
Abstract

Entering the world of palliative care (PC), we discover the limits of medical science and how natural and inevitable death is, sooner or later. We learn how much suffering and even shortening of life may be promoted by therapeutic obstinacy, understood as medical interventions aimed at preserving biological life regardless of the associated burden, even when known to be incapable of preventing an anticipated and irreversible death.1–3 The concept of therapeutic obstinacy is the fruit of the questioned paradigm of medicine that aims to maintain the biological organism at any cost, viewing death as failure. This, in turn, reflects on health care professionals who deny the dread inherent in death, placing their overconfidence in the belief that all death can be prevented. However, since my residency in PC, I have noticed these same highlighted elements in health care professionals specialized in and working with PC.
I remember when I experienced this, though I could not yet name it. I was working in a home hospice service, and the team cared for an elderly woman with advanced-stage cancer, a matriarch with a strong personality marked by a high sense of self-care who took pride in her appearance. She was also determined to remain at home and no longer receive chemotherapy, which came as a shock to her family. Was it a matter of her understanding of the diagnosis and prognosis? No, she was as lucid as anyone can be, and discontinuing chemotherapy was technically acceptable, given that the metastases were unlikely to respond to further treatment.
The team began to be affected by the conflict between the patient and her family. If it wasn’t a matter of understanding, perhaps it was a matter of psychological coping. That’s when I stepped in—as the psychologist who could support both the patient and her family and try to mediate the situation. However, I came to realize that this divergence was a symptom of each party experiencing their own idiosyncratic suffering: the matriarch held on to her dignity through self-care and self-image and didn’t feel like herself when being manipulated in a hospital setting or subjected to the side effects of chemotherapy; the family loved her deeply and felt that this decision would shorten their remaining time with her.
Even so, despite acknowledging the patient’s autonomy, the team continued to struggle with the discomfort that lingered in the home during our visits, leaving us feeling frustrated and powerless. After several meetings with the patient and family, as well as within the team itself, I began to ask: “Is the patient lucid and capable of making her own decisions? Is she aware of the risks she is taking by choosing this path, regarding both the medical possibilities and her family’s expectations? Are we doing everything we can on our part?” The answers were three “yeses.” Then I asked one final question: “So why are we suffering so much?”.
Strauss and her team identified five elements that compose the compassion of health care professionals toward patients. I consider the fourth element the most challenging, as it is “tolerating uncomfortable feelings aroused in response to the suffering person so remaining open to and accepting of the person suffering”. 4 (p.19) Being successful in this acceptance will determine whether compassion will occur or lead to compassion fatigue.
If therapeutic obstinacy can be reduced to the denial of the fact that death is ultimately inevitable, what is the analogous and inevitable fact whose denial may lead to palliative obstinacy? As Garcia so graciously approached, there is a fraction of suffering that may be intolerable, even when the person is cared for. 5 Adding to the discussion she brings, the philosopher of pessimism, Schopenhauer, influenced existentialism when he understood suffering as an unavoidable part of life. 6 Humanistic existentialist Viktor Frankl brought us the axiom of the tragic triad in his logotherapy, which is composed of suffering inherent to life: guilt, death, and pain (a broad concept of pain, not much different from Saunders’). 7 Therefore, the fact whose denial may lead to palliative obstinacy is the fraction of suffering that is inherently human and, therefore, inevitable. So, how do we perceive this obstinacy?
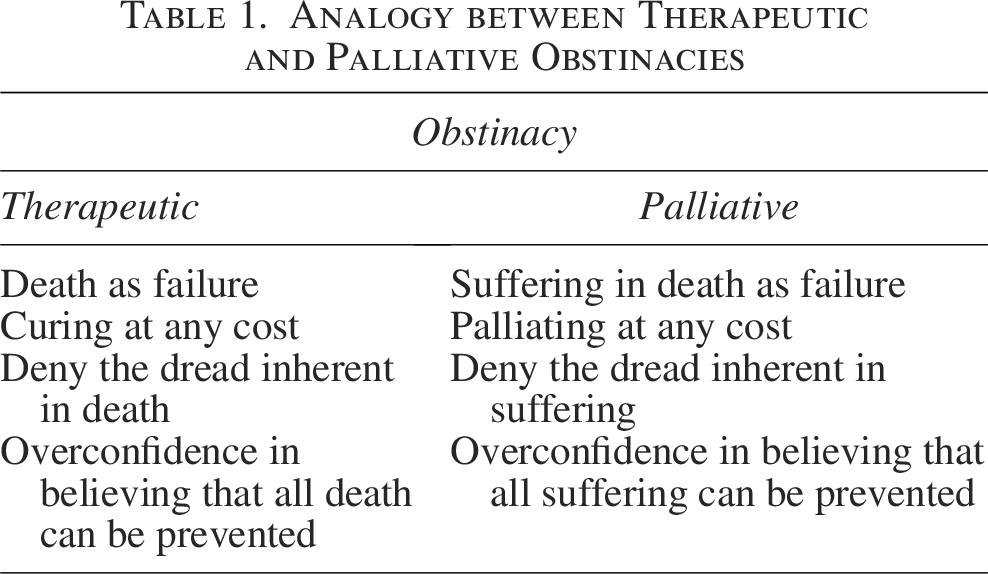
The sense of failure arises when death occurs accompanied by suffering and efforts are made to palliate at any cost. The professional or team denies the dread inherent in suffering (the “impalliable” suffering), a fruit of overconfidence in believing that all suffering can be prevented. Table 1 surmises this analogy.
Analogy between Therapeutic and Palliative Obstinacies
We, as a team, had made every effort to improve the relationship between our patient and her family. Still, there remained a very specific knot we could not untangle, one that made itself present in each person living through this delicate moment, like a thorn no one could quite forget.
With all this in mind, I do not mean to suggest that there is any form of suffering we should ignore, nor that we should leave it solely to the patient. I acknowledge and emphasize the importance of considering and alleviating all suffering to the fullest extent possible. After all, this reflection is focused on the healthcare professional, not on PC or the patients themselves.
The share of inevitable suffering marks a limit—not the limit of the health care professional, but the existential limit of the human condition. What I call overconfidence is the expectation of alleviating even this kind of suffering. When faced with this impossibility, the professional may feel powerlessness, a manifestation of underconfidence merely reflecting the frustrated overconfidence. Ideally, however, expectations should align with reality in the exact measure of confidence: no more, no less.
Well, what can we do about this? Identifying this is a great first step. Asking ourselves, “How much of this suffering is the patient’s and how much is ours?” is a good way to begin. After recognizing this boundary, it is important to respect it and care for oneself. After all, when we say that the patient is a person before being a patient, we must also acknowledge that we are people before being professionals.
Authors’ Contributions
L.B.H.: Conceptualization (lead); writing—original draft (lead); writing—review and editing (lead). D.N.F.: Supervision (lead).
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There is no funding to report for this submission.