offered the opportunity to interview together with their partner or individually.
Data collection
Semistructured interviews were conducted either in person or virtually with a member of the research team (L.B.). The interviews were 30–45 minutes in length and included (1) viewing of two audiovisually recorded scenarios with subsequent feedback, (2) discussion of the GRIE_VING framework, and (3) open-ended questions on their experiences communicating with clinicians following their child’s death.
Data analysis
Rigor and credibility were sought in a number of ways. A structured analytic approach was determined prior to beginning the data analysis, peer-debriefings were held during each phase of the analysis, and researchers reread the interview transcripts at regular intervals to ensure that emergent themes were linked directly to the primary data.
First, parent interviews were audio-recorded and transcribed. Two members of the research team (L.B. and B.R.) conducted the thematic analysis using a modified grounded theory approach, as outlined in Figure 1. 16 Transcripts were first read individually in order to become familiar with the material and to open code—a process in which reviewers identify key words or phrases present in the transcripts. The research members then met for peer-debriefing and to develop a code book. Transcripts were reread individually to apply the codes to each statement. A partnered discussion was then held to identify emergent themes. The transcripts were reread twice with reference to these themes. Finally, theme descriptions were adjusted as needed to accurately reflect the values identified in the source material.
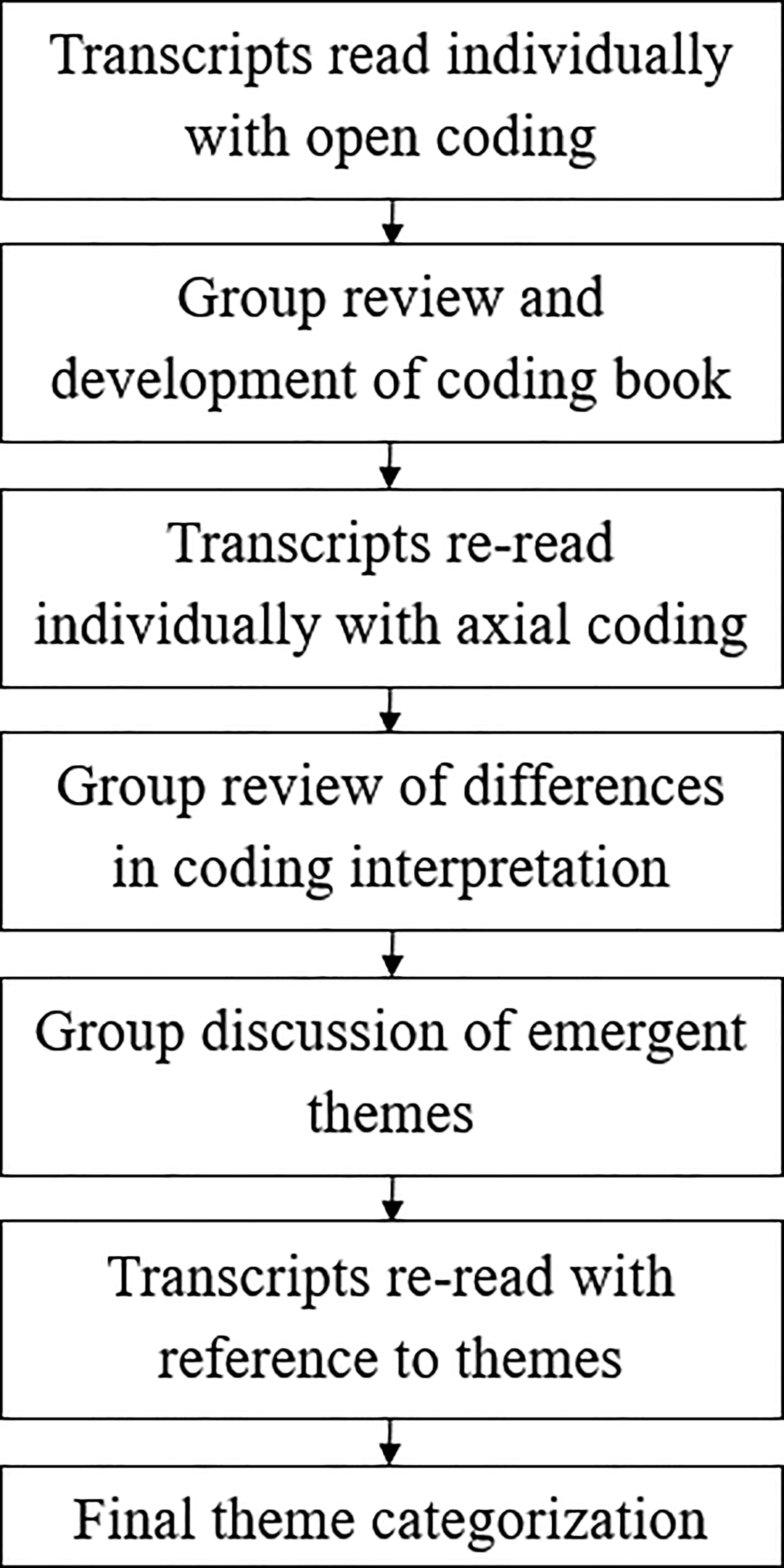
Modified grounded theory approach to qualitative analysis of parent interviews.
Results
Seven parents were approached regarding research participation. Of these, five parents representing three children participated in semistructured interviews. This included two fathers and three mothers. One parent chose to interview in person, while the remainder interviewed virtually. Two parents interviewed together, and three interviewed individually. All participants were Caucasian.
We identified five themes that were important to bereave parents and were absent from the GRIE_VING framework: (1) Reassurance, (2) Avoiding False Hope, (3) Preparing for the Child’s Appearance, (4) Sacred Space, and (5) Offering Guidance. Parent quotations are italicized and tagged with the associated parent’s label.
Reassurance
Reassuring parents that they did the right thing by seeking care was discussed several times. Parent volunteers expressed that telling grieving parents, “You did everything good. You didn’t do anything wrong” [P2] was valuable. While volunteers acknowledged that reassurance would likely not take away the guilt that parents might feel, they still thought it was important to hear assurances from the provider.
I go back to that reassurance, because when you’re reassuring, then you’re putting yourself … in that idea that we’re on the same team. Particularly in an ED situation where you don’t have that established relationship. [P1]
Avoiding false hope
In every interview, parents emphasized the importance of verifying the child’s death early in the conversation. By delaying the delivery and instead focusing on events leading up to the child’s death, parents felt that providers could give false hope.
You don’t want to wait too long, [because the parents are] thinking a thousand things in their head. They have that hanging thread of hope. [P3]
I think it’s important to early on establish that the child has died. The waiting is so hard, because all you’re doing is making up stories in your head. [P1]
When reviewing the simulated conversations, one parent commented,
I would’ve liked to hear the news that my child had died right away, instead of asking the parent for information about what happened. That kind of gives the impression that there’s gonna be an update … that’s more positive. [P4]
Preparing for the child’s appearance
The GRIE_VING framework includes multiple steps to prepare for delivery of the news, including gathering all family members and calling “support resources available to assist the family with their grief. 12 ” However, the interviewed parents expressed the importance of preparing family members for what their child will look like. This includes pallor, bruising from chest compressions, breathing tubes, and venous lines. While this was not included in the GRIE_VING framework, all fellow participants included these descriptions in their simulated conversations.
I think that’s really, really important. Particularly in a situation where she’s an otherwise healthy child … parents don’t have experience with seeing what their child looks like unwell. Much less after they’ve died. So I feel like that was really, really important. [P1]
You don’t know what it’s gonna be like. Especially if there’s some kind of accident or interventions that might look disturbing. Like, with our son, he had CPR for a while, so he had bruising. [The team] kind of prepared us for that a little bit. That was nice … to describe what the situation’s going to look like. [P5]
Sacred space
Multiple parents expressed the desire to see their child early, rather than having a prolonged conversation away from the bedside. They valued private time with their child, without interruptions from unknown personnel. While this is not directly related to communication, it does impact the structure of the conversation. Three parents suggested that the GRIEV_ING framework should be divided into two separate conversations, allowing for private time with their child before moving on to logistics.
Letting them see their child I think is important. That was big for us … we had a long time just with our son, before we got on with the business of what we had to do after. [P4]
You’re gonna have to assure them that they’re gonna have the opportunity to see their child and be with them … for as long as they want. And if you don’t have a relationship with [the hospital staff], then maybe have a point person who deals with the family the most … you don’t want a ton of people in that private space if you don’t know them. [P5]
I felt like any strangers coming in were not really people I wanted to be around. [P4]
Offering guidance
The GRIE_VING framework includes an extensive list of topics to cover, including the “Nuts and Bolts” of notifying the mortician, organ donation, and delivering personal belongings. The interviewed parents discussed the feeling of paralysis that comes with hearing the news of their child’s death and how overwhelming those logistics can be. As aforementioned, one technique suggested was to let the parents be with their child before discussing these topics. Multiple parents also felt that going one step at a time—either by giving parents the options of what to do next or by prompting them to complete the next step—helped with information overload.
[Asking] “Do you want to talk to the chaplain first? Do you want to see your kid first? Do you want to call relatives first?” Your mind is so blank at that point … anybody offering me choices was easier than me coming up with it myself. [P5]
As the parent, I think your brain is probably really scattered or blank; you’re not sure what to do. They have to probably be prompted on what needs to happen next. [P4]
Space
The GRIEV_ING framework includes the term space to describe “allowing the family time to absorb the information.” Parents praised the study participants for appearing comfortable with silence and “not filling empty space with words” [P1]. While this is not a new theme, it was a concept that was brought up by multiple parents and warrants emphasis.
Discussion
Communicating with parents and/or guardians after the death of a child is challenging no matter the circumstances. Given the relative rarity of pediatric deaths, providers may not have extensive experience leading these conversations. Insights from bereaved parents can help prepare clinicians to navigate interactions with grieving parents.
Our findings indicated that parents are looking for empathetic guidance through the steps that follow a child’s death. While every family and situation is different, clinicians understand the logistics that follow a child’s death—notifying the mortician, discussing funeral homes, offering legacy, or memory-making mementos. For parents, these logistics are overwhelming and unclear. Carefully guiding parents through these steps can help mitigate feelings of paralysis or information overload.
We found that parents can feel misled or given false hope when clinicians wait too long to reveal that their child has died. After this has been established, parents want private time with their child as soon as possible. While the clinician may feel the need to provide more information regarding the child’s death and next steps, our parent volunteers felt that these conversations could wait until after grieving parents have had a chance to spend time with their child.
These themes are not only applicable to delivering the news of a child’s death. They may be helpful when communicating with parents in other situations. Providing reassurance and guidance can be beneficial for parents of children with a chronic illness, new diagnosis, or injury. Preparing parents for what their child will look like with a breathing tube or central line is particularly relevant in the intensive care unit (ICU) setting. Perhaps most relevant is the reminder that clinicians have an understanding of the medical system that most parents lack. Sharing this information with parents may help with feelings of being overwhelmed and enable them to make more informed decisions about their child’s care.
These findings are consistent with other published studies on communicating with parents. Notably, a qualitative study on physician–parent communication during end-of-life care revealed similar themes, including the negative association with false hope. In the study, parents felt led on when physicians withheld information regarding their child’s prognosis. 3 In a similar study, parents of children with cancer emphasized that difficult conversations should not be delayed. 7 Both studies also included themes on pacing, to allow parents to come to terms with difficult news.3,7
There are several limitations to our study. Our hospital system provides medical care for a diverse population in terms of socioeconomic status, ethnicity, and religion. However, our interviewees were all White parents with moderate-to-high health literacy. Thematic saturation was achieved with this group of interviewees, but additional themes may have emerged had we interviewed parents from other cultural or economic backgrounds.
We also sought volunteers who were well-established with our bereavement program—including participating in a yearly remembrance walk. Based on their continued interactions with our bereavement team, these were parents who were more likely to have had a positive experience with our hospital system and palliative care program. Parents with more negative experiences or perceptions might have had different insights.
Further steps include incorporating the themes identified by bereaved parents into the initial trainee education. These themes of (1) Reassurance, (2) Avoiding False Hope, (3) Preparing for the Child’s Appearance, (4) Sacred Space, and (5) Providing Guidance could be used to enhance both the GRIE_VING framework and other communication curricula. A larger qualitative study with parents of diverse cultural, racial, and socioeconomic status would also help to identify the needs of parents not represented in our study.
Conclusions
While this was a small pilot study, we gained valuable information regarding the perspectives and needs of grieving parents. The GRIEV_ING framework is a well-established, previously validated educational intervention that is based on an extensive literature review. And yet, bereaved parents still felt that there were missing components. This work emphasizes the need to include family members in palliative care and communication education.
Footnotes
Acknowledgment
The authors would like to express gratitude to Lauren S. Seifert, PhD, for her valuable insights when editing this article.
Authors’ Contributions
L.B. and I.M.A. designed and directed the project. L.B., I.M.A., K.G.-L., and N.S. carried out the simulations. L.B. conducted interviews. L.B. and B.R. completed the qualitative analysis. L.B. wrote the article with input from all authors.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
The authors received financial support from the Case Western Reserve University Hospitals Fellowship Research Awards Program for this research.