
Abstract
Palliative care (PC) clinicians regularly encounter a spectrum of coping strategies, from responses such as humor, legacy-building, and meaning-making to more ambivalent behaviors such as avoidance, splitting, or control-seeking. Supporting adaptive coping is central to the role of all interprofessional PC clinicians to improve quality of life and patient outcomes. Drawing upon principles from psychotherapy, behavioral medicine, and PC research, this article provides guidance to understand, assess, and engage with patients’ coping with intentionality. Harnessing a shared language and approach allows teams to align, self-reflect, collaborate, and respond with greater nuance and empathic attunement during profound moments in our patients’ lives.
Keywords
Introduction
Coping is fundamental to the human condition and the serious illness experience. At its core, coping refers to the cognitive and behavioral efforts an individual makes to manage a situation appraised as stressful, distressing, or overwhelming. It includes varied conscious and unconscious strategies aimed at maintaining psychological integrity amid such stressors; rather than a singular act, coping is a dynamic process of adaptation that can shift as inputs shift.1,2
Palliative care (PC) clinicians regularly encounter a spectrum of coping strategies, each shaped by an individual’s psychological history, cultural background, support systems, and the demands of their illness. Understanding how patients cope—and how we, as clinicians, can best support adaptive coping—is central to our role.2–4 Adaptive coping strategies (whether problem-focused strategies, emotion-focused strategies, or meaning-focused strategies) 2 are associated with lower psychological distress, improved symptom management, and better prognostic awareness, allowing patients to make more informed decisions about their care.5,6 Supporting coping is not an adjunct of PC; it is central to our interprofessional work.
This article addresses the wide array of normative coping responses of patients and families. In cases where coping is severely impairing function, leading to extreme distress, exacerbating psychiatric symptoms and conditions, or obstructing engagement with care, specialized mental health intervention may be indicated. 7 PC social workers can help determine when support beyond their mental health expertise or that of the specialty PC interprofessional team may be necessary.
By integrating principles from psychotherapy, behavioral medicine, and PC research, this article offers practical tips to help clinicians better assess, support, and engage with patients’ coping mechanisms (see Table 1).
Top Ten Tips Palliative Care Clinicians Should Know About Supporting Coping in Serious Illness
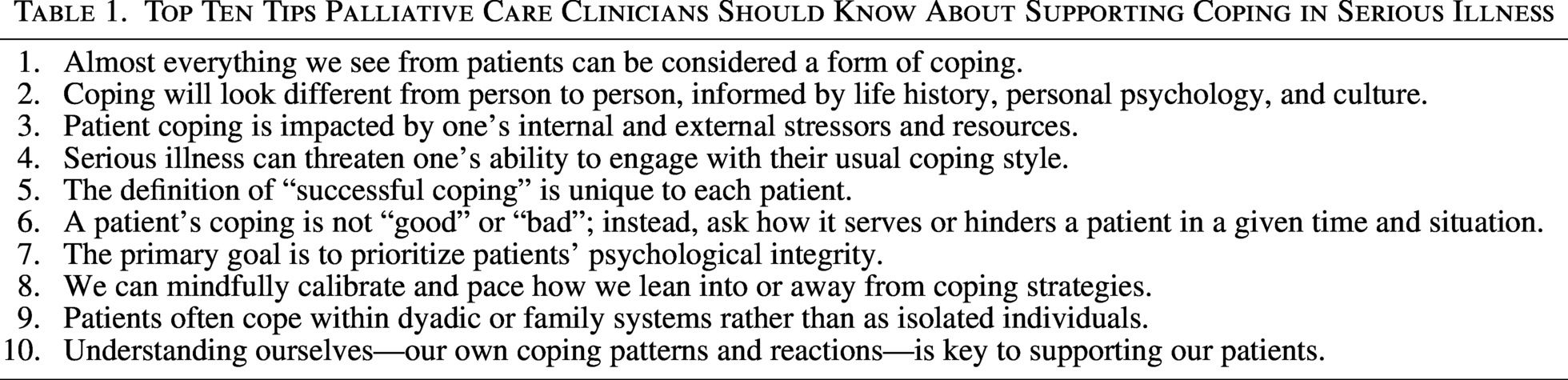
The behaviors of patients with serious illness and their families—whether expected, surprising, or deeply challenging—can be understood as efforts to preserve psychological integrity amid profound uncertainty and difficulties. As clinicians, we can adopt a stance that assumes most patients are doing the best they can with the internal and external resources available to them (see Tip 3).1,2 Framing patient behavior in this way allows us to conceptualize their responses as a form of coping, arising from their attempts to manage distress, assert agency, or maintain a cohesive sense of identity amid loss.
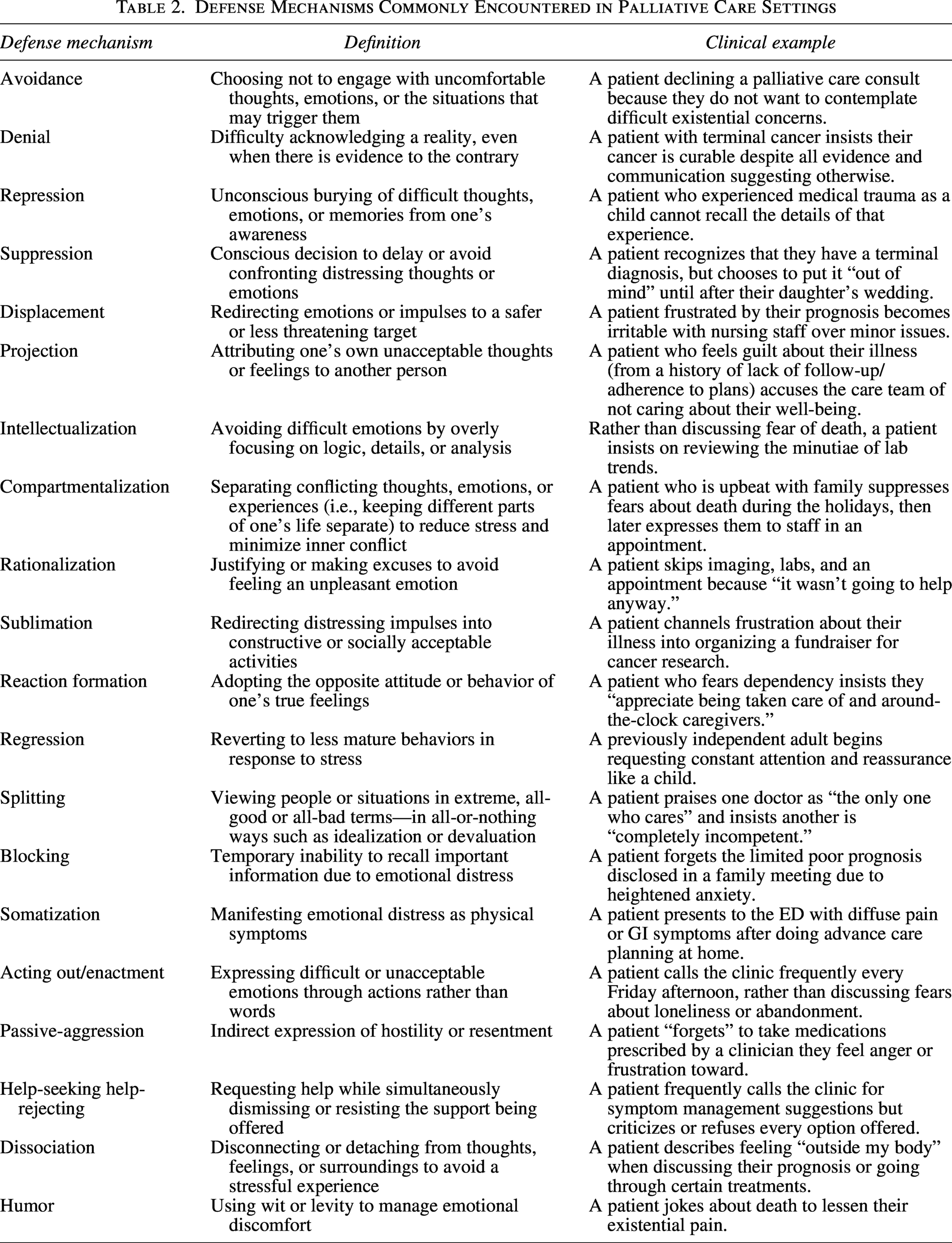
Coping strategies span a broad, normative spectrum, from meaning-making and humor to avoidance or control-seeking.8,9 Some are conscious and intentional, while others arise more automatically—often referred to as defense mechanisms. Defense mechanisms are a specific subset of coping responses, typically rooted in the unconscious, that protect patients from overwhelming affect that threatens psychological intactness. Table 2 outlines several defense mechanisms commonly encountered in PC settings.
Defense Mechanisms Commonly Encountered in Palliative Care Settings
Some coping strategies may be comfortable or even uplifting for clinicians to witness; other behaviors that seem disruptive—such as missed appointments, emotional outbursts, or repetitive questioning—often reflect a patient’s attempt to manage internal distress. Recognizing these behaviors as protective, rather than oppositional, enables clinicians to engage with greater empathy and clinical creativity. This perspective preserves the therapeutic alliance by reframing difficult encounters as reflections of suffering.10,11 All patient behaviors are meaningful and worthy of personalized exploration and deeper understanding, inviting the PC clinician to respond with attuned, nonjudgmental support (see Tips 6–8).
Coping is an individual experience, shaped by a complex interplay of personal history, psychological traits, cultural norms, family systems, place, and context. Life experiences—including trauma, loss, and protective factors—inform how a person navigates adversity, often cultivating lifelong coping patterns.1,2 Cultural frameworks further shape distress responses; for example, in some cultures, stoicism and emotional restraint are revered, while in others, open emotional expression is encouraged.12,13 One person may believe that maintaining a “stiff upper lip” signals strength, while another was raised in a family system/culture that values emotional catharsis to “let it all out” in processing hardship. Given the diversity in how patients cope, there is no singular, universally effective response.
Coping strategies often develop to address specific difficulties in certain phases of life but may outlive their usefulness or be seen as unfitting when new struggles present. A person who learned to repress grief as a child to endure an early loss may later struggle to access and process emotions in adulthood, particularly when facing the losses inherent to serious illness (see Tip 6).
Clinicians can remain patient-centered by adopting curiosity over judgment. Inquiry into how patients have historically navigated stress, hardship, illness, and loss can provide valuable insights into both their distress and resilience. Questions such as, “What has helped you manage difficult times in the past?” or “What is important for us to know about you as a person?” 9 invite reflection and empower patients to articulate their coping needs. 14 This approach deepens the therapeutic alliance and enables clinicians to tailor interventions that align with patients’ strengths and values.
Coping is influenced not only by present circumstances and stressors but also by the internal and external resources available to a patient. Stressors may be external (e.g., financial strain, housing instability, transportation insecurity) or internal (e.g., high symptom burden, underlying psychiatric illness, cognitive limitations). 13 Conversely, resources may also be both internal (e.g., psychological resilience, prior adaptive coping strategies, a sense of meaning and purpose) or external (e.g., family and social supports, access to medical care, financial security). 15
The same diagnosis may be a radically different experience from one patient to the next depending on this interplay of stressors and supports, underscoring the profound impact of social determinants of health. For example, financial insecurity can overwhelm a patient’s coping capacity, leading to higher distress, difficulty accessing care, and increased symptom burden. Conversely, higher education has been shown to be protective, like enhancing problem-solving abilities, self-advocacy, and access to health-related information.13,15
Additionally, the equilibrium between stressors and resources is not static—as patients experience shifts in their disease status, debility, social networks, and external environment, their coping capacity continually adapts. 5 Clinicians can support patient coping by identifying the highest-yield intervention points within this dynamic equilibrium. Depending on the patient, interventions may include the reduction of internal or external stressors, the enhancement of external resources, or the bolstering of internal coping capacity. 16
Clinicians can aim to integrate multiple factors simultaneously. For example, if a patient struggles to attend appointments due to transportation barriers (external stressor) but finds emotional grounding in speaking with a close friend (coping resource), the team might suggest arranging that friend to drive and accompany them to their visits. By taking a holistic view of stressors and resources, PC clinicians can help patients adapt their ability to cope and maintain psychological intactness.
Coping mechanisms serve as essential buffers against stress and adversity, allowing individuals to maintain psychological equilibrium in the face of life’s challenges. However, serious illness can disrupt daily routines, functional status, and self-identity, often dismantling previously reliable coping strategies and leaving patients feeling emotionally destabilized. For instance, individuals who have relied on physical activity to manage stress may find themselves unable to engage in exercise due to fatigue, pain, or functional limitations, while those who use creative outlets such as music or writing for emotional processing may struggle with cognitive impairment or loss of fine motor control.17,18
Physical, emotional, and existential threats posed by serious illness can undermine one’s ability to engage in preferred coping strategies, leading to distress and a fundamental shift in self-identity. This shift can be distressing for individuals whose coping strategies are intertwined with core personal values such as autonomy, productivity, or physical vitality.3,6 Patients may feel a profound sense of loss when they are unable to engage in activities that once provided meaning and stability, contributing to emotional dysregulation, anxiety, depression, demoralization, and even existential despair. Furthermore, the unpredictability of serious illness can erode patients’ sense of control, making structured problem-solving strategies less effective and fostering a sense of helplessness. 4 When individuals (whether patients or caregivers) perceive their coping resources as insufficient or ineffective, they are at greater risk of regressing to less adaptive strategies, including avoidance, withdrawal, or rumination.2,3
There is no singular “right” way to cope with serious illness; coping is a highly individualized process (see Tips 2 and 3). For example, while some patients prefer a structured, problem-focused approach—such as meticulously researching treatment options—others may cope best through meaning-making, spiritual reflection, or reliance on social support networks. 19 Furthermore, since coping needs to evolve through the illness trajectory, it is best to avoid assumptions about what constitutes “effective” coping (see Tip 8). For instance, one patient may find that detailed discussions about treatment side effects help them feel grounded and prepared, whereas another patient may experience heightened anxiety from that same information.
“Success” for one patient may simply be making it through the day without a harmful outburst at loved ones, while for another, “success” may be completing an autobiographical novel. Ultimately, by validating the diversity of coping styles and avoiding one-size-fits-all models, PC teams can embolden patients to navigate their illness in a way that aligns with their values, needs, preferences, and emotional/psychological resources.
Dichotomizing coping as “good” or “bad” fails to capture the nuance in patients’ psychological landscapes. Every coping mechanism serves a function, whether to provide emotional regulation, preserve a sense of control, or shield against overwhelming distress. Rather than labeling a patient’s coping as effective or ineffective in absolute terms, clinicians can explore how a given strategy serves or hinders a patient at different points in their illness trajectory. 20 Recognizing the protective value of coping mechanisms—while also considering when they may become limiting—allows for a more patient-centered and empathic approach. 5
The role of a given coping strategy may differ between patients. For instance, humor may be a grounding and reassuring tool for some patients, while for others, it may function as an avoidance strategy that inhibits deeper emotional processing.
Coping strategies vary not only by patient but also by context. A given approach may serve a patient well in one situation but become limiting in another. For example, a patient who compartmentalizes—intentionally setting aside thoughts of illness—may benefit from this strategy during a family trip, allowing full engagement with loved ones. Yet the same compartmentalization strategy may hinder necessary future planning when adult children wish discuss what to expect as the illness progresses.10,11
The impact of coping strategies may evolve over time and phase of illness. A patient who manages uncertainty by taking an active role—researching treatment options, asking detailed questions, and maintaining a sense of control—may find this approach adaptive during active treatment. However, when transitioning to remission or to hospice, this same active strategy may no longer align with their emotional or existential needs, and a shift toward meaning-focused coping may be more helpful. 19 Understanding the dynamic nature of coping allows clinicians to assess whether a strategy continues to serve the patient’s well-being in the current context and to support flexibility as needs change across time.
The primary goal as PC clinicians should be to prioritize and preserve our patient’s psychological integrity. Rather than viewing certain coping mechanisms as barriers to be dismantled, we should recognize them as structures that provide necessary support. Any defense or coping strategy we observe exists for a reason; it serves a role and that role is to be respected. If a defense mechanism appears to be limiting a patient’s ability to engage in critical aspects of their care, the solution is not to shatter or dismantle it, thereby removing the glue that is holding somebody together. Instead, we can ask ourselves: What alternatives might be supportive that are within the patient’s reach and resources without destabilizing them? (See Tip 8).
This approach does not mean that clinicians should passively accept all forms of coping without engagement. Rather, when we conceptualize the maintenance of patients’ psychological integrity as their most fundamental need, we become more attuned to the ways we can intervene with sensitivity, inclusivity, and respect.11,21 In cases where a coping mechanism is overtly harming a patient—such as avoidance leading to unmanaged symptoms or denial interfering with critical decision making—clinicians can incrementally introduce alternative supports, aligning with what the patient can tolerate or accept at the moment (see Tip 8). By focusing on preserving rather than threatening psychological integrity, we are best positioned to offer interventions that serve both immediate psychological stability and long-term well-being. 22
While striving to help our patients maintain their psychological integrity (see Tip 7), clinicians also work to guide patients toward their most adaptive coping mechanisms. Clinicians can mindfully calibrate their approach to lean into or away from a given coping strategy. When a coping strategy seems to be serving more than hindering, clinicians can actively reinforce and amplify it. For example, a patient who feels intact and stable through control and agency may be more engaged in care discussions when their autonomy is supported. In this case, a clinician might encourage them to write down their questions, structure treatment regimens that allow for self-titration, or offer clear and explicit expectations about appointments and decision-making timelines. These strategies align with the patient’s intrinsic coping style, allowing them to remain engaged in a way that feels authentic, stabilizing, and grounding.20,23,24
Conversely, when a coping strategy seems to be hindering more than serving, clinicians may need to gently pace their approach. Consider a patient who remains highly focused on logistical planning or symptom management to avoid engaging with their existential distress. Rather than forcing a direct confrontation with mortality before they are ready, the clinician can help channel their need for structure into discussions that still support future planning—such as framing advance care directives as “contingency planning” rather than end-of-life preparation.4,6 If that is still too overwhelming, the clinician may recalibrate to an even gentler approach, such as “talking about talking about it”—a method in which the clinician invites a meta-conversation about readiness before addressing the difficult truth directly (e.g., “I am wondering what will help us know when it might be a time to start thinking about contingency planning together?”).
When leaning away from the coping mechanism, several key considerations inform the pace and intensity of this shift:
Case parameters: What is the prognosis? How urgent are the medical decisions at hand? Patient response: Did the patient flexibly tolerate the shift, or was it overwhelming and stifling? Alternative supports or strategies: If moving away from a defense, what replacement strategies can we foster? Can we bolster other existing coping skills or introduce new ones that seem fitting to the patient?
For some patients, even subtle attempts to shift away from a defense may cause harm, requiring that the care team instead adapt to the patient’s existing coping structures as they are and consider if further mental health support is indicated. For others, a clinician’s presence and skillful pacing of how they lean into or away from certain coping strategies can bolster the patient’s ability to cope. Regardless, we support patients in harnessing the most adaptive coping that is accessible to them, while also nonjudgmentally accompanying all coping that emerges.
Coping with serious illness is not an individual endeavor; it frequently unfolds within dyadic systems or broader family networks. 25 Families function as dynamic systems in which stress, coping, and emotional responses are interconnected. The systemic impact of illness means that a partner’s distress, for example, can shape the patient’s emotional well-being and vice versa.
For many patients, a partnered relationship may serve as a central unit of emotional and practical support, where the individuals often develop interdependent roles in response to illness.26,27 This goes beyond simply assuming “patient” and “caregiver” roles. Within these dyadic coping systems, for example, one partner may assume the role of “planning for the worst” while the other assumes the role of “optimizing joy in the present”; alternatively one partner may assume the role of “intensely advocating” with the medical team while the other assumes the role of “amicably building rapport.” Recognizing and naming each partner’s contribution can provide valuable insights into their coping mechanisms and highlight opportunities for tailored interventions.12,26,27
Recognizing the relational nature of coping allows PC clinicians to conceptualize the coping of the “system as a whole” to which all other tips in this article can be directly applied. For example, PC teams can facilitate guided conversations that help couples redefine their roles, validate emotional responses, and develop shared meaning around their experience.26,27 Fostering resilience at the level of the family system, as collective coping, has been shown to buffer against existential distress and improve quality of life for both patients and caregivers.3,5
The collective dimensions of who we are—our experiences, beliefs, biases, identities, cultural backgrounds, family systems, personalities, and coping mechanisms—shape the lens through which we perceive and interact with patients. These factors influence our interpretations about what is reasonable, problematic, abhorrent, admirable, or concerning in others.10,11 Clinicians’ personal beliefs may affect responses and interpretations of patients’ coping. For instance, a clinician who associates raised voices with conflict may perceive a loud patient as aggressive, rather than expressive. Moreover, a clinician who values patient autonomy may perceive a patient who relies on family for decision making as overdependent or helplessly reliant. An extroverted clinician might misinterpret an introverted patient’s quietness as disengaged and judgmental, rather than introspective and reflective.
While we strive for clinical objectivity and equity, our perceptions are inevitably influenced by personal experiences. Recognizing our emotional responses—such as feeling particularly drawn to or avoidant of certain patients—offers valuable insights into unconscious biases and countertransference.10,22 For example, consistently spending more time with certain patients, delaying interactions with others, or selectively sharing personal information may indicate underlying biases. Acknowledging countertransference is not inherently negative; rather, it provides an opportunity for more expansive self-awareness, attunement, and greater inclusivity in patient care.11,28,29
Assumptions and judgments can arise not only with patients who differ from us in culture, faith, identity, or language but also with those who share similar backgrounds, potentially leading to overidentification and projection of our own perspectives. For instance, two patients with financial insecurity may develop opposite coping mechanisms—one practicing extreme frugality, another spending freely to avoid feelings of deprivation. Without self-awareness, clinicians risk imposing their own frameworks onto patients instead of understanding (or immersing into) their unique perspectives and lived experiences.
As we traverse different life stages, our perspectives and potential for countertransference evolve. A young, unpartnered clinician may have a different lens than they will later in life when partnered, parenting, retiring, or facing their own aging and mortality. The task is not to eliminate our subjective lens but to cultivate an awareness of it, using reflection to enhance, rather than obstruct, compassionate, and personalized patient care. 10
Conclusion
Coping is central to the experience of serious illness. As PC clinicians, we are consistently bearing witness to patients’ efforts to adapt and preserve their sense of self in the face of often devastating realities. The behaviors we observe are nearly always attempts at coping. By embracing a framework that assesses these behaviors through a psychologically informed lens, we are better able to support patients in maintaining integrity while also fostering adaptive coping. Harnessing a shared language and approach allows teams to align, self-reflect, collaborate, and respond with greater nuance and empathic attunement during profound moments in our patients’ lives.