
Abstract
Background:
Clinical teams face many barriers to communicating with the parents/caregivers of patients experiencing an acute decline. Outside of these time-critical situations, clinicians often can iteratively assess and cultivate prognostic awareness of the patient and parents/caregivers and elicit values and goals over multiple conversations. However, in emergent circumstances, a modified approach to support prognostic awareness is necessary.
Methods:
We developed a clinical practice guideline for time-critical decision making through consensus with an interprofessional group.
Results:
Our proposed strategy starts with a concise statement naming the situation and urgent decision to be made, followed by an outline of the medical options with individualized clinical contextualization for the child and/or parents/caregivers. Finally, incorporating responses (verbal and nonverbal) from the parents/caregivers, recommendations for next steps are offered, with a check-in to ensure agreement with the recommendation(s).
Conclusion:
This framework is intended to supplement, not replace, existing guidelines for eliciting values and making medical recommendations in time-critical situations.
Case
Jose is a newborn with obstructed supracardiac total anomalous pulmonary venous return and an intracranial hemorrhage (ICH). While the congenital heart disease was diagnosed prenatally and the family knew he would definitely need corrective surgery to redirect the pulmonary venous return, they were counseled that his condition could fall on a spectrum from being able to feed for days/weeks prior to surgery, to being critically ill immediately after birth where there is a high mortality with surgery. He presents shortly after birth in extremis with severe oxygen desaturation on maximal ventilatory support and a decision needs to be made about operating immediately.
Background
While pediatric mortality rates in the United States remain low, the intensive care unit (ICU) remains the most common location of death for children. 1 Clinicians may face extraordinary challenges in fostering prognostic awareness, and numerous barriers are often overcome to deliver high-quality end-of-life (EOL) care in critical care environments. 2 High acuity environments such as the ICU can create time constraints, which impede the prognostic discussions and values exploration necessary to prepare patients and parents/caregivers for complex decisions. As a result, important conversations regarding poor or worsening prognosis may be deferred until critical clinical decisions are unavoidable. This is exacerbated by growing prognostic uncertainty given technological advancements, expanding the scope of available interventions. Shift-work staffing may also impact the development of the therapeutic alliance between clinicians and patients or parents/caregivers. Thus, pivotal conversations may need to be initiated by new faces or covering team members who lack longitudinal relationships with the patient or parents/caregivers. Compounding these challenges, many ICU clinicians report inadequate communication training and discomfort with serious illness conversation. 3
Each patient and family is unique, requiring tailored communication approaches. 4 ICU clinicians frequently manage acute illnesses/injuries in previously healthy children, where parents/caregivers need to make decisions without prior consideration of the possibility of their child’s death. These providers also care for children with medical complexity, whose parents/caregivers may have had prior conversations about the possibility of their child’s death. After experiencing many prior life-threatening episodes, these parents/caregivers may develop “alarm fatigue” from similar prior serious illness discussions. When children do recover, a narrative emphasizing past inaccurate prognostic assessments may lead parents/caregivers to underestimate the gravity of the current situation and may lead clinicians to avoid delivering clear recommendations during subsequent acute presentations.
Integration of primary and subspecialty palliative care has the potential benefit for all ICU patients.5,6 Even as subspecialty palliative care teams are increasingly available, primary palliative care skills such as discussing prognosis or changes in illness trajectory and supporting parents/caregivers developing a subsequent care plan, remain a core competency for ICU clinicians. 7 Additionally, these conversations may occur when other interprofessional clinicians (i.e., social work, chaplaincy, palliative care) are not readily available. 8 Guidelines for early advance care planning and discussion of prognosis are well-established in oncology, for navigating pediatric serious illness, and discontinuing extracorporeal membrane oxygenation.9–13 However, there is limited guidance for how to conduct time-critical conversations in ICU settings.
Outside of ICUs, clinicians often have the opportunity to assess and gradually cultivate prognostic awareness and explore goals and values via iterative conversations over days, weeks, or years.10,13,14 However, the urgency of time-pressured circumstances around acute clinical deteriorations necessitates a modified approach, as even if present during critical events, fully comprehending the clinical implications is infeasible for most parents/caregivers. Thus, we propose a structured communication guide to support clinicians in rapidly fostering prognostic awareness during emergent decision making.
Framework Development
We developed an interdisciplinary clinician-derived communication guide as a practical resource for pediatric critical care clinicians using an iterative, consensus-driven approach. The emphasis was on enhancing prognostic awareness within a timeframe of minutes when urgent decisions need to be made for patients experiencing an acute clinical decline. We first held a brainstorming session involving an interprofessional group from multiple institutions with communication experience in the fields of pediatric palliative medicine, oncology, cardiology, and pediatric intensive care. Members of the group have experience in developing communication training curricula and facilitating interprofessional communication training. This session aimed to identify key areas of focus and best practices leveraging existing communication guidelines/curricula such as VitalTalk, which were then documented and categorized into relevant themes. 15 Themes derived from this session were converted to the four steps of the framework, with a draft document outlining the approach, rationale, and exemplar language for each step. Initial drafts were circulated among team members, incorporating multiple rounds of feedback to refine the guidelines. A structured decision-making process was employed to resolve any disagreements, ensuring alignment and consensus. Once the team reached a final version, the framework underwent external review by clinicians from diverse specialties including ICU physicians, nurses, allied health professionals such as a chaplain and social worker not involved in the initial development process. Their feedback on feasibility, clarity, and applicability informed final refinements, resulting in a rigorously vetted, consensus-driven framework.
Framework for Cultivating Prognostic Awareness for Time-Critical Decisions
The framework outlines four steps to navigate conversations to rapidly cultivate prognostic awareness and make time-critical decisions. Key steps are to (1) clearly name the problem and urgent decision to be made, (2) delineate possible treatment options and explore preferences for escalation or nonescalation of care, (3) provide recommendations, and (4) check in to clarify understanding and agreement with the recommendation (Fig. 1, Table 1).
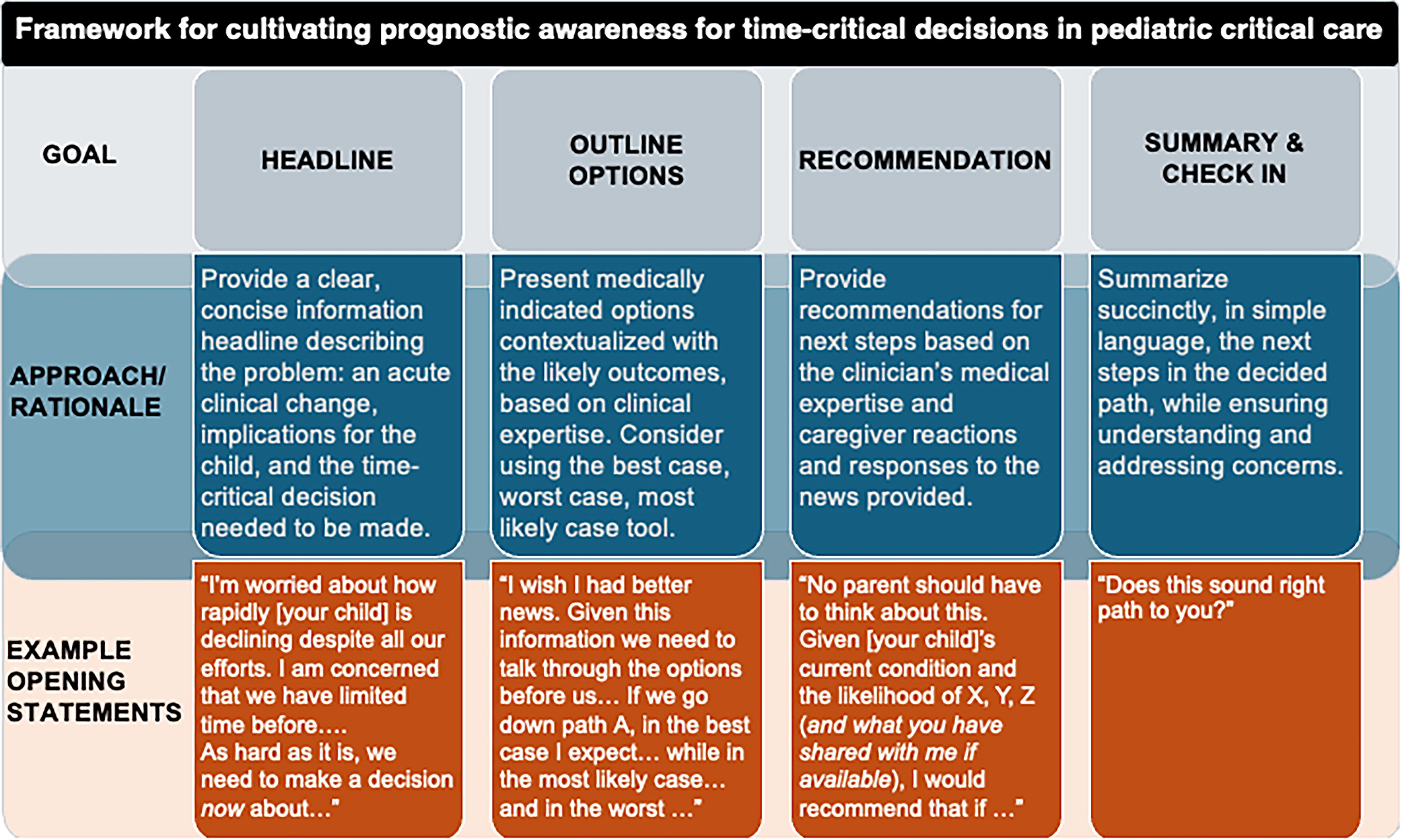
Framework for cultivating prognostic awareness for time-critical decisions in pediatric critical care. A summary of the approach/rationale and example opening statements of the four steps of the proposed framework.
Framework Implementation Phrasing Across Distinct Scenarios Encountered in Acute Illness
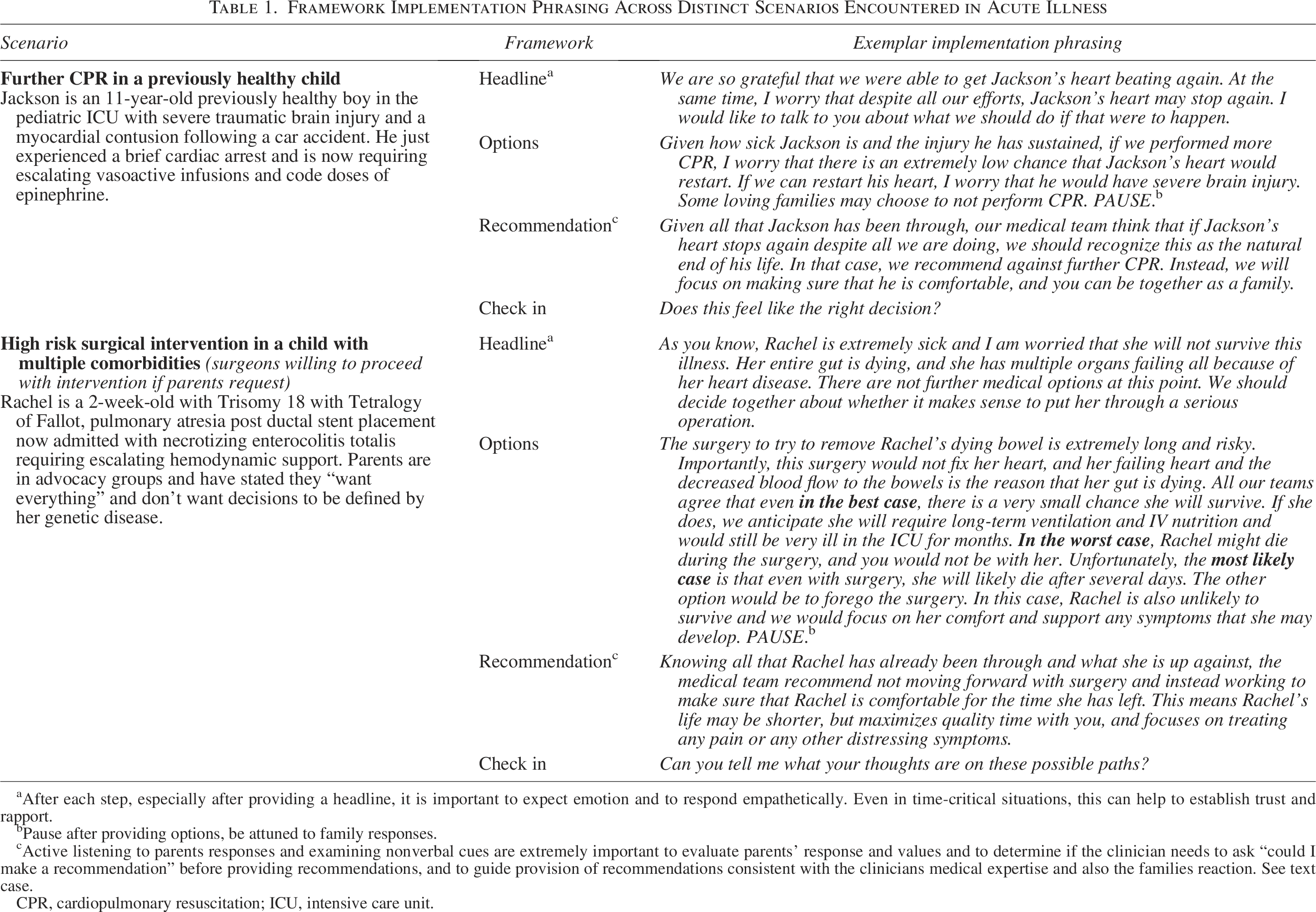
After each step, especially after providing a headline, it is important to expect emotion and to respond empathetically. Even in time-critical situations, this can help to establish trust and rapport.
Pause after providing options, be attuned to family responses.
Active listening to parents responses and examining nonverbal cues are extremely important to evaluate parents’ response and values and to determine if the clinician needs to ask “could I make a recommendation” before providing recommendations, and to guide provision of recommendations consistent with the clinicians medical expertise and also the families reaction. See text case.
CPR, cardiopulmonary resuscitation; ICU, intensive care unit.
In time-critical circumstances requiring an imminent decision, we recommend starting with a concise “news headline” that explicitly summarizes the child’s prognosis and provides context for urgent decision making. This is followed by an outline of the medically appropriate options, tailored to the child’s specific clinical context and family needs. The clinical team should determine, based on their expertise, what therapies/interventions may confer clinical benefit or therapeutic efficacy. These options are then presented along with their likely outcomes for the child. Existing tools such as the best-case, worst-case, and most-likely case scenarios can help contextualize the implications of each option for the child.15–17 When engaging in discussion around the options, the clinician should be attuned to both verbal and nonverbal cues from the patient or parents/caregivers and pause allowing and responding to emotion. Next, incorporating responses from the family where available, recommendations for next steps are provided based on the medical teams’ expertise, ensuring alignment through a check-in on the decision.
There can be a range of potential responses or reactions to these conversations. Therefore, it is essential to incorporate high-quality communication principles, such as those presented in VitalTalk (Table 2).15,17,18 Given differences in communication strategies required for conveying time-critical prognostic information for parents/caregivers of previously healthy children compared with those with underlying chronic conditions, we provide distinct exemplar responses for these populations (Table 1).8,19
Universal Communication Skills to Incorporate in All Conversations in Acute Illness
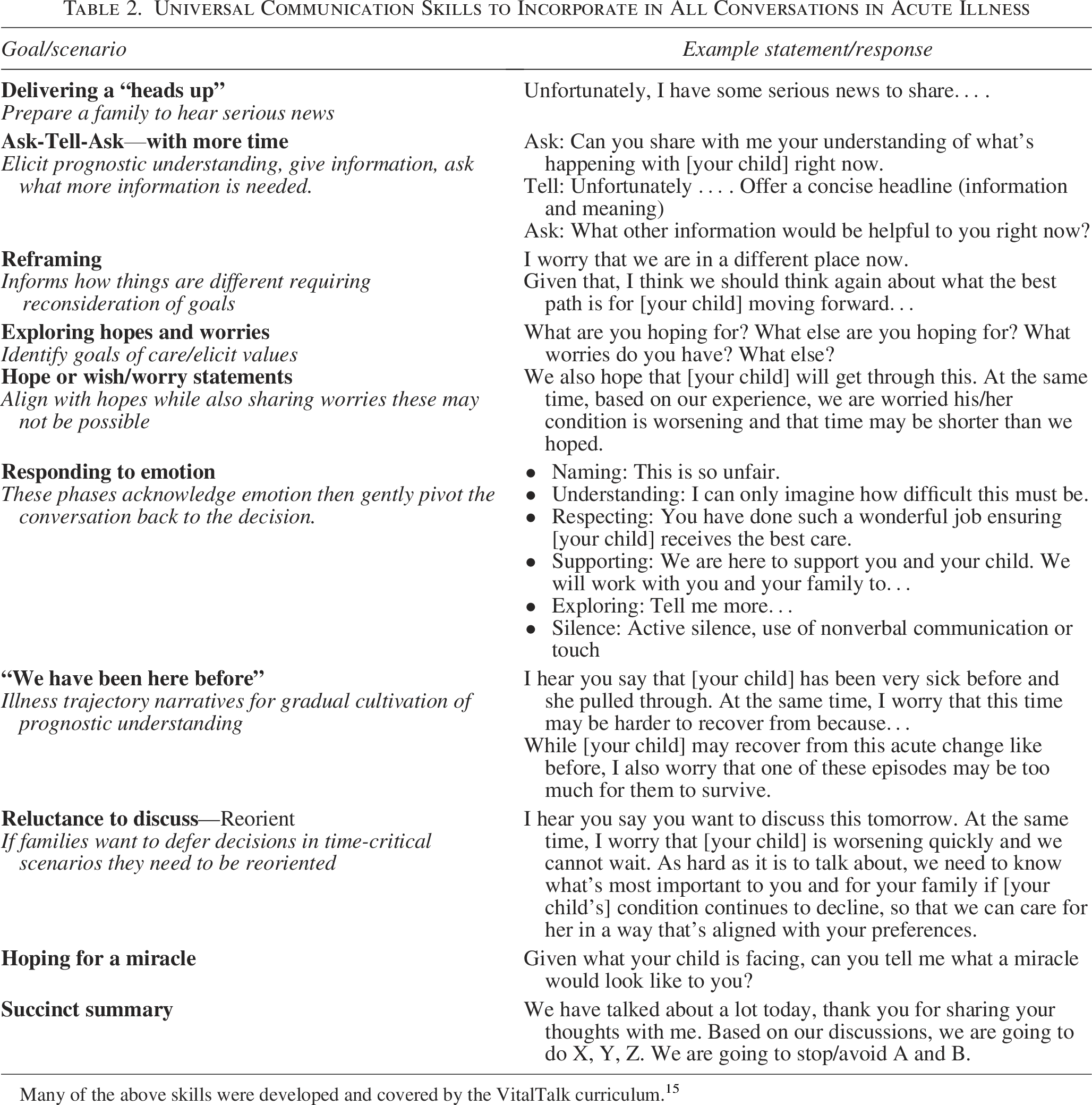
Many of the above skills were developed and covered by the VitalTalk curriculum. 15
This approach is specifically designed for use in time-critical settings. It is the responsibility of the medical team to discern whether the situation at hand necessitates an immediate decision, limiting the opportunity for a deeper exploration of values. In cases involving medical complexity where prior discussions or decisions have taken place, clinicians can draw on that knowledge and cues from the parents/caregivers to inform the current conversation. If the situation allows for a less urgent decision, clinicians should employ previously established approaches to eliciting and incorporating family values. 18
Applying the Framework Incorporating Different Parent/Caregiver Responses
The ICU clinician first offers a “headline,” a concise statement that indicates both the severity of the situation and urgency of the decision: Jose is on the maximum amount of breathing support that we can provide. Despite this, he is worsening and has evidence of bleeding in his brain. We need to decide together now about whether to proceed with an emergent operation.
Next, the clinician offers options: Unfortunately, the surgery will almost certainly worsen his brain damage and there is a high chance Jose won’t survive the operation. On the other hand, without an operation, Jose will not survive. Some families might opt to not move forward with surgery or any further invasive procedures and instead choose to focus on Jose’s comfort. Then pauses to see how the parents respond and read their body language.
Response 1: Jose’s parents are distraught. He is their first baby, and they never considered this may happen. The brain bleed is a grade 3 ICH. The clinician responds to their emotion and incorporates family cues and the clinical information and respond by acknowledging how impossible this situation is. I can only imagine how difficult this must be. Based on everything we know, our medical team recommends proceeding with the surgery, as it offers him a small but likely only chance of survival. In the next few days, we will learn more about his chances of improvement and any neurological effects. We can regroup then to discuss next steps.
Response 2: The parents share that they had thought hard about what decisions they would make if Jose’s heart condition was on the severe end of the spectrum. With three typically developing children at home, they decided they would only pursue interventions if it allowed Jose to grow and develop with the hope that Jose would be able to run on the playground like his siblings. Furthermore, the ICH is classed as the most severe, a grade 4 hemorrhage. The clinician incorporates this clinical information and the cues from the family and respond with empathy. I really wish we weren’t here. In thinking about these options, the likely outcomes of surgery, and what you have shared, the medical team would recommend against proceeding with an invasive surgery and instead focusing on keeping Jose comfortable and allow you to be with him… .
In both scenarios, follow up with a check-in: Does this feel like the right decision for you and Jose?
Commentary
Shared decision making involves a collaborative partnership between clinicians, patients, and parents/caregivers, existing on a spectrum with varying influence from all parties on decision making.20,21 Transparent, high-quality communication provides essential context while incorporating medical expertise. Even in time-critical circumstances, eliciting family values may be feasible and alter recommendations of the medical team. In certain situations, highly directive recommendations from medical teams are both ethically supported and necessary. 21 An observational study analyzing parents/caregivers’ decision-making preferences found that factors such as urgency, perceived need for medical expertise, prognostic certainty, and expected benefits were associated with a preference for greater medical team decision-making influence. 22 Surveys of bereaved parents also highlight the importance of clinician recommendations, with parents/caregivers valuing transparency and preparation.23,24 However, parents/caregivers may make a decision that differs from the clinicians’ recommendation, making it crucial to reassure them that they will be fully supported, regardless of their choice.
Decision making around invasive interventions such as cardiopulmonary resuscitation (CPR) in patients with critical illness is particularly challenging for both parents and clinicians. Among children with heart disease, receiving CPR was the only medical factor associated with a parental perception of a negative death experience. 23 Without clinical context or a clear recommendation about CPR or other invasive interventions, parents/caregivers may interpret the offer as a sign that it will be both effective and without significant downsides. Collectively, findings suggest that clinicians should have greater confidence in providing recommendations regarding whether or not to pursue therapies that may not be beneficial to the patient.22,23,25,26 In offering such recommendations, clinicians must ensure parents/caregivers do not feel isolated or abandoned, and should therefore discuss what will be done for the child, such as ensuring comfort and allowing time together, before addressing what will not be done, such as CPR. Cultural and religious perspectives also shape decision making and in some cases, parents/caregivers rely on and expect clear, directive medical recommendations.21,25 In other cases, particularly if trust has been compromised or unfair treatment perceived, parents/caregivers may be less receptive to a directive communication strategy. Structural inequities, historical mistreatment of underrepresented populations in health care, and the current media climate may lead to mistrust and underscore the need for honest, transparent discussions about the benefits, burdens, and likely outcomes of interventions.27,28
Children with medical complexity represent a substantial proportion of ICU decedents. 29 Many have experienced multiple “near-fatal” clinical deteriorations, which should prompt advance care planning. However, despite growing evidence that preemptive conversations and serious illness communication guides improve parent experience and EOL outcomes, these opportunities are often missed.12,24,30,31 Families whose children previously survived intensive resuscitative measures may reasonably question why this situation is different, and clinicians need a strategy to address these concerns. Notably, the number of prior ICU admissions correlated with greater parental preference for medical team guidance on decision making.22,32 However, complexity should not deter clinicians from their duty to provide their professional perspective and make clear recommendations, while also respecting parents’ deep understanding of their child.25,26
Medical complexity, as exemplified by Trisomy 18 in our case (Table 1), encompasses a wide range of conditions with challenges interpreting outcome data stemming from practice variation, different risk profiles from available interventions, which are often offered to healthier children, and negative publication bias. 33 These areas of substantial controversy highlight the intersections of parental values, clinical judgments, ethics, and the influence of social media publicity or public opinions. 34 These concerns may be further magnified when parents/caregivers are faced with time-critical decisions. When caregivers express a desire to “do everything,” it is essential to explore what that means to them.35–38 Emerging data suggest benefits of personalizing communication as part of family-centered care where therapeutic options are reviewed; and each patient receives a fair, individualized assessment, and value-aligned decision making. 4
This proposed framework is not intended to replace existing guidelines for eliciting values and making medical recommendations; rather it applies key principles to support decision making in time-critical situations. 10
Conclusion
Time-critical situations require precise nuanced communication to rapidly convey and contextualize an acute change in clinical trajectory that requires an urgent decision. We suggest a structured approach that begins with a clear headline statement naming the problem and urgent decision required. This is followed by an outline of medically appropriate options, tailored to the child’s specific clinical context. Finally, clinicians should offer a recommendation incorporating cues from the patient or parent/caregiver, where available, and check in to ensure alignment on the decision and next steps.
Footnotes
Acknowledgments
Chelsea Cotnoir, Meena Laronde, Melissa Vela.
Author Disclosure Statement
The authors have no conflicts of interest to disclose.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.