
Abstract
Suicide by patients can cause significant distress for the palliative care team. This includes feelings of guilt and self-blame which affect both staff morale and mental well-being, which if left unaddressed, can eventually lead to burnout. We report the case of a patient suicide and how our organization implemented a framework to guide and support staff through this process. The HEAL framework comprises 4 components: honoring the loss of the patient, encouraging self-care and organizational support, affirming the individual and team’s sense of meaning and purpose, and learning lessons from the patient’s suicide.
Introduction
Patient suicides are not uncommon in palliative care settings. Previous studies showed a prevalence of around 0.03% of patients in the British and Italian populations.1–2 Oncology patients have a similar suicide rate of 0.01%, people with stomach and pancreatic cancer having the highest risk. 3 Suicide in people with Chronic Obstructive Pulmonary Disease had a suicide rate ranges from 0.05% to 2.5% in various studies,4–5 with men having a higher suicide lethality compared with women (13.9% vs. 4.1%). 5
The impact of a patient’s suicide is often felt profoundly by the palliative care team. 6 Fairman, in a study of hospice clinical staff who experienced patient suicides, revealed that those involved in the deceased patient’s care often felt a sense of guilt and self-blame. They also reported a change in their professional attitude—respecting the suicide as an act of patient autonomy, accepting their own limits, and acknowledging that they cannot control every outcome. The experience also helped them to mature in their clinical practice, helping them become more sensitive to the cues of patients. Palliative care providers exhibit varying means of responding to the trauma of suicide. They described the use of team-based support strategies, debriefings, and personal spiritual practices as useful. They also recommended that future support include facilitated debriefings, individual counseling, spiritual practices, leaves of absence, self-care activities, and educational interventions. However, there is a need for greater support for staff, as the literature shows that organizational responses typically focus on lessons learned and future prevention rather than clinician support. 7
We present the case of the suicide of a patient with end-stage lung disease and describe support strategies to mitigate the traumatic impact of suicide on our palliative care team. We will share the use of a framework in helping palliative care teams to navigate patient suicides.
Case Description
Mr. T was a 70-year-old retired taxi driver with severe bronchiectasis and chronic dyspnea who was attending hospice daycare and undergoing pulmonary rehabilitation. He was married and lived together with his wife and daughter and enjoyed singing karaoke with his friends. He had multiple hospital admissions for infective exacerbations and was on a low-dose Fentanyl patch and oral morphine for breakthrough episodes of dyspnea.
He had complained of dyspnea with a modified Borg Scale of 1–2 (very slight to slight) at rest, which worsened to 6 (severe) on prolonged exertion but would revert to baseline scores after a few minutes of rest. He usually required one breakthrough dose of morphine before showering.
His condition was initially stable, and he improved functionally with rehabilitation for the first two months. However, he started deteriorating in the third month, with worsening dyspnea and exercise tolerance. He also reported escalating anxiety and panic attacks. He was started on alprazolam as needed for his anxiety. He was taught breathing and relaxation exercises by the physiotherapist and also supported emotionally by the social worker. He subsequently admitted to feeling depressed and thought about ending his life by jumping off his high-rise apartment. However, he was held back from the thought for fear of leaving his wife alone.
The multidisciplinary team provided further supportive measures, with the nurses and social worker checking in on him more frequently. We also informed his wife and daughter about his suicidal thoughts, and they became more vigilant in “watching out” for him. A palliative care physician titrated his opioid regimen to manage his dyspnea. He was also started on fluoxetine and maintained on alprazolam for his panic attacks. The team also arranged for supplemental oxygen, which he felt did little to reduce his chronic dyspnea.
Mr. T eventually died by suicide by jumping off his apartment the subsequent week.
His wife informed the palliative care team that morning. The team immediately provided support to his wife and daughter on the same day, and our social worker provided post-bereavement support and counseling for his wife for the immediate period and the subsequent few months thereafter until she had recovered substantially and was able to function in the community.
The clinician leaders recognized the need for staff support in this situation and proceeded to use the HEAL approach to care for staff who were directly involved in caring for Mr. T.
Discussion
When a patient dies by suicide, the entire palliative care team can be deeply affected as one’s personal and professional values and worldviews are challenged and “assaulted.” This trauma can be emotionally overwhelming, particularly given that, on the fundamental level, a patient’s suicide is a direct affront to the very essence of palliative care, which is to improve the quality of life and allow patients to die comfortably and naturally. Consequently, in the aftermath of suicide, team members are often overcome by a sense of guilt and failure, 8 especially after the palliative care team has established close and supportive relationships with the patient.
When such trauma happens, it becomes even more vital for the team to take time to process their emotions and thoughts to facilitate psychological closure—which is the task of coming to terms with a traumatic event and finding a sense of resolution. As an organization, we came up with some practical and compassionate steps (which we have coined HEAL—refer to the Table) to support the palliative care team through this healing process.
Table: Practical Framework for Handling Patient Suicides
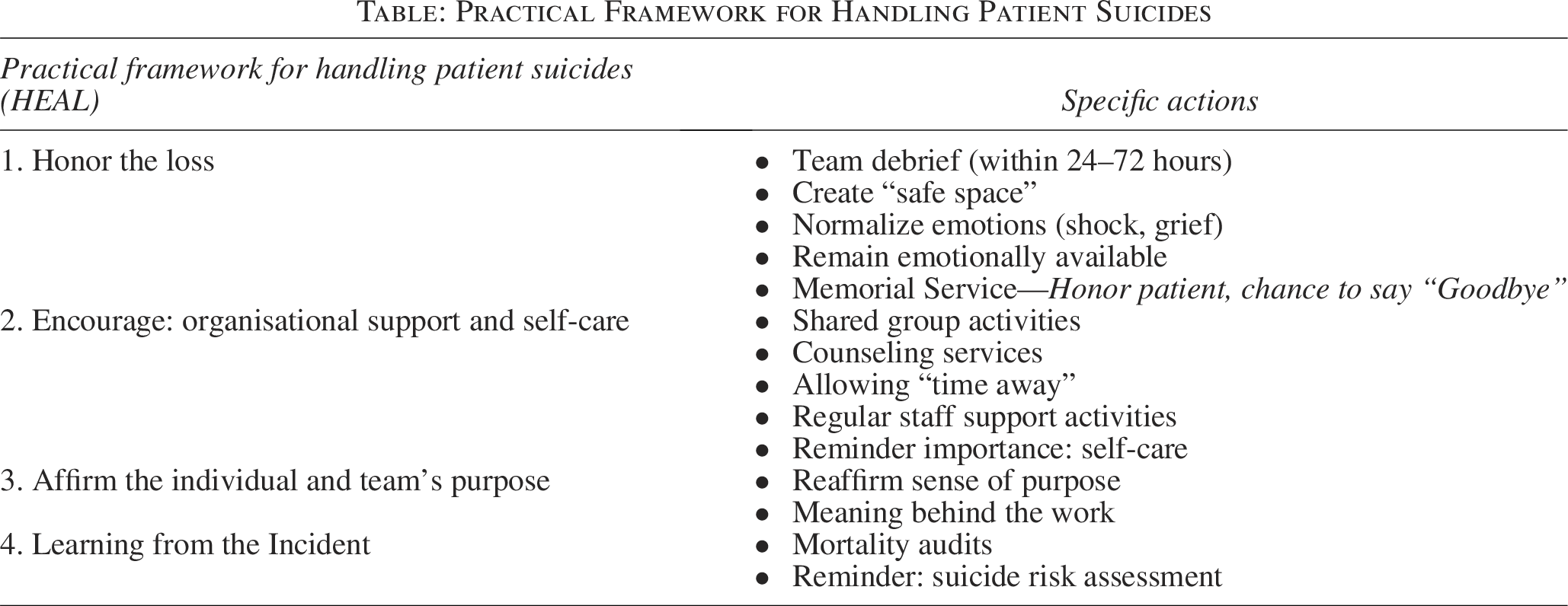
H: Honor the loss
A senior palliative care physician and the chief social worker facilitated a team debrief the next day, within 24 hours of the suicide. We found the defuse and debrief principles of the Critical Incident Stress Debriefing 9 useful in providing a framework to respond to the suicide event. Defusing is done within hours of the suicide for those involved for the purpose of assessment, triaging, and acute mitigation for staff who may be emotionally affected by the event. The facilitators reassured the team that the suicide should not be attributed to the fault of any individuals on the team and normalized the emergence of emotional responses like sadness, grief, and even guilt. They also remained available to support any member of the team who required further one-to-one conversations.
We observed, however, that due to the highly relationship-focused nature of palliative care work, staff often gravitated towards the primacy of the demised patient’s needs above theirs. This necessitated the earlier introduction of a memorial service to facilitate reconciliation of the loss, underscoring the need to view the commemoration of the patient as an integral part, as opposed to a separate process of caring for the staff in response to patient suicides.
Conducting a more formal team debriefing (within the first 72 hours following the incident) and organizing a memorial service 10 allowed the team to honor the late patient, reflect on the impact of the loss, and share their feelings openly. This process not only helps to reduce psychological distress but also leverages communal means of processing the shared experience of grief, trauma, and loss among team members. Facilitating such sessions in a safe space will encourage open and nonjudgmental discussions, fostering greater psychological safety within the team.
E: Encourage: Organisational support and self-care
Our chief social worker facilitated a group support activity one month after the patient’s suicide. The team came together to create craftwork to remember Mr. T. Subsequently, every member of the team took turns to share about their interactions with him and “wished him well” and bade a proper farewell to him. We also reminded the team that the leaders were always available for one-to-one conversations with them and that the organization also provided external counseling for those who felt they needed it.
As recommended by the WHO Suicide Prevention Toolkit, 11 encouraging team members to utilize the counseling services is a tangible way to show that their well-being is a priority. Some may find it beneficial to speak with a mental health professional about their experiences rather than their direct supervisors. If a team member is visibly affected by the patient’s suicide, allowing them to take time away from their duties to process and “re-center” themselves is a clear demonstration of organizational support.
Our organization also conducts regular staff support sessions, during which the team engages in various experiential activities such as art or music-assisted activities or mindfulness exercises. These regular programs provide a platform for staff to reflect, normalize, and talk to each other about their challenges and coping styles. It creates an environment that encourages authentic sharing and fosters greater team connection and trust, which ultimately helps in reducing staff burnout and building individual and team resilience. 12
We also reminded staff of the importance of self-care during these sessions. 13 Coping mechanisms like physical well-being, clinical variety, setting boundaries, transcendental (meditation and quiet reflection), passion for one’s work, realistic expectations, remembering patients, and organizational activities were associated with lower burnout.
Vicarious exposure to pain, suffering, and loss is inherent to palliative care, which underscores the importance of integrating staff support measures as part of organizational culture to reduce the impact of occupational trauma.
The chief social worker and senior palliative care physician (leaders), while providing direct support to the affected staff, also experienced their own grief and trauma. They modeled vulnerability and shared their feelings of shock and sadness openly—thereby allowing the staff to “normalize” their grief and be able to openly share their own feelings. The leaders also used their individual coping strategies, like seeking support from their own social and/or religious networks.
A: Affirm the individual and team’s purpose
The senior palliative care physician reminded the team that Mr. T had enjoyed his sessions during the initial two months, where he looked forward to coming to hospice daycare. He was able to manage his dyspnea better and had also made functional improvements after pulmonary rehabilitation.
With the trauma of suicide, intense emotions often set in, and the staff’s worldviews and professional values may be challenged. Some may even start questioning if they are in the right profession. It is therefore crucial to help affirm the staff and team’s purpose and help them reconnect with the ultimate meaning behind their work in palliative care.
L: Learning from the incident
Conducting mortality audits is a crucial part of the learning process. It allows the team to review the case and identify “gaps” in the care and other areas for improvement. This learning process is vital for the team’s growth and development, empowering them with the knowledge and skills to better manage such complex cases in the future. It is important that these reviews are conducted compassionately and without attributing blame to any individual or the team. Such case reviews also serve as a reminder of the importance of suicide awareness and the need for continued support to patients and their family members.
Regular training on recognizing and supporting patients at risk of suicide is a key part of equipping the team with the knowledge and skills they need. This training helps them feel more confident and empowered in managing similar cases. It also provides them with opportunities for professional growth.
Conclusion
Caring for palliative patients can be profoundly rewarding but also intensely emotional, especially after a patient suicide. Leaders and organizations play a critical role in recognizing patient suicides as traumatic events that pose a serious occupational health risk. Honoring the loss, encouraging and supporting the team, affirming a sense of purpose, and learning from the incident are paramount to helping the team process, reflect, and establish collective meaning-making and learning so as to move the team from grief to resilience.
Informed Consent
As the patient had passed on, informed consent was sought and granted by the patient’s surrogate decision-maker (spouse). The article also complies with ethical guidelines for managing posthumous data.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.