
Abstract
Introduction:
Psilocybin-assisted therapy (PAT) has gained traction in palliative care as a treatment for existential distress in the last decade. Patients with brain cancer have been excluded from studies, yet they stand to benefit as much as other patients with cancer-related psychological distress.
Case description:
In this report, we discuss the case of a patient with end-of-life distress secondary to stage 4 astrocytoma that received PAT through Health Canada’s Special Access Program. The patient had a positive response to PAT without adverse events.
Discussion:
Standard treatment for existential distress is often inefficacious and PAT is rarely available, especially for patients with brain cancer. We highlight the importance of making PAT more available as many patients with unresolved existential distress resort to medical assistance in dying without ever knowing of the existence of PAT.
Conclusion:
PAT was effective in partially alleviating the patient’s existential distress. Access to PAT needs to be expanded urgently.
Introduction
Psilocybin-assisted therapy (PAT) has gained popularity in the past decade as a promising treatment modality for end-of-life distress in cancer patients.1–4 This is particularly significant considering the lack of definitive treatment for such a serious illness. Conventional approaches to anxiodepressive symptoms such as pharmacotherapy and psychotherapy, although partially effective, have a low-to-moderate effect-size, and are not well studied in patients with cancer. 5
While PAT results have been impressive in the most recent small scale 2016 RCT’s, patients with cancer involving the central nervous system (CNS) have been excluded from studies due to the potential risk of seizures. Furthermore, all recent studies exploring PAT have excluded patients with known epilepsy or recent seizures. Although the risk of seizures is low with psilocybin even in recreational settings,6,7 little is known about the real risk of seizures due to psilocybin exposure in patients with brain cancer.
Patients suffering from brain cancer are a particularly relevant population for PAT. They are afflicted by one of the most prevalent neoplasia in adolescent and young adults, which is associated with substantial morbidity and mortality. 8 Not only are these patients diagnosed at a younger age than the average cancer population, they are also prognosed with a devastatingly limited life expectancy. The resulting demoralization and despair they face could stand to benefit strongly from this therapeutic tool. Additionally, it may also facilitate the profound process of grief that is shared by the loved ones, family and friends of this specific patient population, who are also negatively affected.9,10 This secondary burden of disease could be alleviated through a healthier acceptance of the dying process, which PAT has been shown to offer.1–3
Since January 2022, psilocybin has been available through the Health Canada Special Access Program under specific and limited conditions, one of which is end-of-life distress. It is in this context that we chose to treat a patient with primary brain cancer suffering from existential distress with psilocybin.
Case Description
In September 2022, MR (the patient) had her first seizure episode when she was diagnosed with stage 4 astrocytoma at 41 years-old. She was given a prognosis of 9–12 months life expectancy. In April 2023, she was referred to our team by another patient who had received PAT under our care.
She was generally healthy, with a long-standing generalized anxiety disorder (GAD), which had worsened since the cancer diagnosis, and two past depressive episodes in 2000 and 2015. At the time of our initial involvement, she had received two neurosurgeries, radiotherapy and was completing chemotherapy. She received cognitive behavioral therapy for her anxiety and existential distress with only partial improvement. She was not interested in using selective serotonin reuptake inhibitors as she had not tolerated them well with multiple past attempts for GAD and had seen no benefit from them. Furthermore, she felt that chronic daily medication was not aligned with her therapeutic goals as it would not address the root causes of her distress.
The shared decision-making process included an in-depth discussion around the small risk of seizure and secondary complications that might ensue. These conversations were limited in our ability to discuss these risks with an evidence-informed approach due to the aforementioned lack of research. The conclusion of this process with additional input from her treating neuro-oncologist, was to safeguard this potential risk by doubling her dose of Keppra on the day of the session, and to have on-hand sublingual lorazepam and intramuscular midazolam in case of a prolonged seizure.
Management and Outcome
Once we received approval from Health Canada, we started preparation sessions for PAT. On August 2023, she underwent her first PAT session which went well, without any adverse events nor seizures. She had a strong mystical and emotional experience as objectified in the emotional-breakthrough inventory (550/600) and mystical-experience questionnaire (107/150).
In the patient’s own words: “I remember arriving under a huge golden arch where sparkling crystals were falling towards me. Beings of light like immense angels were there waiting for me. I remember thinking how beautiful the confines of my mind were and I felt tears streaming down my cheeks. Then I said out loud: ‘Please leave me here, I’m already there!’ I felt myself floating towards these immense angels. Afterwards, I went towards the darkness of my soul and it was a long journey.”
She had a significant and rapid improvement of all her symptoms (Fig. 1) within the following weeks. She was followed for integration and individual psychotherapy during the following months. As some of her anxio-depressive and demoralization symptoms started to recur, a second PAT session was considered. The patient also felt she would benefit from a second session, now knowing better what to expect and how to prepare.
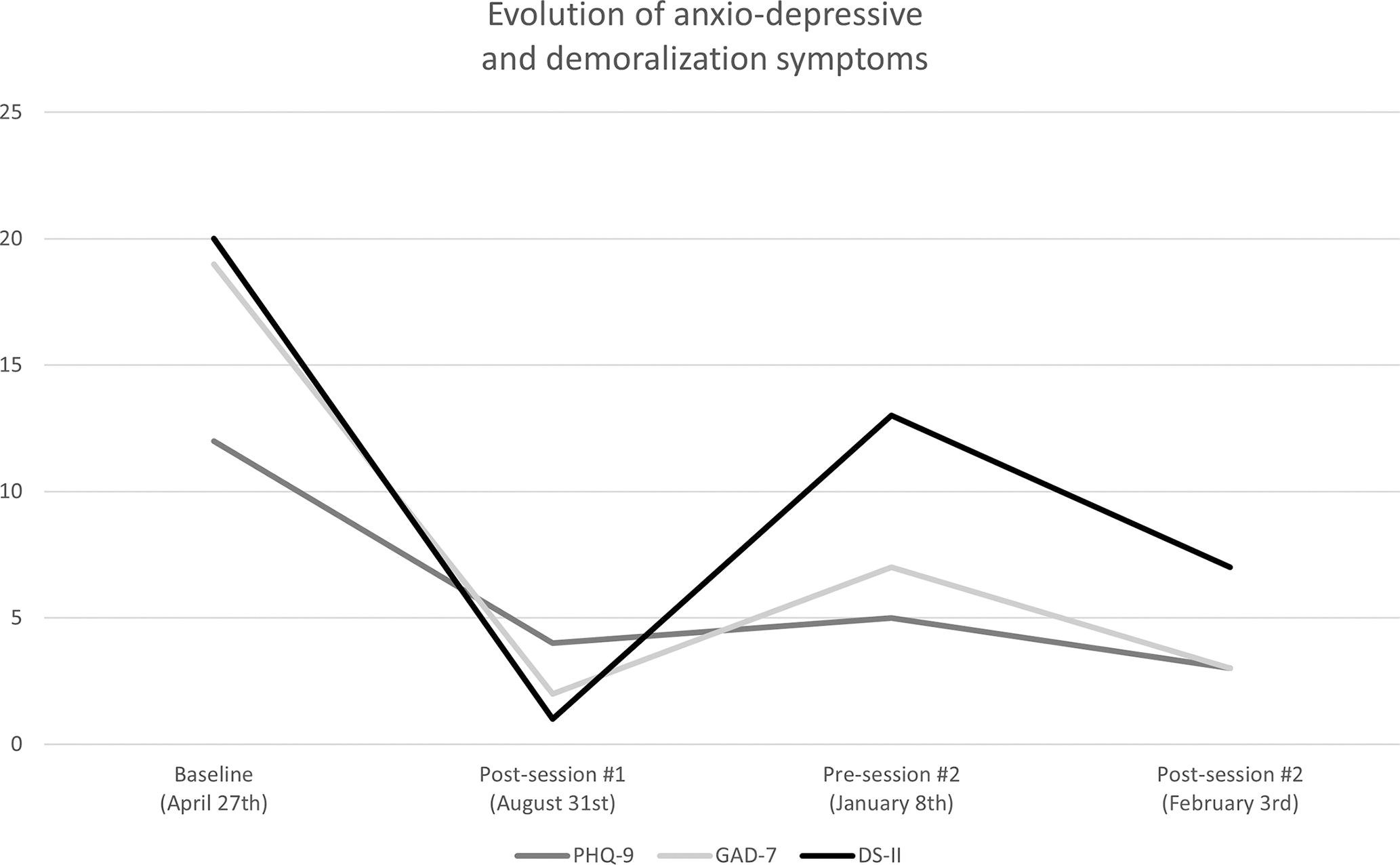
Evolution of Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder 7 (GAD-7), and Demoralization Scale-II (DS-II) scores from baseline on April 27th 2023 to February 3rd 2024. The first PAT session was on the 18th of August and the second PAT session was on the 11th of January.
On January 2024, she received her second PAT session that also went well without any complications. However, its content was emotionally more challenging and painful, including deep experiences of sadness, grief, and fear. MR reported peace and gratitude the following day during the first integration session. She linked the session’s emotional releases to her initial intentions of finding back her inner compass, and noted that these emotions had to be expressed and felt through to reconnect to her inner guidance. Acceptance of difficult emotions, which had been a challenging part of the preparation work, now made experientially more sense to her.
She also had a positive response to her second session in alleviating her symptoms, although less dramatic than the first (Fig. 1). We chose to continue individual psychotherapy after the integration sessions to deepen the therapeutic process of acceptance of her situation, which had been catalyzed by PAT.
Discussion
We decided to offer PAT to a patient with existential distress in the context of brain cancer, complicated by seizures, by carefully weighing the risks and benefits in a shared-decision making process. Acknowledging that brain cancer was an exclusion criterion for PAT studies and the limited data on the risk of seizures associated with psilocybin, more research is needed to best support patients facing such serious illnesses that can be difficult to treat with conventional modalities.
In our opinion, the most compassionate choice for this particular patient was to offer her PAT while considering the unforeseeable nature of potential risk, and to assist her in making an “as-informed-as-possible” choice. In this particular case, the patient responded well without any complications. However, more documented cases are required to safely and effectively disseminate this treatment to a larger number of patients.
At the present moment in Canada, it is far easier for patients like the one discussed here to have access to medical assistance in dying (MAID) than it is to have access to PAT, even if the sole reason for accessing MAID is their psychological distress. It is our view that facilitating access to PAT for patients with existential distress in the context of incurable illness should be immediately prioritized, as suggested in the Report of the Special Joint Committee on Medical Assistance in Dying of February 2023, 11 to make it at least as accessible and available as MAID.
Conclusion
We’ve discussed the case of a young women in her forties treated with psilocybin for her existential distress in the context of brain cancer who did not sufficiently benefit from psychotherapy and for whom pharmacotherapy did not align with her therapeutic goals. PAT had a significant beneficial impact without serious adverse events.
This case highlights the importance of including a wider variety of terminal illnesses in the research on PAT for end-of-life distress, as well as the urgent need to make PAT more available for patients who are candidates to MAID. The current legislation creates a situation where some Canadians will choose MAID for their end-of-life distress without ever being told of the existence of PAT, a therapeutic modality that has been shown to be safe and effective at treating existential distress and the accompanying anxio-depressive symptoms.
PAT is neither a replacement nor an alternative to MAID. It is simply a treatment modality that needs to be integrated as an accessible option in palliative treatment care plans, and obviously offered before MAID. It is appropriate time that the Canadian Parliaments’ Committee on MAID Recommendation 9, stating that Health Canada should review laws and regulations to improve access to psilocybin, be implemented.
Footnotes
Acknowledgment
The authors would like to thank our patient for her courage and willingness to go through the transformative and demanding process that PAT can be and for her generosity to share her direct experience.
Author Disclosure Statement
The authors have no conflict of interests to declare.
Funding Information
No funding was received for this case-report.