
Abstract
Background:
People with rheumatic diseases suffer from serious complications of their illness, though little research is available on the utilization of palliative care (PC) for this population.
Methods:
We performed a retrospective chart review of patients referred to outpatient PC from a single academic rheumatology practice over five years and reviewed patients seen concurrently by rheumatology and PC in the inpatient setting over one year.
Results:
Of 18,441 patients seen in the outpatient rheumatology practice over five years, 11 (0.06%) patients were referred to PC by rheumatology providers. Of the 527 patients seen by inpatient rheumatology over a year period, 14 (3%) had rheumatic disease and were also seen by inpatient PC. Average time to death was 190 days among outpatients and 139 days among inpatients.
Conclusion:
Patients with rheumatic disease are rarely referred to PC despite high morbidity and mortality. Interventions are needed to improve this gap in care.
Introduction
Palliative care (PC) emphasizes quality of life and relief of suffering for people with serious illness. Benefits of PC, such as reduced symptom burden, improved quality of life, and more timely advance care planning (ACP) discussions, have been demonstrated in diverse medical specialties.1–5 However, little is known about the role of PC in rheumatology. Despite the rapid expansion of treatment options in rheumatology over the past several decades, many patients with rheumatic diseases continue to suffer significant morbidity and mortality, particularly in patients with systemic lupus erythematosus (SLE), vasculitis, and scleroderma (SSc).6–12 The objective of this study is to describe referral patterns to PC for patients with rheumatic diseases. To our knowledge, this is the first study to examine PC referrals made by rheumatologists.
Methods
An electronic medical records (EMR) tool was used to identify patients for retrospective chart review. PC referrals from the outpatient and inpatient settings were analyzed separately given differences in acuity. For outpatient referrals, patients seen at Duke University Health System’s (DUHS) rheumatology clinics over the preceding five years (October 19, 2018–October 18, 2023) were filtered by referral to ambulatory PC. For inpatient referrals, patients seen by the inpatient rheumatology consult team over the preceding one year (October 5, 2022–October 4, 2023) were filtered by co-consultation with inpatient PC. Inpatient consults were further subdivided according to whether the patient was diagnosed with a rheumatic disease; those with a rheumatic disease were analyzed fully. Chart review was performed through May 1, 2024.
Chart review was performed to identify demographics, primary rheumatic disease, prior ACP, indication for referral, associated referral diagnosis, and time to death. For inpatient consultations, we also identified whether rheumatology initiated the PC consultation. ACP was captured through the use of an EMR ACP tool. “Associated referral diagnosis” refers to the ICD-10 diagnoses attached to the outpatient order; on the inpatient side, orders are not linked to a diagnosis, and thus the associated diagnosis was determined by chart review of progress notes from when the referral was placed. “Referral indication” refers to the reason for PC consultation as selected by the referring clinician; in our EMR, indications include ACP/goals of care, anxiety/depression, end-of-life planning/hospice, pain, symptom management, or other. Multiple indications can be selected. Demographics of patients from all outpatient and inpatient rheumatology encounters during the same time periods were obtained for comparison with the referred population. Data were analyzed in Excel.
Results
Of the 18,441 patients seen in rheumatology clinics over the preceding five years, 11 (0.06%) were referred to ambulatory PC. Of the 527 inpatients seen by rheumatology over the preceding one year, 29 (6%) were also seen by inpatient PC. Fifteen of these patients were not found to have a rheumatic disease, leaving 14 out of 527 (3%) inpatient consults for full chart review. Demographics and disease characteristics are shown in Table 1. Most referred patients were female. Black patients represented more than one-third of referred outpatients and greater than half of inpatients, slightly higher than the general outpatient and inpatient populations. Patients had a wide range of primary rheumatic diagnoses, and there was no prevailing disease among referrals. Only one outpatient (9%) and one inpatient (7%) had ACP before seeing PC.
Patient Demographics and Primary Rheumatic Disease and Disease Associated with Palliative Care Referral
*Subtypes of rheumatic disease indications, shown in italics, are reported as percentage of total rheumatic disease indications associated with referral to PC (n = 3 for outpatient, n = 8 for inpatient), rather than as percentage total of all indications. CRPS = chronic regional pain syndrome; CTD = connective tissue disease; SLE = systemic lupus erythematous.
For outpatients, rheumatic disease was an associated referral diagnosis in only a quarter of cases (n = 3, 27%); cardiovascular disease was the most common associated diagnosis (Table 1). In contrast, rheumatic disease comprised the majority of associated diagnoses for inpatient referrals (n = 8, 57%), though rarely did the inpatient rheumatology team initiate the PC referral (n = 2, 14%).
Indications for PC consultation among outpatients and inpatients are shown in Figure 1. Anxiety and depression were frequently an indication for referral in outpatients (n = 7, 64%), but they were never an indication for inpatients. Pain was also a common indication for outpatient consultation (n = 8, 73%). ACP (n = 7, 50%) and symptom management (n = 7, 50%) were the most common indications for inpatient consultation. Patients could have more than one indication for referral.
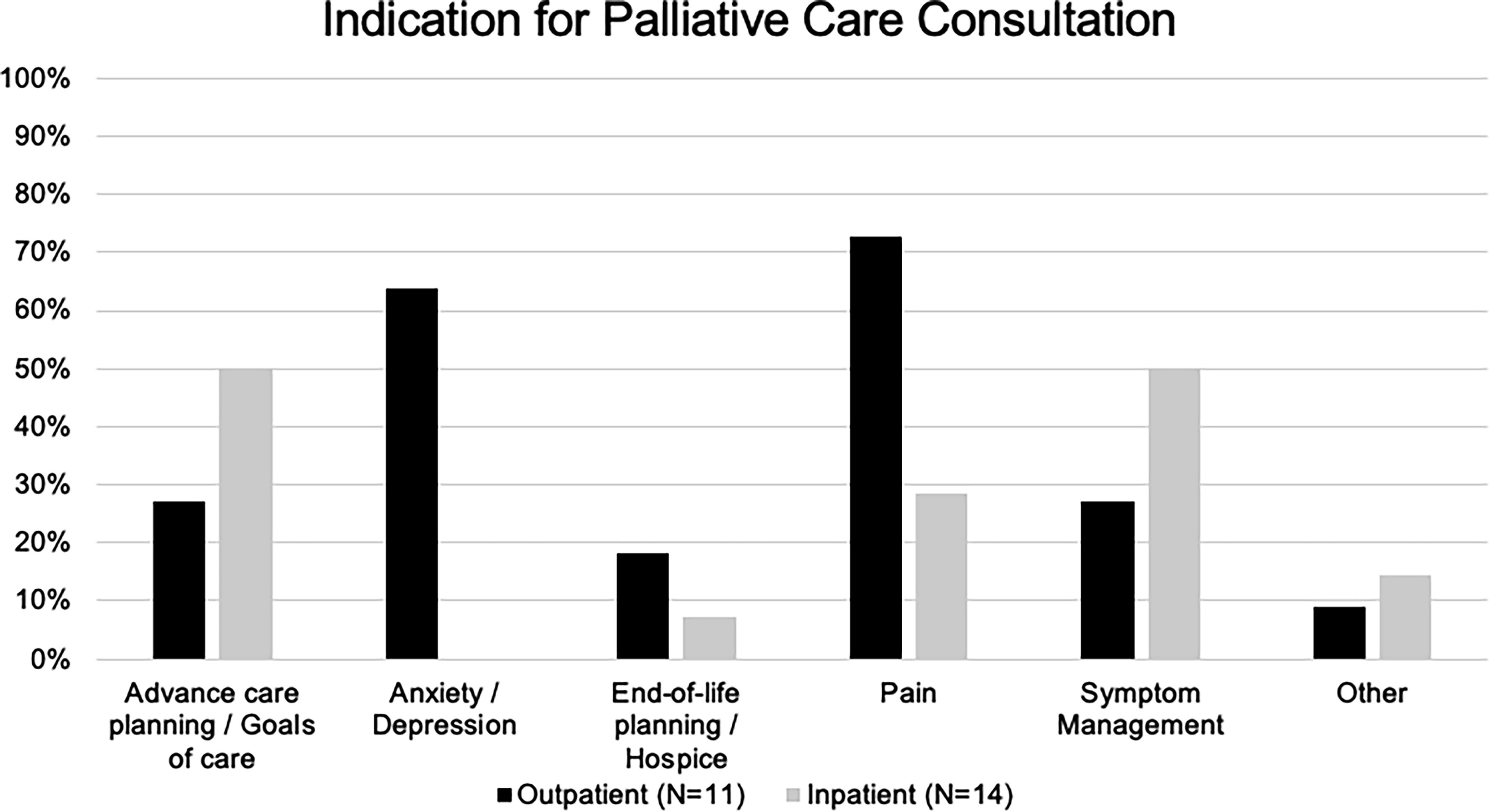
Indication for palliative care consultation, shown by outpatient and inpatient palliative care referrals.
Nearly half of outpatients (n = 5, 45%) were deceased by the time of chart review (Fig. 2); average time of death following outpatient referral was 190 days (range 76–478). No inpatients died during hospitalization, and seven (50%) were deceased at the time of chart review; the average time of death following hospitalization was 139 days (range 1–332).

Number of days to death following outpatient referral or inpatient hospital discharge, shown by outpatient and inpatient palliative care referrals.
Discussion
Data from this single academic center study demonstrate that rheumatology patients are rarely referred to PC, and at the time of referral, rates of ACP are low and mortality is high, with median time to death occurring around 6 months or less. These findings are mirrored by previously published data in patients with SLE in a United States inpatient sample. 13 and patients with all classes of rheumatic disease in an Asian population. 14 The high mortality rate seen in our study suggests that patients are being referred late to PC; in addition, our finding that fewer than 1% of outpatients are referred to PC despite the high morbidity and mortality demonstrated in rheumatic disease literature, with standardized mortality ratios ranging from 2 to 12 times the general population depending on factors such as disease type and age,6–12 suggests that PC is currently underutilized in patients with advanced rheumatic disease.
The demand for PC has increased over the past decades, with models projecting exponential need for PC as our population continues to grow and age. 15 Primary PC (compared with specialist PC) has been proposed as a way to expand the reach of palliative care practices. 16 Our finding of low rates of ACP at the time of referral suggests that primary PC discussion about goals of care is rarely occurring in rheumatology, highlighting an opportunity to design interventions that enhance primary PC education for rheumatologists. Previously published data found that few rheumatologists have received PC education and almost none have received rheumatology-specific PC education, 17 though further studies are needed to better understand this education gap.
Our study also found that patients are referred to PC for a variety of rheumatic and nonrheumatic diagnoses, though these data only reflect a small pool of patients in a single center. Pain and anxiety/depression were common reasons for outpatient PC referral, which correlates with literature demonstrating a high prevalence of these comorbidities in people with rheumatic disease.12,18–21 Black patients comprised more than a third of the referred population, and it is well known that Black patients with rheumatic disease suffer more serious manifestations and have a higher mortality rate compared to non-Black patients.6,22–25 Among rheumatic diagnoses, there was no discernible leading diagnosis. However, a recent study demonstrated that in a large SSc registry, almost three-quarters had sufficiently high symptom burden to warrant referral to PC. 9 These findings suggest that patients with SSc may benefit from early integration of PC into routine practice. In addition, people with rheumatic disease suffer from higher rates of comorbidities such as cardiovascular disease 26 and malignancy,27,28 which may also necessitate PC interventions. Further studies are needed to better describe which rheumatic diseases may benefit from PC.
Several factors may contribute to underutilization of PC in rheumatic disease. Misperceptions about the purpose of PC,29,30 lack of awareness about benefits of PC, 30 and insufficient PC training, 31 all contribute to underutilization in other specialties, and it is likely that similar factors are present in rheumatology. In addition, the trajectory and prognosis of many rheumatic diseases are uncertain, further challenging the issue of who and when to refer. Identifying and addressing barriers to referral, including insufficient education about PC, may improve current utilization rates of PC in the rheumatic disease population. Further research should explore challenges experienced by PC clinicians when caring for rheumatology patients, specifically probing for knowledge deficits and quality of training around rheumatic disease.
Our study has several limitations. It occurred at a single tertiary academic center, and thus, findings may be biased toward a more advanced disease population and may not be generalizable to other practice settings. Additional studies with a larger cohort and matched controls could further refine referral practices and compare characteristics to non-referred patients. Rates of ACP were identified through documentation with a specific ACP EMR tool, and thus some ACP conversations may not have been captured. In addition, this study examined outpatient referrals from rheumatology clinics alone, rather than from all medical clinics, and thus the rate of referral to PC may be higher than reported if additional specialties referred patients with rheumatic diseases to PC. Finally, some factors of interest, such as the associated diagnosis for referral, were done by chart review and may not completely capture the full details leading to referral.
Conclusion
Patients with rheumatic disease are rarely referred to PC, and rates of ACP are low. By the time patients are referred, mortality is high. These findings suggest that PC is underutilized and utilized late in patients with advanced rheumatic disease. A future research agenda should include surveying clinicians in rheumatology and palliative medicine; querying patients with rheumatic disease about their perceptions and fears around PC; and implementing educational and interdisciplinary clinical interventions. Collaboration between rheumatology and PC is needed to foster integration of these specialties and improve health outcomes for patients with rheumatic disease.
Institutional Review Board Statement
Determined exempt by Duke University Health System IRB, protocol ID: Pro00114459.
Footnotes
Author Disclosure Statement
J.K. and C.J. have no relevant disclosures.
Funding Information
S.H. has received grant funding from the Rheumatology Research Foundation (related to this work) and Aurinia Pharmaceuticals (unrelated to this work). D.L. receives funding from the Rheumatology Research Foundation and Pfizer for medical education and quality improvement work unrelated to this project. He has also served as a consultant to Sanofi and Pfizer.