
Abstract
Background:
Accurate prediction of next-day survival in imminently dying patients is crucial for facilitating timely end-of-life decisions.
Objectives:
To develop diagnostic models for predicting next-day survival in cancer patients with a Palliative Performance Scale (PPS) score of ≤20.
Design:
A multicenter, prospective, observational study.
Setting/subjects:
We enrolled advanced cancer patients at 23 palliative care units across Japan.
Measurements:
Clinical signs of impending death were recorded daily after patients’ PPS scores decreased to ≤20, continuing until death or for up to 14 days. The developed models included the prediction of one-day survival-decision tree (P1d-Survival-DT), based on recursive partitioning analysis, the P1d-Survival-organ system score, which utilized a scoring system across four clinical systems (nervous/cardiovascular/respiratory/musculoskeletal), and the early signs model that focused on the absence of two early signs (altered consciousness and liquid dysphagia).
Results:
Of the 1896 patients included in the study, 1396 (74%) reached PPS ≤20. The average age was 73 ± 12 years, with 49% being female. The P1d-Survival-DT model showed next-day survival rates of 91.6% for patients with a response to verbal stimuli and no peripheral cyanosis, and 37.1% for those with no response to verbal stimuli and respiration with mandibular movement. The P1d-Survival-organ system score model revealed a 95.9% survival rate for score = 0, decreasing progressively to 46.7% for score = 4. The early signs model predicted a 95.2% survival rate in patients with normal consciousness and no liquid dysphagia.
Conclusions:
This study successfully developed three distinct models to predict next-day survival in cancer patients with PPS ≤20, offering vital tools for informed decision making in palliative care settings.
Key Message
In this multicenter prospective observational study involving 1396 cancer patients with a Palliative Performance Scale score of ≤20, we developed three diagnostic models to predict next-day survival. The models, based on clinical signs and a scoring system across multiple systems, aim to aid timely end-of-life decisions in palliative care.
Introduction
Accurately predicting impending death is important for clinicians to help patients and families prepare for the end of life, especially in the context of terminal cancer. Previous studies and guidelines identified various signs, systems, and models to detect impending death.1–7 However, a crucial aspect is the prediction of survival within one day, which holds equal importance as predicting death within a few days. This is especially relevant as families often struggle with the difficult balance of spending the maximum time with their loved ones while managing their daily responsibilities. In inpatient settings, it is common for families of dying patients to ask if they can leave the hospital briefly to rest or attend to personal matters. Unfortunately, many families later experience regret over not spending enough time with their loved ones, preparing for death, or being absent at the time of death.8–10 A nationwide survey showed that over 90% of bereaved family members wished to have been present at the moment of death and that meaningful conversations, such as saying “good-bye,” were associated with a lower incidence of depression and complicated grief later on. 11
While previous research focused on predicting imminent death, these predictions over several days can be imprecise, leaving families uncertain about immediate decisions for “today” or “tonight.” Accurately predicting whether a patient will survive to the next day is therefore vital, enabling families to leave comfortably for a day and return in a timely manner. This necessity becomes particularly marked during pandemics, where visitation restrictions impact family experiences, often leading to distress and difficult daily decisions about hospital visits. 12
Therefore, our study aimed to develop models to predict next-day survival in patients with advanced cancer nearing death. We hypothesized that by effectively integrating various signs and systems indicative of impending death, we can accurately predict a patient’s likelihood of surviving to the next day.
Methods
Setting and subjects
This study was part of the East-Asian collaborative cross-cultural Study to Elucidate the Dying process (EASED) and used data collected in Japan. The detailed methodology has been described elsewhere. 7 Briefly, in this multicenter, prospective, observational study, we consecutively enrolled patients with advanced cancer admitted to 23 palliative care units (PCUs) in Japan from January to December 2017, and followed them until their death or six months after enrollment, whichever came first.
Eligibility criteria included patients aged 18 years or older who were diagnosed with locally advanced or metastatic cancer and admitted to PCUs. Exclusion criteria were patients who were scheduled for discharge ≤1 week or patients who declined to participate. For the current analysis, patients with a Palliative Performance Scale (PPS) ≤20 (i.e., bedbound, completely dependent) were included. PPS is a valid and reliable scale that ranges from 0% (death) to 100% (completely asymptomatic) and includes the patient’s function, oral intake, and cognitive status.13–16 We chose PPS ≤20 as an inception point because this is an easily detectable “early sign” of impending death for both clinicians and families, and it leads to families becoming concerned about the vital status of their loved one in the imminent future. 3
This study followed the ethical standards of the Helsinki Declaration and guidelines for medical and health research involving human subjects presented by the Japanese government. Written consent was waived in accordance with the Japanese guidelines for a noninvasive observational study. 17 The institutional review boards of all participating sites approved this study.
Measurements
We collected data on patients’ baseline characteristics at admission and documented clinical signs associated with impending death1–6 daily from the day when PPS decreased to ≤20 until death or 14 days later, whichever came first. In this study, these included two “early” signs (altered consciousness and dysphagia of liquid) and 12 “late” signs (no response to verbal stimuli, no response to visual stimuli, apnea periods, Cheyne-Stokes breathing, peripheral cyanosis, pulselessness of radial artery, respiration with mandibular movement, drooping of nasolabial folds, hyperextension of neck, inability to close eyelids, grunting of vocal cords, and death rattle).3,4 The level of consciousness was recorded using the Japanese version of the Richmond Agitation-Sedation Scale (RASS), a validated 10-point scale ranging from −5 (unarousable) to +4 (very agitated).18–20 For the current study, we used a cutoff of RASS = 0 (alert and calm) as opposed to the other scores, because accurate differentiation of RASS −1 (drowsy) and −2 (light sedation) as well as that of RASS +1 (restless) and +2 (agitated) can be challenging due to the fluctuating nature of consciousness, making the prediction of one-day survival with high probability difficult. Definitions regarding the presence of other signs of impending death were the same as those used in our previous study. 7
Statistical analyses
After conducting descriptive analyses of patient characteristics, we calculated the diagnostic performance of 14 clinical signs for one-day mortality. We used robust variances, which are valid estimates to account for the multiple observations for each patient to obtain point estimates and 95% confidence intervals for each statistic.
To develop diagnostic models to predict one-day survival, we adopted three approaches. First, we used recursive partitioning analyses involving the entire dataset of the 14 clinical signs and performed 10-fold cross-validation. We set the optimal tree size as one with four terminal nodes (i.e., leaves) to ensure clinical utility, 5 and developed a diagnostic model for one-day survival (prediction of one-day survival-decision tree [P1d-Survival-DT]).
Second, we categorized major bedside signs into four systems: nervous (altered consciousness as indicated by RASS score not being 0), respiratory (Cheyne-Stokes breathing, respiration with mandibular movement, and apnea), cardiovascular (peripheral cyanosis and pulselessness of radial artery), and musculoskeletal (inability to close eyelids, hyperextension of neck, and drooping of nasolabial folds).2–5 If any sign was present in each domain, a score of 1 was assigned to the system. The total score (P1d-Survival-organ system score) was calculated by adding the score of each system, ranging from 0 to 4, with a higher score indicating the presence of clinical signs in different systems.
Third, we calculated the sensitivity, specificity, and positive and negative likelihood ratios (LRs) of the combination of the absence of two early signs (RASS = 0 and absence of liquid dysphagia). 3
Comparison of the accuracy of the three models was not considered to be within the scope of the study, as all of them would be clinically useful regardless of differences in their diagnostic properties. We used SAS software, version 9.4 (SAS Institute) for all statistical analyses.
Results
A total of 1896 patients were included in the main study. Data after PPS ≤20 were available for 1396 patients (73.6%) and included in the present study for analysis. The baseline characteristics of the patients are summarized in Table 1. The mean age was 73 ± 12 years, 683 (48.9%) were female, and 399 (28.6%) had gastrointestinal tract cancer. After the first day of PPS ≤20, 1198 (85.8%) patients died within 14 days, and the median length of survival was four days (interquartile range, 2–9).
Patient Characteristics
CCI, Charlson Comorbidity Index; IQR, interquartile range; PPS, Palliative Performance Scale; SD, standard deviation.
Frequency and diagnostic performance
Table 2 shows the frequency of the 14 signs on the day before death, their median onset, and their diagnostic performance in predicting death within one day. Both altered consciousness and liquid dysphagia showed relatively high frequency, early onset, and high sensitivity for one-day mortality. In contrast, 12 late signs showed low frequency, late onset, and overall high specificities for one-day mortality.
Diagnostic Performance of 14 Clinical Signs for Impending Death Within One Day (n = 1396)
CI, confidence interval; LR, likelihood ratio; RASS, Richmond Agitation-Sedation Scale.
Any occurrence of the sign of interest within the last three days of life among patients who showed PPS ≤20 and died in palliative care units.
Onset from death backward.
We computed the sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio for each sign of one-day mortality with data from all 1396 patients who showed PPS ≤20 during admission to palliative care units. We constructed a 2 × 2 table with one observation per patient based on the presence or absence of a particular sign during a randomly sampled day and on whether that patient died on the next day (i.e., gold standard); we then calculated the sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio. To account for the multiple observations for each patient, we resampled our data 100 times to obtain an average and a 95% confidence interval for each statistic.
The prediction of P1d-Survival-DT
Figure 1 shows the final model using three variables and four terminal leaves for one-day survival (P1d-Survival-DT). The next-day survival rates for individuals with response to verbal stimuli and no peripheral cyanosis, response to verbal stimuli and peripheral cyanosis, no response to verbal stimuli and no respiration with mandibular movement, and no response to verbal stimuli and respiration with mandibular movement were 91.6%, 76.6%, 75.3%, and 37.1%, respectively (overall accuracy, 85.2%).
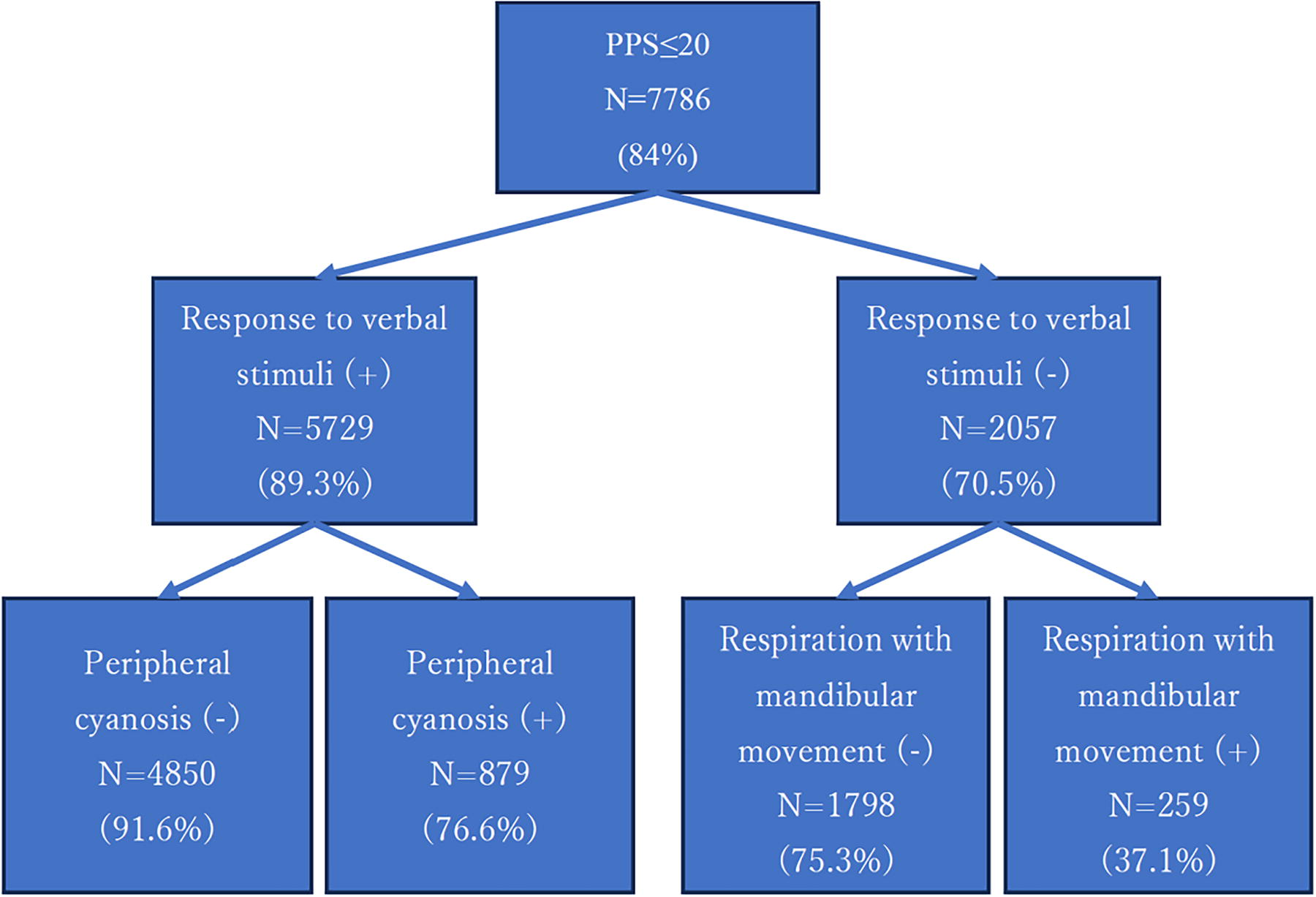
Recursive partitioning model for one-day survival in patients who showed PPS ≤20 during admission in palliative care units: P1d-Survival-DT. The main model was based on three variables and had two levels and four leaves. The diagnostic accuracy (1–error rate) was 85.2%. For each node, the number of patients fulfilling the criteria is shown along with the one-day survival rate (in parentheses). P1d-Survival-DT, prediction of one-day survival-decision tree; PPS, Palliative Performance Scale.
A system-based prediction score: the P1d-Survival-organ system score
Overall, 95.9%, 90.5%, 81.4%, 70.0%, and 46.7% of patients with P1d-Surval-organ system score points of 0, 1, 2, 3, and 4, respectively, survived to the next day. Table 3 summarizes the diagnostic performance of the P1d-Survival-organ system score with various cutoff points. As the cutoff points decrease, the specificity and positive LR for survival to the next day increase, while the sensitivity decreases. The specificity and positive LR of a P1d-Survival-organ system score of zero were 97.4% (95% CI, 96.5–98.3) and 4.36 (95% CI, 3.01–6.32), respectively.
Performance of Impending Death Categories in the Prediction of One-Day Survival
Prediction of next-day survival using two early signs: early signs model
Of a total of 7786 observations with PPS ≤20, a normal RASS score and no liquid dysphagia were noted in 562 observations, and an abnormal RASS score and/or liquid dysphagia were seen in 7224 observations. Overall, 95.2% of the former and 83.5% of the latter survived to the next day. The sensitivity, specificity, positive LR, and negative LR of a normal RASS score and no liquid dysphagia were 8.2% (95% CI, 6.3–10.0), 97.8% (95% CI, 97.0–98.6), 3.68 (95% CI, 2.45–5.55), and 0.94 (95% CI, 0.92–0.96), respectively.
Discussion
Main findings
To the best of our knowledge, this is the first study to develop diagnostic models for predicting survival to the next day with high probability in imminently dying cancer patients in a PCU setting. Previous studies on prognostic tools mainly focused on predicting death within a certain time period such as months, weeks, days,16,21–23 or within a few days.1–7,24 Regarding prediction of the next-day vital status, we previously reported moderate diagnostic performance of a one-day surprise question among patients with advanced cancer (sensitivity of 82.0% and specificity of 45.5%). 25 While predicting death within a certain time frame, such as within a few days, is useful for clarifying overall goals of care, it does not necessarily aid in day-to-day decision making by patients and their families. In contrast, the prediction of survival to the next day is more important for informing families who desire a balance between staying with their dying loved one in the hospital and taking care of their own needs. We have shown that the absence of two late signs (no response to verbal stimuli and peripheral cyanosis), system-based P1d-Survival-organ system score of 0, and absence of two early signs of impending death (altered consciousness and liquid dysphagia) can each help clinicians predict with a high probability that the patient will most likely survive to the next day.
Features of the diagnostic models
The first important finding was that the response to verbal stimuli and no peripheral cyanosis can predict next-day survival in up to 91.6% of cases (P1d-Survival-DT). This model is clinically useful because of its simplicity. Clinicians can easily assess responsiveness to verbal stimuli by speaking to a patient and peripheral cyanosis at a glance at the bedside. These can be evaluated in settings other than hospitals (e.g., home and nursing home) and by any professional or family caregiver.
The second important finding was that a total P1d-Survival-organ system score of zero provides good prediction performance for next-day survival. A score of zero essentially indicates the absence of major late signs. Considering that all patients in our analysis developed PPS ≤20, an early sign of impending death, a positive LR close to 5 is quite high and suggests usefulness in clinical practice.3,5 On the other hand, the fact that only 2.6% of the patients had a score of zero may limit its use due to its low-level applicability.
Of note, the absence of two early signs (altered consciousness and liquid dysphagia) showed a moderate diagnostic performance for next-day survival with a positive LR of 3.68. A previous study showed that the sensitivity of these two early signs (RASS ≤−2 and dysphagia of liquids) in predicting death within three days was relatively low, ranging from 41% to 51%. 3 In our cohort, the sensitivity of these two signs in predicting death within three days was 74% to 81%. 7 To further improve the diagnostic performance of predicting the vital status within one day, we modified the cutoff of RASS to 0 or other values. Our results indicate that these two signs in combination may be better to rule out death within one day, while its performance remained moderate. This may be in part because early signs may not be as closely associated with life-or-death discrimination. 3 Another possible interpretation is that all patients already had one early sign (PPS ≤20) and were therefore considered to have entered the imminent death phase; thus, the diagnostic performance of the other two early signs may have been diluted.
Clinical implications
All three models can help clinicians predict next-day survival immediately upon a request from patients or families at the bedside. Patients may be waiting for a family member to visit from afar, or close family members who want to be with their loved one as they draw their last breath may wish to leave the hospital for the night. When pressed for time, clinicians are advised to focus on only two late signs (response to verbal stimuli and peripheral cyanosis). If they have time for a comprehensive assessment of four systems, P1d-Survival-organ system score of zero provides an additional level of confidence that a patient will survive to the next day. Finally, the absence of two early signs (altered consciousness and no liquid dysphagia) can be used immediately after a patient develops PPS ≤20, even before they show late signs.
Future directions
After external validation, these diagnostic models could be widely used in daily practice to inform patients close to death and their families. While we focused on the next-day vital status, prediction of function (e.g., how long patients can think or communicate with families) may be more important to help them fulfill their wishes and complete unfinished business.26,27 Future studies should include the functional prognosis as well as vital status, and explore whether such predictions will improve clinical outcomes for patients and their families. Finally, the clinical signs measured in our study are part of the complex phenomena of impending death, and may not fully capture subtle physical changes during this phase. The use of continuous monitoring of comprehensive physical signs by information technology and analysis using artificial intelligence may markedly improve the continuous prediction of next-day survival.
Strengths and limitations of the study
The strengths of our study include a large sample size from more than 20 institutions across Japan, the novel idea of predicting next-day survival in the last days of life, use of explicit definitions of clinical signs based on the previous studies,3–5 and use of robust statistical analyses that facilitated highly clinically interpretable results.
However, several limitations should be noted. First, we included only cancer patients who were admitted to PCUs in Japan, where interprofessional care for the dying is provided. Further studies should determine whether the dying process is similar in other settings (e.g., general ward, home) and noncancer diseases. Second, the daily assessment of clinical signs by palliative care physicians may have limited the resolution of the data, as many signs of impending death may develop a few hours before death. 1 In addition, data on clinical signs were not collected in patients who died on the first day of PPS ≤20. Thus, the presence of signs of impending death may have been underestimated, especially in predicting survival within one day. However, the daily assessment allowed physicians to report based on observation throughout the day, even for signs developing intermittently. Third, we did not assess the inter-rater reliability of the clinical signs. However, participating physicians received an orientation prior to commencement and support throughout the study. Fourth, we collected impending death signs only after patients had a PPS of 20 or less, and thus the diagnostic performance of these scales in more imminently dying patients (e.g., those with a PPS of 10) remains unknown.
Conclusion
Using early and late signs of impending death, we developed three diagnostic models for next-day survival in patients with PPS ≤20. These may further enable clinicians to assist patients and their families in making important decisions and preparing for the last day(s) of life.
Footnotes
Acknowledgments
This study was performed in the East-Asian collaborative cross-cultural Study to Elucidate the Dying process (EASED), and the authors sincerely appreciate all the investigators. The authors also thank Dr. Junko Nozato and Mr. Keisuke Ariyoshi for their generous support in developing the case report form.
Data Statement
The study data are available from Masanori Mori upon reasonable request.
Funding Information
This study was supported in part by a Grant-in-Aid from the Japan Hospice Palliative Care Foundation and JSPS KAKENHI (grant numbers 16K15418, 18H02736, and 20K20618).
Author Disclosure Statement
The authors declare no relevant conflicts of interest.