
Abstract
Background:
Understanding the environment in which patients live at the end of their lives is essential to improving palliative care for these patients and their families.
Objectives:
We aimed to explore the different living places and trajectories of palliative care patients in the last three months of life in primary care and to identify patient characteristics associated with these trajectories.
Methods:
This retrospective national study was carried out among a population of adult patients who died a non-sudden death. The trajectories were modeled and classified using sequence analysis, optimal matching, and hierarchical ascendant clustering. Univariate and multivariate multinomial logistic regression compared patient characteristics associated with these trajectories. The focus was on primary care. Patients had to have spent at least one day at home or in a nursing home in the last three months before their death. The research took place between November 2020 and November 2021 in mainland France.
Results:
Three hundred adult patients were included in the study. Cluster analysis revealed three main trajectories during the last three months of life: “staying at home” (57%), “staying in a nursing home” (29%), and “moving from home to hospital” (14%). Dementia and having children limited hospitalization. Not having an informal caregiver and having dementia were associated with staying in a nursing home.
Conclusions:
Palliative care patients’ living situations and transitions can be tracked using primary care practice data. This study highlights the unique needs of palliative care in home and nursing home settings. Additionally, factors such as dementia and family dynamics play a significant role in determining where patients live, which can help inform clinical practices and research strategies in palliative care.
Key Message
Cluster analysis highlights three trajectories for palliative care patients in primary care: “staying at home,” “staying in a nursing home,” and “moving from home to hospital.” Less than 20% had a hospital-based trajectory. When considering hospitalization, informal caregivers and children need to be consulted.
Introduction
In an advance care planning approach, data from end-of-life research can contribute to information and health care recommendations for the patient and the family. 1 Two situations must be considered: the living place and the place of death. 2 The place of death is more commonly studied in the literature—with home being the preferred place, particularly for cancer patients. In 2015, a systematic review found that studies reporting preferences for place of death often did not include patients who had no preference. 3 End-of-life decisions vary according to the care setting and the progression of the disease.4,5
From an epidemiological perspective, end-of-life data can support palliative care policies and suggest predictors. 6 Most papers focused on the place of death. Using death certificates, some authors tracked place of death trends over the years.6,7 In Europe, they showed differences in the place of death between different countries and suggested that health policy was the main factor.6,8 Few studies have used administrative health data to evaluate palliative care policies and describe hospital admissions in the last months of life.9,10 Using the National Health Insurance Information System from 2013, a French study described both where the patients were living during the year preceding death, and the place where they died. It highlighted the dynamics of hospitalization with admissions increasing in the months before death. The home death rate, estimated indirectly, was 29%. People who received palliative care in hospital were more likely to die in hospital than those who did not. 9
End-of-life data collection is often limited to hospital indicators, with a lack of research in primary care.11,12 Since 2005, European teams have used data from different national general practitioner (GP) sentinel networks. They focused on the last three months of life of patients who died non-suddenly and looked at transitions between care settings.11,13–15 In the EURO-SENTIMELC study, the main final transition was from home to hospital. Home death rates ranged from 23% to 49%, depending on the country. Consistent with previous death certificate studies, this study supported the feasibility of using primary care databases, especially through GPs. 11
Measuring the prevalence of palliative care needs remains challenging, particularly at the community level. 16 A better understanding of where patients with serious illnesses live and receive care could help to tailor palliative care resources. Our study aimed to explore the end-of-life location of palliative care patients and associated factors.
Methods
This study was conducted in mainland France. The first objective was to visualize and quantify the end-of-life locations and trajectories of palliative care patients who were followed by a GP, using plot modeling of trajectories. The secondary objective was to statistically test potential factors influencing these trajectories.
The research was based on data collected by GPs on patients after their death. The main inclusion criteria were predictable and non-sudden death. Patients were aged 18 years or over and had spent at least one day at home or in a nursing home in the last three months of life.
A monitoring committee reviewed the inclusion criteria based on the cause of death reported by the GP. During the inclusion period, from November 2020 to November 2021, GPs completed questionnaires regarding deceased patients they considered to have met the study criteria. They could complete either a paper case report form or an electronic one using the web application RedCap (www.project-redcap.org). Participating GPs were members of the French Sentinel network (https://sentiweb.fr/).
The questionnaires included several types of data. The patients’ socio-demographic characteristics were age, sex, marital status, number of children, cohabitation, and presence of an informal caregiver (only non-professional caregivers were considered in the paper). The urban or rural location was determined by the GP’s office location. The medical variables were the primary illness responsible for the death and any secondary acute intercurrent illness. GPs were also asked whether the patient had comorbid dementia and, if so, whether they considered it to be mild, moderate, or severe. Due to the inclusion period, COVID-19 was specifically studied as a primary and secondary disease. Regarding data for the patient’s location in the last three months before death, GPs were required to list the patient’s successive locations and duration in each location in reverse chronological order from death (day 90) to day 1. Five locations were preselected: home (own or family home), nursing home, hospital (standard hospital units including aftercare and rehabilitation units), long-term care hospital unit (with more medical resources than in nursing homes), and palliative care unit. We coded the relevant variables as continuous variables or classes according to the literature and clinical considerations.
To describe the trajectories, we used sequence analysis and emerging epidemiological methods derived from the social sciences, initially developed in biology for DNA sequences but already used in health research to study clinical pathways.17,18 Using SAS and then the TraMineR package for R, the description of the sequence of living places was longitudinal. A collectively scaled chronogram enabled us to visualize the number of patients in each location on a daily basis and to highlight the most frequent living place for each day. Linked to the chronogram, the transversal entropy measured the dispersion of the patients in the various locations day by day. Individual scaled plots (sequence index plots) demonstrated all the individual trajectories, meaning the sequence of place and duration of each stay for each patient.
To compare sequences, we used the optimal matching method and hierarchical ascendant clustering (HAC) with Ward linkage. These methods allowed a side-by-side comparison of each sequence using specific parameters such as a 2-constant value substitution cost matrix and a default insertion/deletion cost of one. The graphical representation of the hierarchical clustering is represented as a tree diagram, the inertia jump curve and the calculation of the mean intra-class distance showed the evolution of the dispersion and the intra-class heterogeneity, according to the number of clusters. In the clusters, we also used the lowest number of patients still sufficiently relevant for statistical analysis. Overall, we looked for clinical relevance by examining the mean time spent in each location.
To compare subpopulations, we adjusted for both medical and socio-demographic conditions. We used multinomial logistic regression with the most prevalent trajectory cluster as the reference. The results of univariate analysis and the clinical relevance allowed the selection of variables for the multivariate analysis. Age and sex were retained in the final models. The variable “main disease” was changed to “cancer” versus “non-cancer,” and the variable “comorbid dementia” to “dementia” versus “no dementia.” Marital status was binarized into “in a couple” and “not in a couple.” In a step-by-step procedure based on the lowest Akaike information criterion (AIC), starting with the factors age and sex, we tested the best models. The significance threshold for all of the statistical analyses was 0.05.
There was no gold standard for calculating sample size or odds ratio (OR) in the literature on factors in community-based end-of-life care. The sample size of 300 patients was initially calculated to highlight the statistical association between a patient factor and the occurrence of a binary event, considering an OR of 3 and a 10% proportion of the factor in the group that could be considered as control. There were also no clear recommendations for sample size in cluster analysis in the bioinformatics and marketing literature.19–21 More recently, Dalmaijer’s work suggested that small samples provide sufficient statistical power aiming for N = 20–30 per cluster and Δ = 4 clusters. 22
Results
Ninety-five GPs included 303 patients and attained the expected sample size in one year. One patient was excluded due to an unpredictable death from COVID-19. For three patients, the GP did not know the complete 90-day trajectory. Finally, 299 trajectories were studied.
The mean age of the patients was 82.7 years and 54% (n = 161) were women. The main causes of death were cancer (n = 121 [41%]), heart disease (n = 61 [20%]), and neurological disease (n = 48 [16%]). Less than half of the patients suffered from dementia (128 [43%]) and had a secondary disease that hastened the predictable death (138 [46%]). Most patients were or had been in a couple (258 [89%]) and had children (225 [75%]) (Table 1
Characteristics of Palliative Care Patients in Primary Care, According to the End-of-Life Place Trajectory
Three months before their death, 199 (67%) patients were at home, 76 (25%) were in a nursing home, 20 (7%) in a standard hospital unit, 2 (<1%) in a palliative care unit and 2 (<1%) in a long-term care hospital unit. Sequence analysis showed, per patient, between one (no transfer—n = 114) and eight locations (seven transfers—n = 1), meaning 2.33 transfers on average during the last three months. The development of the patients’ dispersion among the different sites showed few transfers from day 1 to day 44 and a gradual increase until the last 10 days of life. On day 90, 108 (36%) patients died at home, 85 (28%) in a nursing home, 95 (32%) in a standard hospital unit and 11 (4%) in a palliative care unit (Fig. 1). The longitudinal study identified 281 different trajectories. Two were more common. A 90-day stay in a nursing home and a 90-day stay at home represented 59 (20%) and 54 (18%) patients, respectively (Fig. 2). During the 90 days, the mean cumulative time for each location was 54 days for home (max: 90 days), 25 for nursing home (max: 90), 10 for standard hospital unit (max: 75), and less than one day for both palliative care unit (max: 38) and long-term care hospital unit (max: 69).
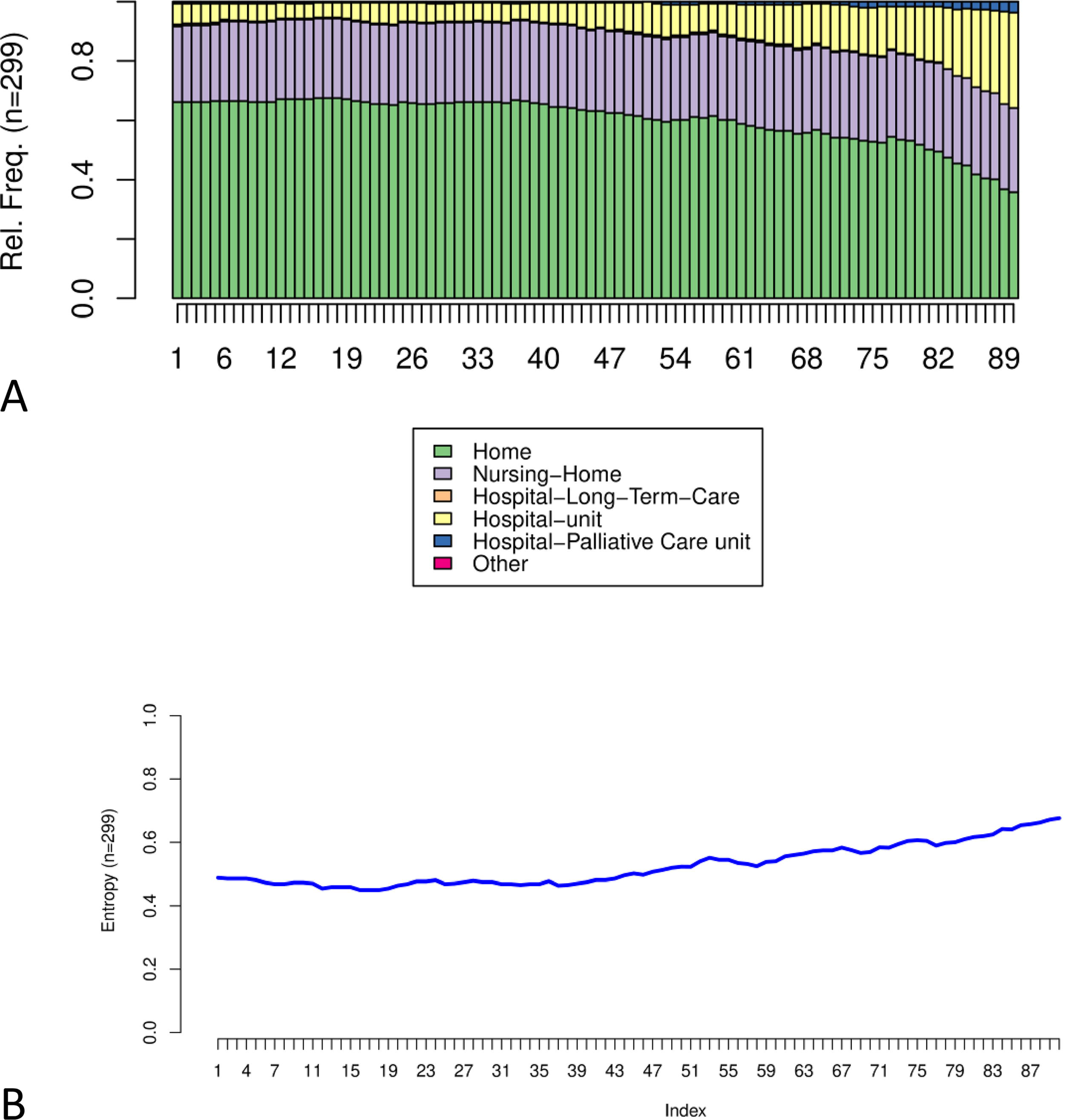
Daily transversal description of the patients’ living place in their last three months of life.
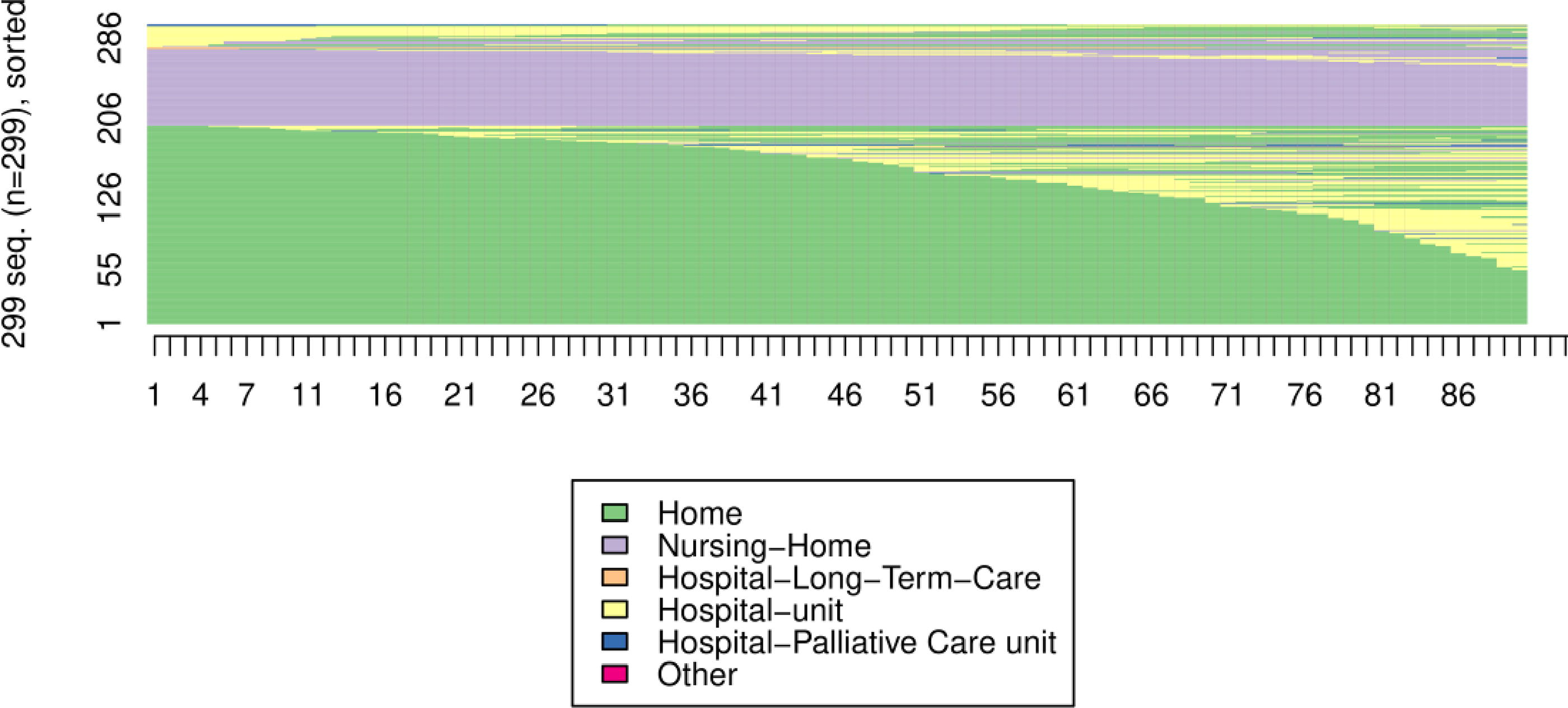
Description of the trajectories of palliative care patients in their last three months of life. Sequence index plot: one line corresponds to one patient and his/her trajectory, that is, the sequence of the successive places of care that the patient occupied during the last 90 days. The trajectories were classified according to the initial location to pre-visualize different trajectory profiles.
Considering the HAC tree and the inertia jump curve, the 3-class HAC model was the most clinically and statistically relevant with the smallest cluster above 30 and the mean intra-class heterogeneity not at maximum (Figs 3, 4).

Hierarchical Ascendant Clustering of palliative care patients’ trajectories.
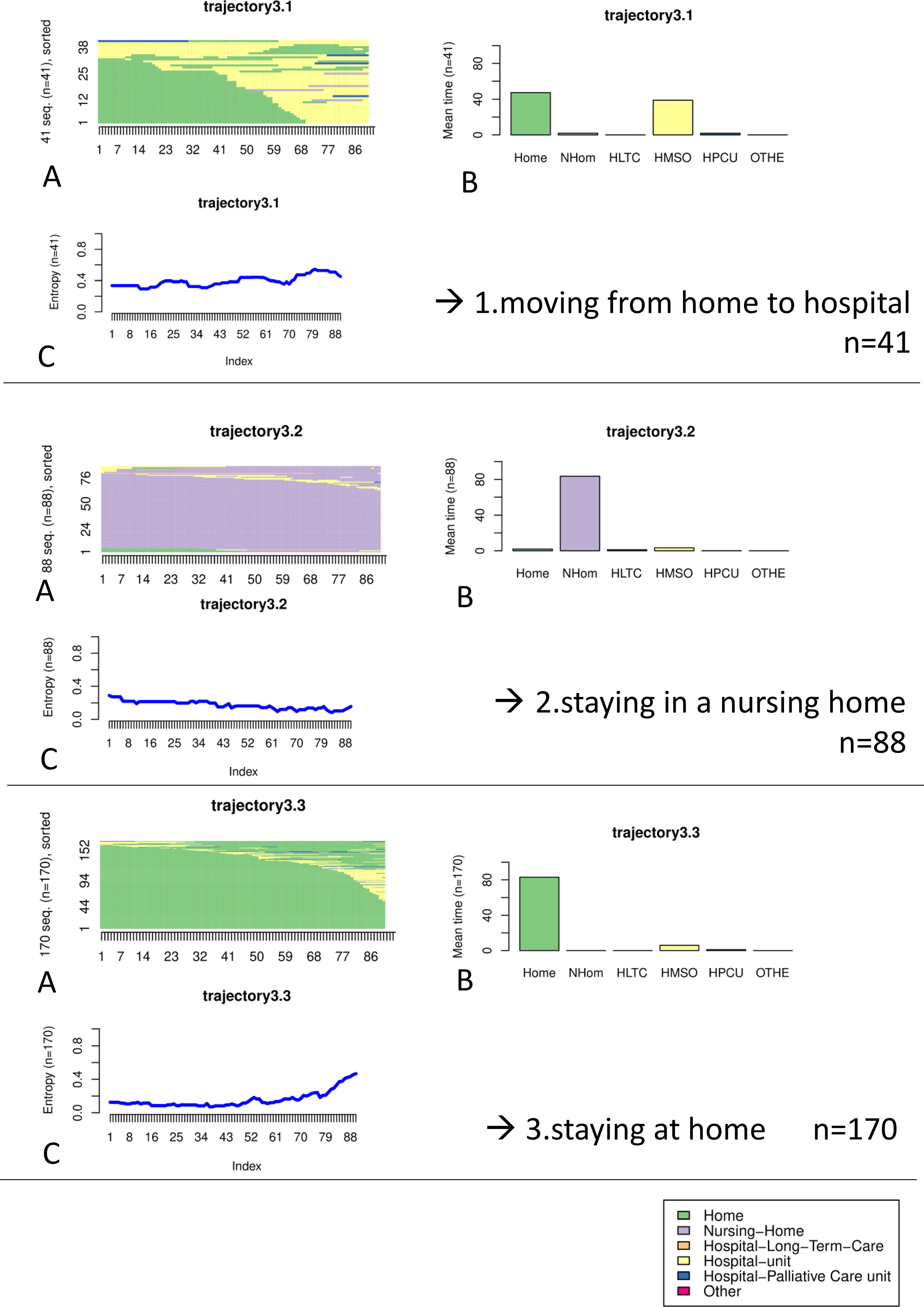
Key trajectories of palliative care patients revealed by 3-class clustering on last-3-month data.
The average time spent in each location confirmed the three selected classes (Fig. 4). In the “staying at home” class (57%; n = 170), patients spent on average more than 80 days at home and less than 10 days in hospital in the last 90 days. In this class, patients hardly moved until the 20th day before death, with a maximum of dispersion at death. In the “staying in a nursing home” class (29%; n = 88), patients spent almost all of their time in a nursing home. The dispersion was quite small and decreased slowly over time; patients moved less and less. In the “moving from home to hospital” trajectory (14%; n = 41), patients spent on average less than 50 days at home and almost as much time in hospital. The dispersion was moderate over the 90 days, although there was a marked increase in hospitalizations in the last 20 days.
The characteristics of patients differed according to the end-of-life place trajectory (Table 1). In the “staying at home” and the “moving from home to hospital” trajectories, cancer and heart disease were the main causes of death. In this population, most patients were married. In the “staying in a nursing home” class, neurological and other diseases were the most common causes of death. More than two-thirds had dementia and most patients were widowers.
Table 2 and Figure 5 show the univariate analysis and the multivariate model including social and medical conditions. In the final model, age was the only factor positively associated with both nursing home and hospital. Using “staying at home” as a reference, we confirmed three main factors of the end-of-life trajectory. Not having a caregiver and having dementia were associated with nursing home stay with OR= 6.98 95% confidence interval (CI) [2.62–18.8], and OR = 4.47 CI [2.07–9.65] respectively. Dementia also limited hospitalization from home (OR = 0.19 CI [0.06–0.61]). Not having children was positively associated with hospitalization (OR = 2.93 CI [1.05–8.13]).

Forest plot of multivariate analysis. The reference was “home.”
Comparison of Palliative Care Patients’ Characteristics According to the Trajectory Using Multinomial Logistic Regression with Home as the Reference
Multivariate multinomial regression highlighted the best model after step-by-step descendant analysis. From the start, several covariates were excluded. Covid-19 and urban areas were irrelevant in univariate. Marital status had clinical links with cohabitation and caregiver. Sex was included because of clinical links with age.
CI, confidence interval; OR, odds ratio.
Discussion
Using HAC, our study identified and quantified three trajectories during the last three months of life: “staying at home” (57%), “staying in a nursing home” (29%), and “moving from home to hospital” (14%). Three factors were associated: dementia, caregivers, and children.
Our results are close to the European figures, except for age. In the EURO-SENTIMELC study, between 32% and 44% of non-sudden deaths occurred at the age of 85 years or older (56% in our study). Between 46% and 54% were female (54% in our study). Cancer rates (37–63%) were similar to our study (41%). In Europe, between 23% and 49% died at home (36% of our population).11,23 In our study, most patients (86%) stayed in the same place during the last 3 months of life. As in another Dutch paper, transfers, especially to hospitals, occurred in the last month. 23 In the end, most patients (64%) died outside the hospital (36% at home and 28% in a nursing home), as in other European studies (61–75%).11,23,24 Deaths at home and in nursing homes were higher than in previous French studies. In 2018, a study, including sudden deaths, revealed that 43% occurred outside the hospital (29% in “home and other”, and 13% in nursing homes). 9 In 2009, only 34% of non-sudden deaths occurred outside the hospital: 17% at home and 17% in nursing homes. 25
A major factor preventing patients from staying in their homes is the absence of a caregiver or family member. The influence of family and informal caregivers has already been identified as a potential factor associated with deaths at home and in nursing homes.26–28 For example, regarding patients with dementia who lack medical decision-making capacity, caregivers and family members are frequently involved in advance care planning and may be asked to decide whether hospitalization is appropriate. 29 Literature shows a positive association between the presence of a partner and home care. 30 Our study suggests a difference between children and informal caregivers. We know that influencing factors, such as pain assessment, may differ between partners and children. 31 Our findings suggest that partners are the caregivers who enable long-term home care in chronic situations while children occasionally support acute crises at home and avoid hospitalization.
Our study confirms dementia is a factor associated with nursing homes. In our population, 43% of patients had dementia, as in other European countries (14–51%). 24 Dementia is already recognized as an element of specific palliative care needs. In a Norwegian study, the researchers excluded patients with dementia because they already knew that the majority died in a long-term care facility. 32 The literature reports how dementia can affect every aspect of end-of-life care.33,34 In a 2016 study, in New Zealand, patients with dementia had more physical distress than patients with cancer, with no age relevance. However, they were as likely to be hospitalized as those with cancer, unlike our results. 35 In 2019, an international systematic review showed that people with dementia were more likely to be hospitalized than others. Although our findings are controversial about the literature, 36 they confirm that palliative care strategies should focus on dementia as much as, or even more than, cancer.
In our final model, age was the only factor positively associated with both nursing home and hospital stays. Older age is known to influence palliative care needs due to frailty and multimorbidity, 37 although there is no agreed definition of old age, with different age thresholds used in the literature such as 65, 70, or 85 years.24,30,38 In addition to the findings on caregivers and family, this highlights the specificities of the end of life in aging and more dependent populations. It confirms the need to increase the number of health professionals in primary care to meet palliative care needs at home and in nursing homes. 39
Our study was original and revealed distinct trajectories through a nationwide population, using reproducible exploratory modeling that considers individual scale. It could help holistic assessment of patient needs and resources in palliative care, including caregivers and a wider range of care settings through primary care. However, focusing exclusively on GPs, we have had to consider a data collection bias. 11 Diagnosis of comorbid dementia could also have been more accurate, for example, using the Mini-Mental State Examination. Finally, the context of the pandemic may also have influenced some end-of-life decision strategies, even in patients with diseases other than COVID19. The hospital was perceived as a less safe place of care, with restrictions on family visits and capacity issues. 40
Beyond the place of death, our study shows that the hospital is not the main living place during the last three months of life. Palliative care plans should consider all possible trajectories early and not be limited to the question of hospitalization or non-hospitalization. The degree of autonomy and decision-making, including the opinion of caregivers and family, should be considered, especially in the case of dementia. Systematic reassessment of neurocognitive status and social environment should be performed as regularly as general clinical assessments of the patient. In addition, palliative care policies need to focus on specific support for patients with dementia at home, and for their caregivers. Further studies on long-term monitoring of places of living and care settings, including primary care, are expected to enable real-time adjustment of palliative care strategies.
Footnotes
Acknowledgment
The authors thank the funders, the integrated staff, and the GPs who participated in the study.
Authors’ Contributions
Conceptualization and project administration were by all authors. Data curation and formal analysis were done by D.N., G.R., and L.R. All the authors contributed substantially to the interpretation of the data, to critical revisions of the article, and final approval of the published version.
Ethics Statements
In accordance with European regulations and French law, our study was a public interest study based on the re-use of data. It complied with the MR004 reference methodology and the recommendation of the National Commission on Information Technology and Civil Liberties.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Two external funds : credits from the Direction Générale de l’Offre de Soins, and credits from the Fondation de France, a foundation recognized as a public utility (contract number : 00101615).