
Abstract
Systemic autoimmune rheumatic diseases (SARDs) consist of a broad range of immune-mediated multisystem diseases. They are chronic, incurable illnesses that often present in early to mid-life and can be associated with a high symptom burden, disability, and early mortality. Treatment guidelines for similar chronic, life-limiting conditions with uncertain disease courses now recommend palliative care (PC) assessment at the time of diagnosis. Recently, the first rheumatology treatment guidelines to recommend PC were also published. Integration of PC into rheumatology offers an opportunity to improve quality of life and deliver better goal-concordant care for people with severe rheumatic disease. This article provides 10 tips to guide PC clinicians when caring for people with rheumatic diseases.
Keywords
Introduction
Systemic autoimmune rheumatic diseases (SARDs) consist of a broad range of autoimmune diseases (Table 1). SARDs are incurable, lifelong, multisystem diseases, with diagnosis commonly occurring in early to mid-life. High symptom burden and associated functional disability are notable from disease onset,1–4 and some SARDs are also associated with high mortality.5–9
Examples of Autoimmune Diseases Based on Disease Class

irAE, immune-related adverse event; ANCA, anti-neutrophil cytoplasmic autoantibody.
Historically, the management of SARDs has focused on disease modification rather than individual symptom management. Treatment guidelines for similar chronic, life-limiting conditions with uncertain courses now recommend palliative care (PC) assessment at the time of diagnosis,10,11 and recently the first rheumatology guidelines to discuss the role of PC in systemic sclerosis (SSc) were published. 12 These rheumatology guidelines describe PC as an area for “development and engagement” and recommend PC involvement in cases of SSc with high symptom burden and those nearing end of life. 12 While little research is available on PC in rheumatology, data from other fields have demonstrated that targeted symptom assessment and management provided through PC and in parallel with disease-modifying treatment can improve patients’ and caregivers’ quality of life, reduce health care costs, and potentially improve survival.13–19 Integration of PC into rheumatic disease management offers an opportunity to similarly improve the lives of people with SARDs.
Tip 1: While People with SARDs May Live for Years, They Can Suffer from High Symptom Burden and Disability from Disease Onset; Management of Symptom Comorbidities Requires a Combination of Pharmacologic and Nonpharmacologic Interventions
People with SARDs have significant healthcare utilization and require lifelong specialist management, monitoring of treatment side effects, and management of disease-specific and treatment-related comorbidities. SARDs are commonly associated with significant fatigue, cognitive symptoms that include headache, brain fog, memory loss, low mood, anxiety, breathlessness, gastrointestinal symptoms, and sleep disturbance.2,20–22 Poorly controlled symptoms have a major impact on patients’ quality of life,2,23–26 and in some SARDs, unfortunately, disease-modifying therapy is not associated with significant improvement in symptom burden and quality of life. 20
Management of symptoms is often complex, owing to the multifactorial causes of pain, fatigue, and breathlessness. Symptom management is best performed together with patients’ rheumatologists as disease-specific therapy may offer major symptom benefit in addition to standard PC treatments. Common symptoms seen in SARDs are shown in Table 2 with recommended management options.
Useful Pharmacologic and Nonpharmacologic Interventions for Common Symptoms Seen in Systemic Autoimmune Rheumatic Diseases
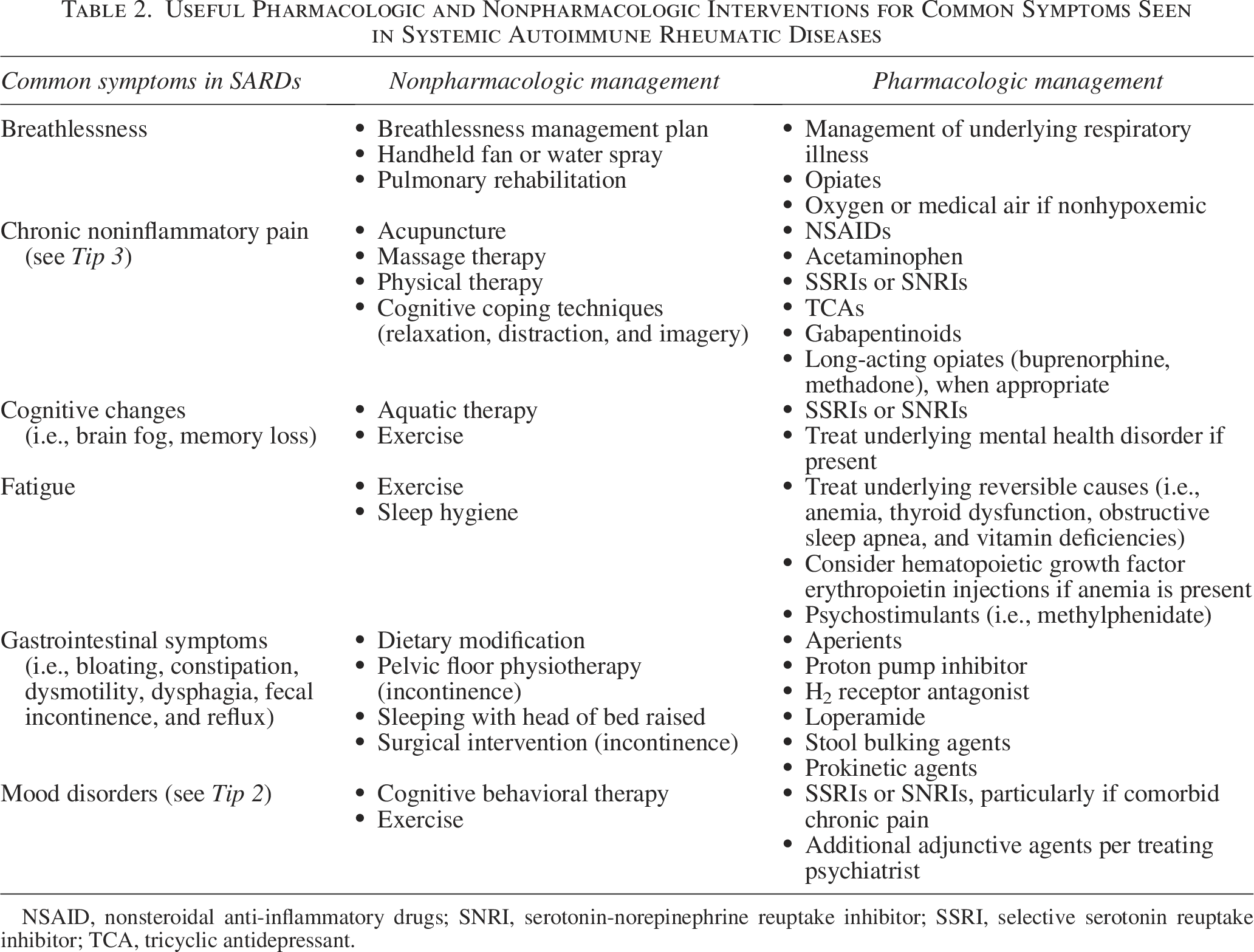
NSAID, nonsteroidal anti-inflammatory drugs; SNRI, serotonin-norepinephrine reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor; TCA, tricyclic antidepressant.
Tip 2: Pain Is the Most Common Symptom That People with SARDs Experience, Though the Etiology of Pain Is Complex; Close Collaboration with Rheumatology Teams Is Needed to Institute Both Disease-Modifying Treatments and Palliative Treatments
People with SARDs often have heterogeneous pain symptoms that are a combination of nociceptive, neuropathic, and nociplastic pain.27,28 Careful history-taking and physical exam are critical in determining appropriate pharmacologic interventions.
When evaluating pain, it is helpful to think about Type 1 versus Type 2 symptoms as characterized in people with systemic lupus erythematosus (SLE) (Table 3). 29 Type 1 refers to internal organ involvement often driven by clear immune mechanisms, such as inflammatory arthritis, oral ulcers, or serositis. Type 2 symptoms refer to those with less clear pathogenesis that are often not responsive to immunosuppressive medications, such as fatigue, depression, cognitive dysfunction, and widespread pain. 30
A Model to Classify Inflammatory and Noninflammatory Symptoms Experienced by People with SLE
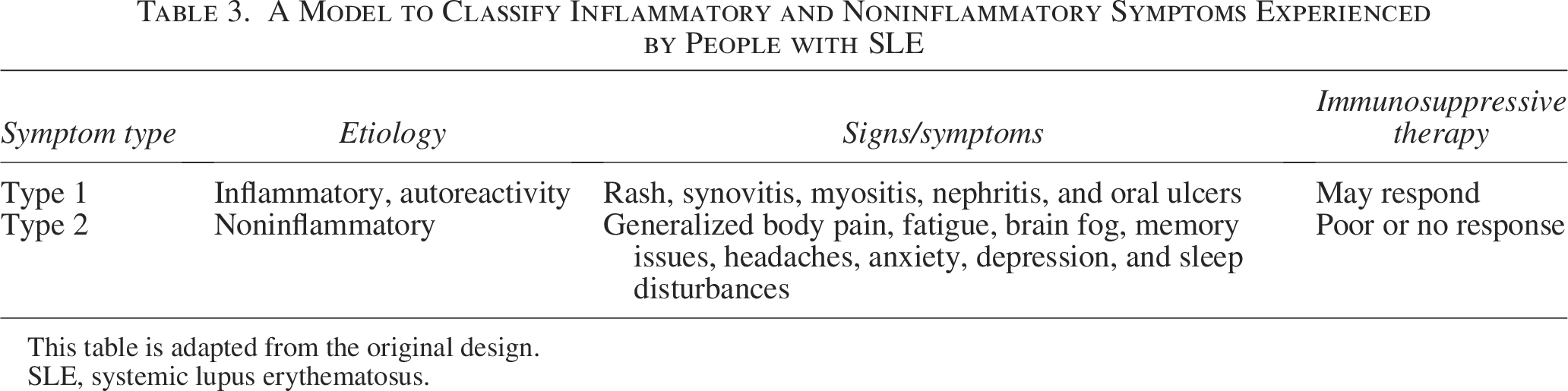
This table is adapted from the original design.
SLE, systemic lupus erythematosus.
Both symptom types can coexist with varying severity, though Type 2 symptoms often occur independent of acute flares. This model of symptom characterization may also be beneficial when evaluating pain symptoms in people with non-SLE SARDs. Clinicians should consider adjuncts such as topical creams and patches, gabapentinoids, selective serotonin reuptake inhibitors (SSRIs), and serotonin-norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), and muscle relaxants. Opioids may be used to help manage pain, but it is important to note that opioids in SSc can be associated with worsening gastrointestinal dysmotility and lead to severe constipation or pseudo-obstruction.31,32 Hand pain from ischemic digital ulcers may be best managed by a combination of treatments that includes vasodilatory agents such as phosphodiesterase-5 inhibitors and antibiotics in combination with analgesics.
People with SARDs can have complicated disease trajectories and significant symptom burden, and they often suffer from suboptimal pain management. Care for these patients requires specific knowledge and expertise of the underlying condition, understanding of the etiologies of pain and its relation to inflammation, and treatment modalities. Thus, symptom management strategies are best implemented in collaboration with rheumatology teams to balance the need for disease-modifying agents in combination with palliative agents to derive the most symptomatic benefit for patients.
Tip 3: People with SARDs Suffer from High Rates of Mental Health Disorders; It Is Important to Consider Early Utilization of Psychiatry, Psychotherapy, and Pharmacotherapy to Improve Quality of Life
Studies demonstrate that a high prevalence of mental health disorders, such as depression and anxiety, are present in people with SARDs, and these disorders are often undertreated. 33 Recognizing the presence of mental health comorbidities is critical for addressing rheumatic disease and improving clinical outcomes. For example, a study in pediatric SLE demonstrated psychotropic medication use or psychotherapy was associated with improved adherence to hydroxychloroquine therapy. 34 Anxiety and depression are major independent predictors of fatigue, and thus important to address in holistic care of these patients. 35
Aside from mental health disorders, people with SARDs often suffer from additional “invisible” symptoms that can be equally and sometimes more debilitating, such as fatigue, cognitive dysfunction or brain fog, and noninflammatory chronic pain syndromes like fibromyalgia. These manifestations are common in some SARDs such as SLE; for example, up to 80% of those with SLE have fatigue. 36
The Type 1 and Type 2 model of SLE referenced in Tip 2 (Table 3) is helpful when approaching these “invisible” symptoms. Recognition of non-inflammatory comorbidities, including fibromyalgia, depression, and anxiety in SARDs, is critical, given these symptoms do not typically respond to immunosuppressive medication and contribute to significant disability and reduced quality of life. Recognizing these manifestations can help ensure targeted, nonpharmacologic interventions are used and prevent overprescribing immunosuppressive medications for noninflammatory symptoms. Interdisciplinary models involving PC, social work, psychotherapy, and cognitive behavioral therapy can be helpful to better address this symptom constellation.
Tip 4: There Is a High Caregiver Burden Associated with Management of SARDs That Is Frequently Overlooked; Incorporating Caregiver Assessments into Palliative Visits Is Needed
Caregiver burden is a well-documented challenge for those caring for people with major health issues such as cancer, dementia, and heart or renal failure.37–39 Similarly, caregiver demands in SARDs can cause burdens that are frequently overlooked. Caregivers for people with SARDs dedicate significant time each week to caregiving; this ranges from 7 hours or more per week in rheumatoid arthritis (RA) 40 to 16 hours or more per week in SLE. 41 Caregivers experience disruption to their daily lives, including work disruptions, economic challenges, and emotional strain, and higher psychological distress in patients has been shown to correspond with higher caregiver burden.42–45 Unique challenges include legitimizing disease to others for caregivers of people with fibromyalgia 46 and change in family relationships for caregivers of people with juvenile idiopathic arthritis. 44
Incorporating caregiver assessments, such as the Zarit Burden Interview (ZBI), 47 which has specifically been utilized in caregivers for people with SARDs,43,45 into visits allows clinicians to better address these challenges, providing support that can alleviate some of the burdens. 48 The ZBI 4-item screening version has been shown to correlate well with the full version 49 and can be implemented efficiently in clinical practice to identify high caregiver burden. Studies in other disciplines have shown that interventions, especially those involving psychoemotional support, have positive effects on caregiver well-being. 50 These approaches are crucial for improving both patient and caregiver outcomes in SARDs.
Tip 5: Trajectories of SARDs Can Be Highly Variable Depending on the Diagnosis, Patient Factors, and Treatment Factors and Tend to Most Closely Resemble the “Organ Failure” Trajectory: Longitudinal Slow Decline with Intermittent, Serious Episodes
Most people with SARDs tend to have a relapsing and remitting course, with periods of disease quiescence alternating with episodes of increased disease activity, commonly called a “flare.” Disease flares are associated with worsening symptoms such as increased pain and may also present with new or progressive organ dysfunction. The timing and severity of flares can be unpredictable; some can be managed on an outpatient basis with temporary adjustments to oral medications, while some flares are severe enough to result in hospitalization or even critical illness. This course tends to closely resemble the organ failure trajectory model. 51
An unpredictable disease trajectory is one aspect of illness-related uncertainty for people with SARDs. Prior studies have revealed additional themes of illness uncertainty, including symptoms, medical management, self-management, and social functioning. A recent study demonstrated that among people with SARDs, those with greater uncertainty tended to have worse mental health outcomes, including greater anxiety, depression, and greater perceived impact of illness. 52 Notably, this study also showed that people with SARDs expressed strong interest in interventions to address mental health needs, particularly those with greater illness-related uncertainty.
Clinicians caring for people with SARDs, whose diseases are rare and difficult to study, face uncertainty in terms of diagnosis and management decisions.53–55 Furthermore, uncertain disease trajectories make prognostication challenging; this in turn increases the difficulty for rheumatologists in determining appropriate triggers for referral to PC. Importantly, even in the face of prognostic uncertainty, rheumatologists caring for people with SARDs can partner with PC teams who can take an active role in framing prognostic discussions and supporting those experiencing distress due to illness-related uncertainty. Collaboration between rheumatology and PC teams is needed to determine individualized and population-wide approaches for PC referral.
Tip 6: Acute Organ Decompensations from the Underlying SARD Can Lead to Recurrent Hospitalization and Mortality; Engaging Rheumatology Teams, Who Often Have Known the Patient for Years, Can Be Helpful in Maintaining Effective Therapeutic Relationships in the Acute Setting
As is true with other serious chronic diseases, people with serious SARDs may have a meaningful longitudinal relationship with the specialist managing their condition. While there are few studies looking specifically at communication preferences in people with SARDs, studies in other disease states show that people value the relationship they have with their outpatient subspecialty team and report increased trust in a care plan when a trusted clinician is involved. 56 When people with SARDs are reaching the final stages of their disease, prognostic information and end-of-life planning may be better received or more readily accepted when their primary rheumatologist is part of the conversation. 57
Particularly in the acute setting, PC clinicians should involve the primary rheumatologist whenever possible to gain insight into the clinical and prognostic implications of the SARD and to gain knowledge about the patient’s social support, coping strategies, and any communication that has already taken place about preferences for treatment or goals of care. If breaking bad news is anticipated, PC clinicians should include the primary rheumatologist. Even if there are no active rheumatologic issues, input from trusted members of the rheumatology team may assist in developing and maintaining therapeutic relationships.
Tip 7: Pulmonary Involvement Is Seen Across Many SARDs and Contributes to High Symptom Burden and Increased Mortality; Attention to Breathlessness Is Particularly Important as This Symptom Is Often Underrecognized and Undertreated
Connective tissue disease-associated interstitial lung disease (CTD-ILD) accounts for ∼25% of all cases of interstitial lung disease (ILD). 26 Any SARD can be associated with ILD, with varied incidences between different SARDs: SSc (65%), mixed connective tissue disease (52–67%), idiopathic inflammatory myopathy (36–45%), Sjögren’s syndrome (11–27%), RA (5%), and SLE (1–2%).26,58
In general, the prognosis of CTD-ILD is more favorable than idiopathic pulmonary fibrosis (IPF), though disease severity can vary according to the underlying SARD, radiographical imaging pattern, autoantibody status, and other prognostic factors. For example, people with seropositive (positive antirheumatoid factor and anticyclic citrullinated protein) RA often present with usual interstitial pneumonia, which progresses at a similar rate as that seen in IPF, whereas people with SSc and idiopathic inflammatory myopathies often present with nonspecific interstitial pneumonia, which can be more responsive to immunosuppressive therapy or more slowly progressive. 58 Regardless of these factors, the most consistent predictor of poor prognosis among all CTD-ILDs is significant and progressive impairment in pulmonary physiology as measured by the forced vital capacity. 58
Cough and breathlessness can significantly impair patients’ quality of life, and CTD-ILD has been associated with worse quality of life than IPF due to increased dyspnea and the concurrent experience of joint pain, stiffness, and other manifestations of the underlying SARD. 59 Unfortunately, most immunosuppressive and antifibrotic therapies have not been shown to improve cough or breathlessness, and rheumatologists are not trained to provide supportive therapies for these symptoms, leaving people with CTD-ILD vulnerable to significant impairment in their quality of life. 26 PC clinicians are uniquely trained in pharmacologic and nonpharmacologic interventions for these symptoms, such as careful opiate titration, medical air, handheld fans, and breathlessness crisis management plans, which may be invaluable to people suffering from late-stage effects of CTD-ILD. 60
Tip 8: Despite Advancements in Rheumatic Disease Therapy, Early Mortality Remains High, Particularly for Diseases Such as SSc and SLE; Advance Care Planning Is a Critical Tool for Helping People with SARDs Prepare for the Future
On average, SSc and SLE each account for more than 20 years of life lost for people living with these diseases.5,6 Chronically, SSc results in the highest burden of morbidity and mortality with a mortality rate four to five times the general population. 5 Mortality is higher for people with diffuse compared to limited SSc.5,61 The distinction between diffuse and limited disease is made by the extent of skin thickening, with diffuse disease defined by the presence of skin thickening proximal to the elbows or the knees. End-stage organ failure in SSc can manifest as respiratory failure from ILD or pulmonary arterial hypertension, gastrointestinal failure from dysphagia or intestinal dysmotility, and renal failure from SSc renal crisis.
Similarly, SLE results in mortality rates two to three times the general population. 6 People with juvenile-onset SLE fare worst, and SLE ranks in top 5 causes of death for Black and Hispanic people aged 15–24 years. 7 Lupus nephritis is a significant contributor to mortality in people with SLE; up to one in five people with SLE will develop end-stage renal disease within 10 years of lupus nephritis diagnosis, and when present, mortality rises to five to eight times the general population.62,63 Additional SARDs that are associated with increased mortality include vasculitis 8 and classes of idiopathic inflammatory myopathies such as inclusion body myositis 9 and anti-melanoma differentiation-associated gene 5 (MDA5) dermatomyositis. 64
Given the disparate mortality rates seen in SARDs, timely Advance Care Planning (ACP) and serious illness communication are critically important to help people prepare for the future and ensure delivery of goal-concordant care when they do become ill. ACP should involve discussion of possible disease evolution to end-stage organ failure and the accompanied uncertainty in disease course (see Tip 5) and include trusted outpatient clinicians (see Tip 6); when appropriate, discussion should explore patients’ preferences toward organ transplantation.
Tip 9: People with SARDs Die from Direct Complications of Their Rheumatic Disease and from the Same Causes as Everyone Else at Higher Rates; This Mortality Risk Is Important to Incorporate into Discussions About ACP and Prognostication for People with SARDs
People with SARDs experience higher rates of common causes of death such as cardiovascular disease, 65 infection,6,66 and malignancy, 66 which contribute to the increased morbidity and mortality seen in this population. This disparate risk is thought in part to be due to disease-specific risk factors such as glucocorticoid use, immunosuppressive disease-modifying treatments (i.e., methotrexate, cyclophosphamide), and inflammation from the rheumatic disease itself. 67 These disease-specific risk factors are important to consider when framing ACP discussion about comorbidity risk and mortality. It is also important to recognize that younger people with disease, women, and Black, Asian, and Hispanic patients experience an even more pronounced risk.68,69 For example, a woman less than age 40 with SLE has a 50-fold increased risk of having cardiovascular disease compared to women of the same age without SLE. 70
When considering the risk of malignancy in SARDs, there are factors to consider that can help frame a person’s risk of developing malignancy. For example, ILD (see Tip 7) increases the risk of lung cancer development, particularly in people who smoke.71,72 People with RA and Sjögren’s syndrome have a 2- and 5-fold higher risk of developing non-Hodgkin’s lymphoma, respectively.73,74 The risk for lymphoma is related to years of increased B cell and T cell activation, more frequently seen in people with difficult to control disease. 74 SARDs may also present as a paraneoplastic disease, such as in dermatomyositis and people with SSc who have a positive anti-RNA polymerase III antibody.75,76 Rheumatic disease symptoms from paraneoplastic SARDs often improve with treatment of malignancy; however, for treatment refractory malignancies, collaboration of rheumatologists and PC experts may prove valuable to optimally control patient symptoms and improve the quality of life.
People with SARDs and comorbid malignancy often require nuanced discussions about the most optimal treatment approach to ensure it is concordant with the patient’s goals of care. Some disease-modifying antirheumatic medications may not be compatible with lymphoma treatments, and PC evaluation and management can result in enhanced symptomatic control for people with SARDs and lymphoma. Additionally, immune checkpoint inhibitor therapies used to treat some malignancies pose an increased risk of flaring any underlying autoimmune disease, which can hasten death if a patient develops rapid onset end-organ failure such as respiratory failure in patients with underlying ILD. 77 ACP discussion prior to initiating potentially life-threatening treatment is paramount, and early integration of PC into the treatment team may be particularly helpful for these patients.
Tip 10: Current Rates of ACP and PC Referrals Are Low for People with SARDs; Interdisciplinary Efforts to Integrate PC Principles into Rheumatic Disease Care and PC Specialists into Rheumatology Clinics Are Obvious Ways to Improve the Quality of Life for People with SARDs and Their Caregivers
In a study examining nearly 160 people with SARDs during their last year of life, 15% of people were referred to PC and only 3% of people had documentation of ACP. The median time between PC referral and death was just 8 days. 78 Encouragingly, there has been work demonstrating an increase in inpatient PC referrals in people with SLE over an almost 10-year period from 0.1% to 1.2% 79 ; nonetheless, these rates remain exceedingly low. It is critical to acknowledge that certain people with SARDs have inequitable access to PC. People with lower income, those insured by Medicare, and those of Hispanic ethnicity had lower rates of PC consultations. 79
Integration of specialist PC clinicians into rheumatology clinics offers hope of improved symptom management, quality of life, and ACP for people with serious SARDs. 20 This benefit has been demonstrated in studies evaluating interdisciplinary clinic models for people with other serious chronic illnesses. For example, comanagement of ILD with pulmonary and PC specialists in the outpatient setting has been shown to improve both symptom management and ACP documentation; as discussed in Tip 7, ILD is a common form of organ involvement in SARDs with significant suffering, providing further strength to the recommendation for integration of PC into rheumatology. 80
While comanagement can increase access to specialist PC for people with serious SARDs, it is also necessary to investigate ways to improve primary PC skills by the rheumatologist for all people with SARDs. Collaboration between rheumatology and PC, such as through fellowship training initiatives, grand round presentations, and clinician workshops, is needed. PC specialists will be essential in implementing these needed educational initiatives. Topics should include basic symptom assessment and management, caregiver assessment, and ACP discussion skills. By incorporating PC principles into rheumatology practice, more people can benefit from these tenets while minimizing the burden on both inpatient and outpatient PC specialists.
Conclusion
SARDs consist of a wide range of chronic, incurable, multisystem autoimmune diseases. People with SARDs can suffer from a high symptom burden, disability with reduced quality of life, and early mortality. SARDs are accompanied by significant disease uncertainty, including prognostic uncertainty, which challenges the appropriate timing of ACP and referral to specialist PC. PC clinicians offer a unique set of skills to improve the care for people with serious SARDs, and further collaboration between PC and rheumatology is needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.