
Abstract
Background:
Chronic intravenous inotropic support (CIIS) is recommended as palliative therapy for end-stage heart failure (HF) but is underutilized in hospice settings.
Objectives:
This study evaluates outcomes for patients on CIIS receiving hospice care.
Design:
Retrospective cohort study using electronic health records of patients on CIIS admitted to hospice.
Setting/Subjects:
Twenty-one patients admitted to a mid-Atlantic hospice between 2018 and 2022.
Measurements:
Data collected included demographics, inotropic therapy details, hospice length of stay (LOS), hospitalizations, and medication usage.
Results:
The mean age was 72.9 years; 67% were on milrinone. Patients had a mean hospice LOS of 49.6 days, with 66% experiencing no hospitalizations. Only 24% of patients required high-dose opioids. 24% of patients were discharged alive from hospice, and 52% died at home.
Conclusion:
Caring for patients on CIIS in hospice appears feasible and may portend some benefits to patients. Further research is warranted to confirm these findings in a prospective observational cohort.
Introduction
Chronic intravenous inotropic support (CIIS) as palliative therapy carries a Class IIb recommendation per the 2022 ACC/AHA Heart Failure (HF) Guidelines. 1 CIIS as palliative therapy, when compared to controls, improves NYHA functional class without impacting survival. 2 Although the principles of CIIS as palliative therapy align with the hospice philosophy of care, only 57% of hospices offer CIIS. 3 Barriers to CIIS in hospice include lack of experience, cost, and the limited evidence supporting its use. This study was conducted to evaluate the outcomes of CIIS for patients with end-stage HF receiving hospice care.
Methods
We conducted a retrospective cohort study of 21 adult patients on CIIS admitted to a mid-Atlantic hospice between 2018 and 2022. Data abstracted included demographics, inotrope type, management (weaned, maintained, or discontinued), hospice length of stay (LOS), hospitalizations, location at death, opioid and diuretic doses, and interdisciplinary team visits. The hospice agency prescribed CIIS; at hospice admission, the medication/dose of CIIS was the same as the previous effective medication/dose that was prescribed by the advanced HF cardiologist. Opioid doses were classified as low (equivalent to 5 mg PO morphine q3h PRN; ≤40 oral morphine equivalents [OME]) or high (greater than 5 mg q3h PRN; ≥40 OME). Diuretics were classified similarly based on furosemide dosing (greater or less than 80 mg PO furosemide). The study was approved by the MedStar Health Research Institute IRB.
Results
Among 21 patients (mean age 72.9 years; 62% male), 48% identified as White and 52% as Black. Fourteen patients (67%) received milrinone, and 7 (33%) received dobutamine. Most patients (66%) had no hospitalizations during hospice admission; the mean hospice LOS was 49.6 days (SD 102.4) (Fig. 1). The interdisciplinary hospice team visited each patient an average of 1.2 (SD 1.1) times daily. Twenty-four percent were discharged alive; 52% died at home, 14% died at inpatient hospice, and 10% died in an acute care hospital. Low-dose opioids were prescribed for 76% and high-dose for 24%; 19% were prescribed no diuretics, 48% low-dose, and 33% high-dose. Most patients (66%) maintained their CIIS dose during hospice; 29% had a dose reduction/weaning, and 5% had a dose increase.
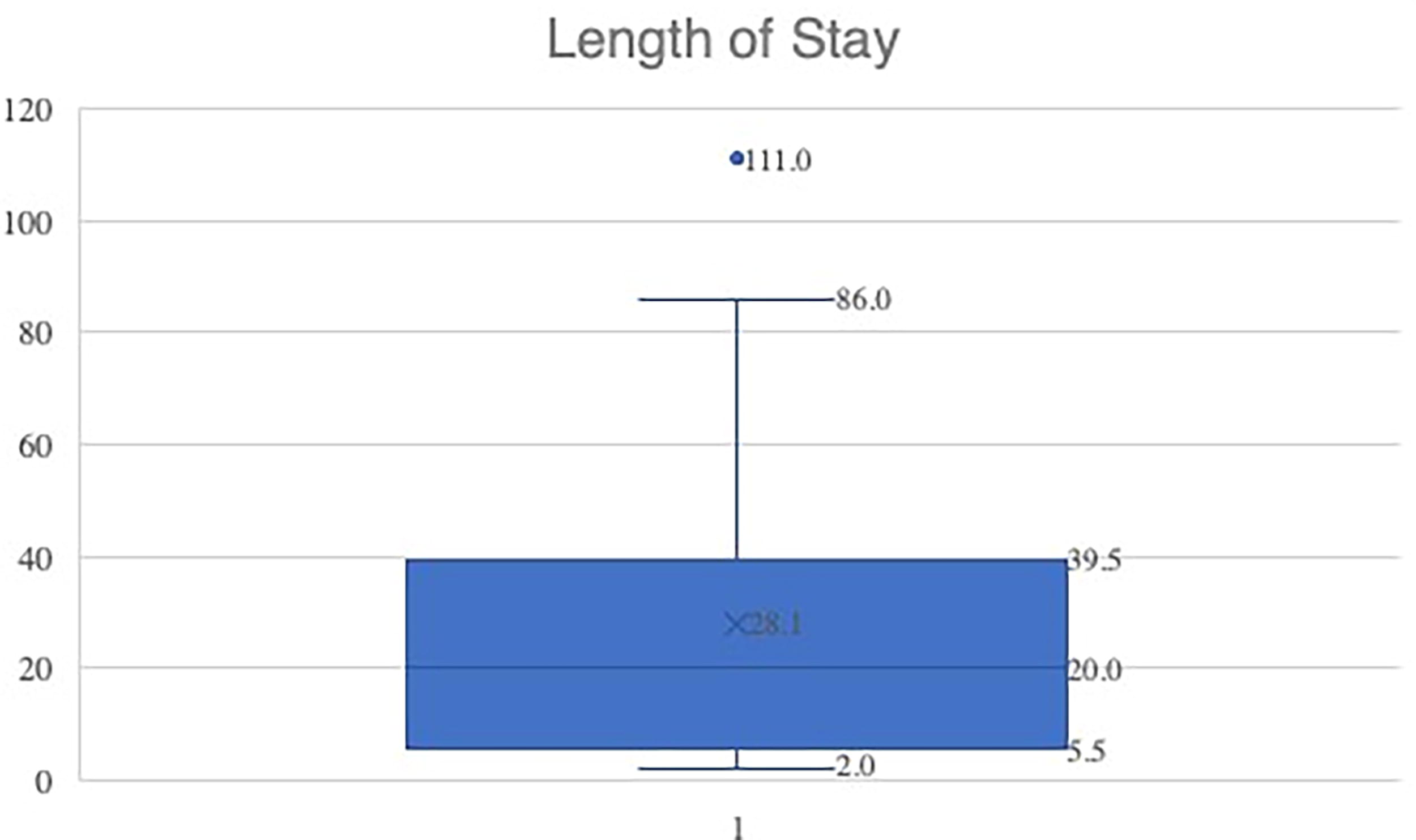
Length of stay for 20 patients (one outlier with 479 days was excluded in this graph). X = mean. ● = Outlier. Box-and-whisker plot with range of lower to upper extreme, lower quartile, median, and upper quartile depicted by the box.
Discussion
To our knowledge, this is the first study detailing the experience of a hospice agency caring for patients with end-stage HF who are treated with CIIS. We report that the majority of patients are prescribed low-dose opioids. We also report a long hospice LOS compared to previously published data on patients with HF, which reports a median LOS of 11 days. 4 However, patients on CIIS may have a higher rate of hospital readmission, likely attributable to the medical complexity of the intervention; in our cohort, 33% of patients were rehospitalized, compared to only 4% 30-day readmission rate in a national cohort. 4 30% of home hospice patients with HF experienced a live discharge, similar to the rate we describe in our cohort. 5
Opioids and diuretics are the cornerstones for managing dyspnea related to end-stage HF. Inotropes can improve end-organ perfusion and, therefore, alleviate ischemic pain and lung congestion, which may decrease dyspnea and reduce opioid requirements. Our results suggest that CIIS may alleviate symptoms of end-stage HF, potentially reducing opioid requirements and associated side effects. The implications of CIIS as an opioid-sparing agent warrant further exploration.
Alleviating the symptoms associated with end-stage illness is congruent with the hospice philosophy of care. However, caring for patients on CIIS in the hospice setting can be expensive. The hospice LOS for patients in this cohort on CIIS was greater than previous studies that report median survival of only 11 days. 4 This additional prolongation in hospice LOS may mitigate the additional costs to hospice for providing CIIS.
Limitations include the study’s single-center design and lack of a matched control group, limiting the assessment of complications or effects on survival. A limitation to studying a population on home hospice is that we do not have granular information regarding medication administration, especially for medications that are ordered PRN.
Our study generates new questions and hypotheses that CIIS may be associated with reduced opioid use and increased hospice LOS; these findings should be evaluated further in an observational, prospective cohort study of patients admitted to hospice with and without CIIS. Our findings highlight the potential of CIIS in improving end-of-life care for patients with advanced heart failure.
Footnotes
Acknowledgments
The study authors thank Dr Samer Najjar for his contributions to study design. The authors thank the staff at Hospice of the Chesapeake for their assistance with data acquisition.
Authors’ Contributions
U.A.E.: Methodology (supporting), investigation (supporting), writing—original draft (equal); S.H.R.A.: Investigation (supporting), writing—original draft (equal); C.T.: Investigation (supporting), writing—original draft (equal); K.M.A.: Conceptualization (supporting), writing—review and editing (equal), supervision (supporting); H.G.: Conceptualization (supporting), writing—review and editing (equal); supervision (lead); F.H.S.: Writing—review and editing (supporting); E.B.: Conceptualization (supporting), investigation (supporting), writing—review and editing (equal), supervision (supporting); A.R.: Conceptualization (lead), methodology (lead), investigation (lead), writing—original draft (equal), writing—review and editing (equal), supervision (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. A.R.’s time and effort are supported in part by an institutional research grant.