
Abstract
Palliative care clinicians will regularly take care of patients with diabetes and play numerous roles in educating not only patients but also families and care partners regarding the changing balance of harms and benefits of blood glucose control as patients near end of life (EOL). There is limited evidence regarding the optimal timing and process for de-escalation of blood sugar monitoring and diabetes medications (including insulin) in the hospice and EOL setting. Rather, decisions are guided by prognosis, impacts of hypo- or hyperglycemia on a particular patient’s symptoms, and the burdens of specific diabetes medications or interventions. Shared decision-making with patients and care partners is essential, as is addressing the emotional impact of changes to diabetes routines, which some patients have adhered to for many years. Diabetes also impacts overall symptom control at EOL. These ten tips guide palliative care clinicians to identify and address the impact of glycemic control, diabetes medications, and common long-term complications of diabetes on symptom burden.
Keywords
Introduction
Approximately 11.6% of the U.S. population has diabetes; this percentage increases to 29.2% among older adults over the age of 65. 1 Primary care and palliative care clinicians may not specifically address the changing goals of diabetes management as patients near the end of life (EOL), which can leave patients and their care partners feeling confused or abandoned as they navigate diabetes care. 2 Clinicians also demonstrate variation in their familiarity or comfort with managing diabetes in the palliative care setting. 3
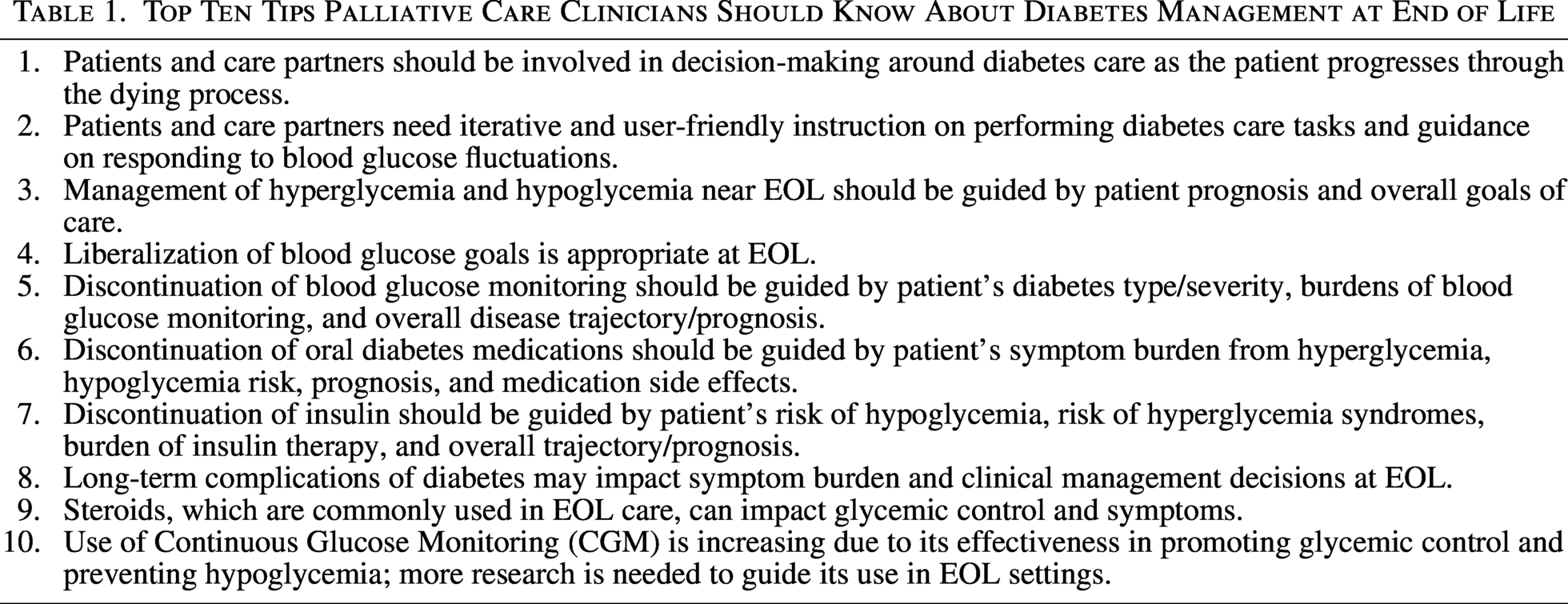
Long-term complications of diabetes include retinopathy, neuropathy, nephropathy, cardiovascular disease, and peripheral arterial disease, all of which can increase symptom burden and decrease quality of life, even in advanced stages of other illnesses. Palliative care clinicians are poised to alleviate symptoms arising from these complications, as well as guide patients and their care partners through the transitions of diabetes care, from a focus on long-term complication prevention to short-term symptom management. With this article, we offer ten tips that provide clear, consistent, person- and family-centered guidance for EOL care for patients with diabetes (Table 1).
Top Ten Tips Palliative Care Clinicians Should Know About Diabetes Management at End of Life
Tip 1: Patients and Care Partners Should Be Involved in Decision-Making Around Diabetes Care as the Patient Progresses Through the Dying Process
It may be difficult for patients to adjust to changing blood glucose goals and de-escalation of medication therapy as they near EOL. Those who have closely managed their diabetes may struggle to let go of medications, insulin administration, or routine blood glucose checks. Clear descriptions of the rationale for liberalizing blood glucose goals and deprescribing diabetes medications, as well as allowing patients to express their preferences regarding if and when they are ready for these changes, can prevent feelings of abandonment or hopelessness that can occur if patients perceive that clinicians have suddenly lost interest in blood glucose levels.2,4 Having conversations about the patient’s expected prognosis (if the patient desires this information) can facilitate discussions around the utility of continued strict blood glucose control, allowing discussions to be anchored in the time to expected benefit of these interventions.
It is also important to involve care partners early and often. Care partners play an important role in helping patients to navigate the multitude of decisions and changes that come with EOL care. 5 For patients with diabetes, some care partners find routine diabetes tasks (e.g., checking blood glucose or administering insulin) to be highly burdensome, while others may find these tasks to be an important source of control and opportunity to demonstrate caregiving. Conversations around diabetes care tasks can be an opportunity to further explore the care partner’s expected role in assisting with routine diabetes tasks, assess their comfort level and emotional preparedness for these tasks, and provide anticipatory guidance on the way their role might change as the patient’s clinical status declines. Furthermore, these conversations can serve as a reminder to explore the care partner’s understanding of the patient’s prognosis and expected trajectory. It can also be an impetus to leverage the interdisciplinary team if the care partner requires additional coping support amid the patient’s declining clinical status. Finally, involving care partners early can help to avoid conflicts (for example, a scenario in which care partners are focused on blood glucose levels or medication adherence while the patient may prioritize minimizing interventions and liberalizing diet).
Tip 2: Patients and Care Partners Need Iterative and User-Friendly Instruction on Performing Diabetes Care Tasks and Guidance on Responding to Blood Glucose Fluctuations
For patients with a longer prognosis (e.g., many years), routine diabetes care tasks such as blood glucose monitoring and use of diabetes medications can be crucial to effectively manage the condition and prevent complications. Empowering patients and care partners with the knowledge to manage diabetes effectively can significantly improve health outcomes and quality of life. 6 As the patient declines functionally or cognitively, care partners may need to perform diabetes care tasks that the patient was previously performing independently. It is important to educate care partners on the basics of blood glucose monitoring, medication administration, dietary management, wound care, and recognition of hyperglycemia and hypoglycemia.2,4 Practical demonstrations/videos/pamphlets, hands-on training with diabetes educators, and regular follow-up sessions can enhance understanding and adherence and should be tailored to the individual’s needs and literacy levels. As prognosis becomes shorter (e.g., months to fewer years), this education should evolve to include information about the expected illness trajectory, anticipatory guidance around plans to change and ultimately discontinue blood glucose monitoring based on illness stage, as well as the role of complications of diabetes in symptom management at EOL (see Tip 8).
Tip 3: Management of Hyperglycemia and Hypoglycemia Near EOL Should Be Guided by Patient Prognosis and Overall Goals of Care
Managing symptoms of hyperglycemia and hypoglycemia is crucial for patients with diabetes. Hyperglycemia (elevated blood glucose levels) can lead to symptoms such as polyuria, polydipsia, and fatigue. The primary goal of managing hyperglycemia in EOL settings is to treat and prevent these symptoms and prevent hyperglycemia syndromes like diabetic ketoacidosis (DKA) or hyperosmotic hyperglycemic syndrome (HHS), which can lead to increased symptom burden. DKA is typically associated with a blood glucose level of >250 mg/dL, and HHS is typically associated with a blood glucose level of >600 mg/dL, though there is substantial potential for overlap between the two syndromes. 7 While there are no guidelines discussing how to treat symptomatic hyperglycemia near EOL, it is appropriate to test blood glucose if it is suspected that a patient is experiencing bothersome symptoms due to hyperglycemia and to administer short-acting insulin based on a sliding scale once hyperglycemia is confirmed. 8 Sliding scale doses should be derived from the patients previous regimen or, alternatively, using the institutions low-dose or sensitive sliding scale. Symptoms can also be targeted individually (e.g., use of antiemetics for nausea or ensuring adequate availability of water if the patient reports thirst). For patients with a prognosis of weeks-to-months, nutritional support and encouragement to maintain adequate hydration can also help to prevent severe hyperglycemia.
Hypoglycemia (low blood glucose) presents with symptoms such as shakiness, diaphoresis, confusion, and irritability. Patients often begin experiencing symptoms at a blood glucose level of around 70 mg/dL, though this can vary widely between patients. 9 Severe hypoglycemia can lead to loss of consciousness, seizures, and sudden death. For patients with a prognosis of weeks to months, check glucose levels in patients with acute symptoms of hypoglycemia and treat immediately. Hypoglycemia treatment involves consuming fast-acting carbohydrates like glucose tablets, juice, or candies. Correction of hypoglycemia is likely not necessary or appropriate for those with a prognosis of days-to-weeks or with substantially decreased PO intake, as decreased responsiveness is more likely due to the underlying disease. 4
Tip 4: Liberalization of Blood Glucose Goals Is Appropriate as Prognosis Shortens
As life expectancy decreases, the harm/benefit balance of tight glycemic control changes, favoring liberalization of blood glucose targets. Evidence suggests that there is minimal benefit (in terms of either life extension or reduction in diabetes complications) of tight glycemic control for patients with a prognosis of less than five years. 10 Thus, blood glucose management for patients with limited life expectancy should focus on symptom control rather than prevention of long-term complications. 11 The burdens of overly strict glycemic control also increase at EOL. The risk of hypoglycemia increases in older adults and those with comorbidities; older adults also often have lower awareness of hypoglycemia when it does occur. 8
For many patients, liberalizing blood glucose goals at EOL is ideally part of a longer conversation throughout the aging process. The American Diabetes Association recommends loosening blood glucose targets for all patients with limited life expectancy, multiple comorbidities, or high side effect burden from diabetes medications (including episodes of hypoglycemia), as well as those living in long-term care facilities. 9 If these conversations have been started in the outpatient endocrinology or primary care setting, palliative care clinicians can continue to modify blood glucose targets as prognosis and goals change.
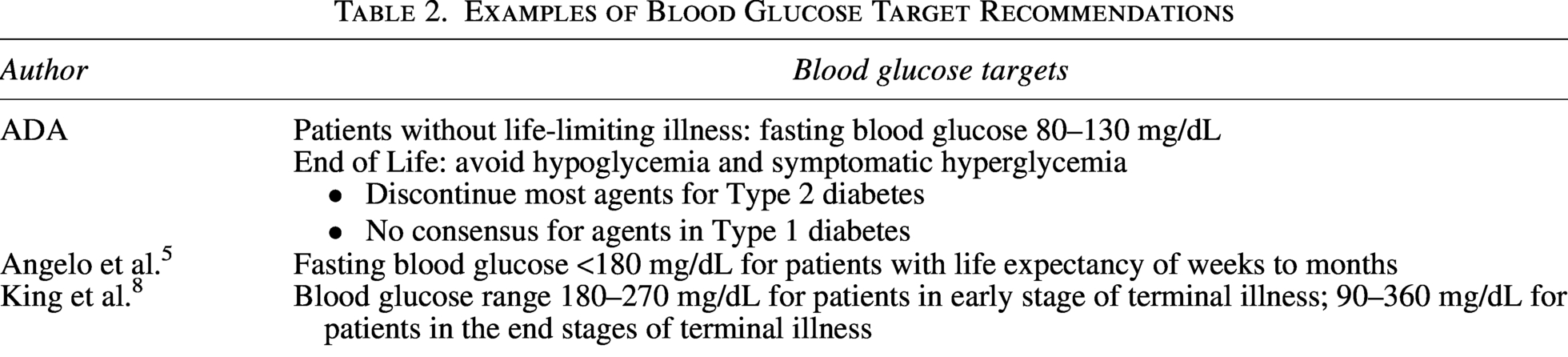
There are no consensus guidelines regarding specific blood glucose targets at EOL. All recommendations acknowledge the prevention of hypoglycemia as a primary goal. 12 Examples of recommendations in the literature are listed in Table 2. Patients may have insight regarding the blood glucose values at which they become symptomatic or have a risk of developing hyperglycemia syndromes (HHS or DKA); this information can be helpful when creating patient-specific recommendations for blood glucose targets at EOL in those patients for whom continued blood glucose monitoring is indicated (see Tip 5).
Examples of Blood Glucose Target Recommendations
Tip 5: Discontinuation of Blood Glucose Monitoring Should Be Guided by the Patient’s Diabetes Type and Severity, Burdens of Blood Glucose Monitoring, Overall Disease Trajectory/Prognosis, and Goals of Care
As previously described, there is minimal benefit of tight glycemic control at EOL, and routine testing of blood glucose levels results in increased burden to patients and care partners. For patients with a prognosis of weeks to months, hemoglobin A1c checks should be discontinued. The patient’s diet should be liberalized, with a focus on eating for pleasure and maximizing enjoyment of food, and dietary modifications to prevent hyperglycemia should be relaxed.6,11,12 Within the last weeks to months of life, the utility of blood glucose monitoring lies in identifying and treating hypo- or hyperglycemia as a source of discomfort for the patient. 4
For patients with non-insulin-dependent Type II diabetes (those on minimal or no insulin without a history of HHS or DKA), there is minimal benefit of point-of-care blood glucose monitoring in either the inpatient or outpatient setting near EOL. Consider stopping routine blood glucose monitoring in these patients when the prognosis is weeks to months. In patients with a prognosis of weeks to months, blood glucose levels can be checked and addressed if the patient is symptomatic; in patients with a prognosis of days or less, hypoglycemia is an expected part of the dying process, and routine monitoring of blood glucose levels is not indicated.6,11,12 It may also be reasonable to check blood glucose levels daily after about one week after stopping glucose-lowering medications. 13
For patients with Type I diabetes or insulin-dependent Type II diabetes, blood glucose monitoring should be continued if the patient remains on insulin (see Tip 7 for recommendations around timing of insulin discontinuation). The frequency of monitoring can be tailored to the individual’s needs (for example, checking for hypoglycemia in the morning or at the time of expected peak action of antihyperglycemics, or checking for hyperglycemia postprandially after the patient’s largest meal). Routine blood glucose monitoring should be stopped once the patient is taking only minimal PO and subsequently can be checked only if the patient is symptomatic and goals align with treatment of hyper- or hypoglycemic states. As above, when the prognosis is days or less, routine blood glucose monitoring is not indicated.6,11,12
Tip 6: Discontinuation of Oral Diabetes Medications Should Be Guided by Patient’s Symptom Burden From Hyperglycemia, Hypoglycemia Risk, Prognosis, and Medication Side Effects
Oral diabetes medications can often be deprescribed when the patient’s prognosis is limited to less than a few years. For patients with non-insulin-dependent diabetes, consider stopping oral diabetes medications when the prognosis is weeks to months, particularly if patients do not report symptomatic hyperglycemia. One study of older adults in nursing homes found no significant increase in hyperglycemia in the month after discontinuation of oral diabetes medications but did find a reduction in hypoglycemia; 14 this study provides evidence that deprescription of oral diabetes medications may be an effective way to lower pill burden without negatively impacting the patient’s overall health and well-being.
In addition to contributing to pill burden, diabetes medications can also increase symptom burden. It is important to maintain a high index of suspicion for identifying when symptoms may be medication side effects. For example, metformin and Glucagon-Like Peptide 1 (GLP1) agonists commonly cause gastrointestinal symptoms including nausea, abdominal pain, and bloating; GLP1 agonists can cause weight loss or poor appetite; and Sodium-Glucose Cotransporter 2 inhibitors can lead to dehydration, orthostatic hypotension, or urinary symptoms. Sulfonylureas are associated with a high risk of hypoglycemia and are often appropriate to discontinue.6,11,12 Even in patients who have previously taken a medication without issue, physiological changes at EOL can contribute to increasing side effect burden. For example, decreasing renal function can lead to a prolonged duration of action for insulin and can lead to impaired excretion of medications (e.g., metformin should be avoided in GFR <30). 15 Table 3 lists examples of common diabetes medications and their side effects. 16
Common Non-Insulin Diabetes Medications and Their Side Effects
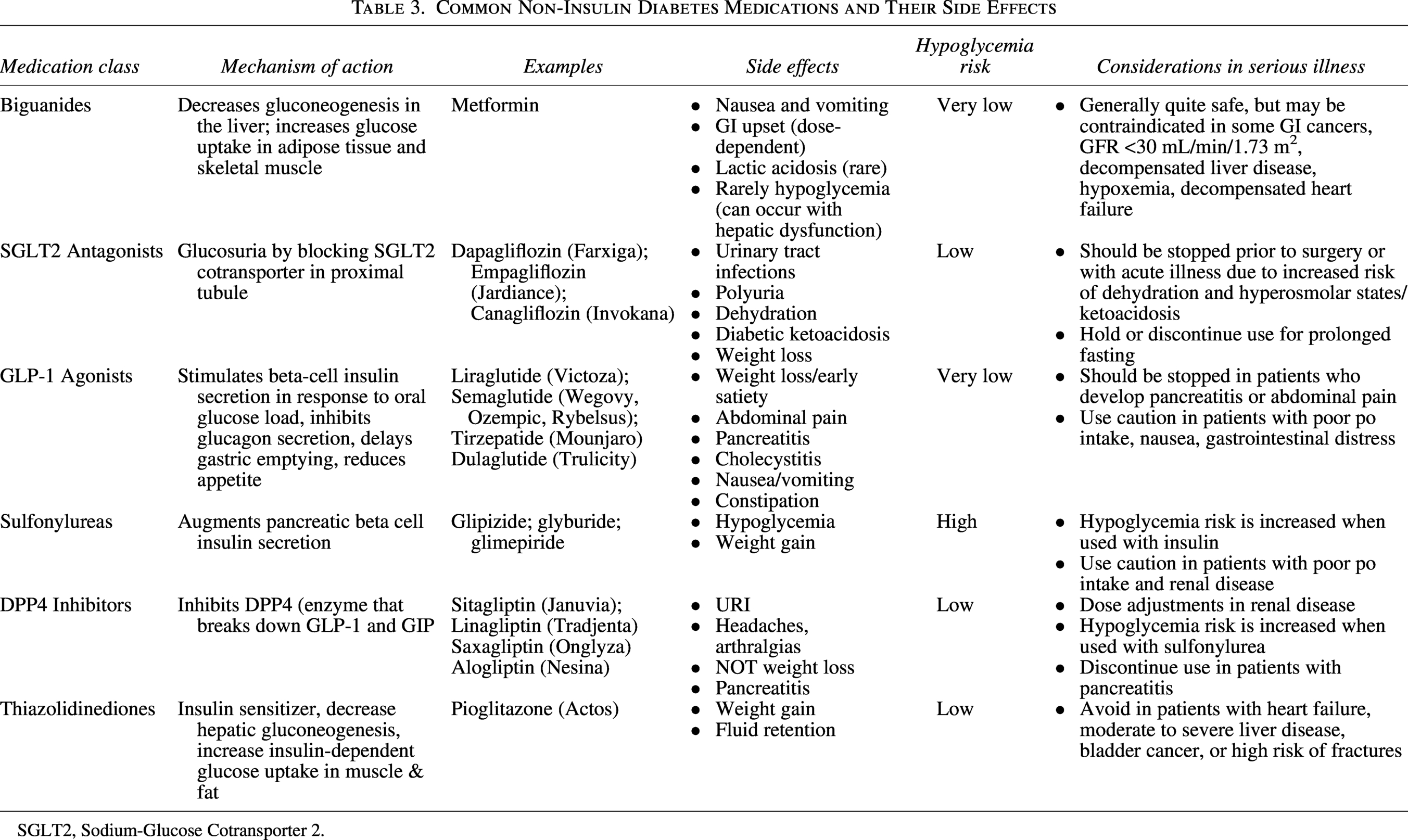
SGLT2, Sodium-Glucose Cotransporter 2.
Tip 7: Discontinuation of Insulin Should Be Guided by Patient’s Risk of Hypoglycemia, Risk of Hyperglycemia Syndromes, Burden of Insulin Therapy, and Overall Trajectory/Prognosis
Some patients may benefit from continued insulin therapy even if the prognosis is limited. Patients with Type I diabetes or insulin-dependent Type II diabetes (e.g., with high insulin requirements or episodes of HHS/DKA) may be at high risk for developing symptomatic hyperglycemia or hyperglycemia syndromes if insulin is discontinued while the patient is still taking normal or nearly normal amounts of food by mouth. In these patients, consider stopping meal-time short-acting insulin first 13 and then decreasing basal insulin dose as patient’s oral intake declines (e.g., halving the dose of basal insulin when the patient takes only 50–75% of meals). In most patients with Type II diabetes, mealtime insulin can be discontinued without issues; patients with Type I diabetes may need continued mealtime insulin if they become symptomatic with long-acting insulin alone. Consider cessation of all insulin therapy once the patient is taking minimal-to-no oral intake (or if the burdens of insulin administration or hypoglycemia begin to outweigh the benefit of preventing symptomatic hyperglycemia).6,11,12
In contrast, for patients with Type II diabetes who are on insulin only to optimize A1c (and without a history of proclivity to HHS or DKA), insulin therapy should be stopped when the prognosis is weeks to months.6,11,12
Tip 8: Long-Term Complications of Diabetes May Impact Symptom Burden and Clinical Management Decisions at EOL
Long-term complications of diabetes (including retinopathy, nephropathy, cognitive impairment, neuropathy, and vascular disease) can lead to increased morbidity for patients near EOL. Retinopathy is present in approximately 25% of patients with diabetes and often goes undiagnosed. The high rates of visual impairments in patients with diabetes underscore the importance of access to visual assistance devices and engagement with written text prior to providing written instructions or communication. 17 In addition to visual problems, people with diabetes have a 5–13x increased risk of developing end-stage renal disease (ESRD), 18 presenting unique challenges to EOL care. Patients with ESRD may defer hospice enrollment because they wish to continue dialysis, and being on dialysis may impact the level of burden of a patient’s existing medical care. Even among patients who maintain some kidney function, the high rate of chronic kidney disease among patients with diabetes necessitates renal adjustment for medications. 18
Palliative care clinicians should be prepared to assess for and address painful diabetic neuropathy, which often presents as burning or tingling pain in the feet or hands and can be extremely bothersome even if the patient’s primary pain concern is related to another pathology. Pregabalin and duloxetine are good first-line agents for painful diabetic neuropathy; tricyclic antidepressants can also be considered. 19 Opioids may be appropriate for refractory cases and when the prognosis is short. 19 Neuropathy can also lead to issues with balance. For patients with good functional status and a prognosis of years, physical therapy focused on balance can prevent falls and improve balance. 20
Additionally, neuropathy and peripheral arterial disease can lead to late identification of wounds, increasing the risk of cellulitis, osteomyelitis, and amputation. 21 The need for amputation can be a negative prognostic factor: one review article found a one-year mortality of 13% and a five-year mortality of 50% after amputation for diabetic ulcers. 22 Wounds and amputations are also associated with a high amount of caregiving requirements, may be painful, and can limit the patient’s mobility. Palliative care clinicians should be prepared to address pain associated with wounds, provide education to care partners regarding wound care, and help to ensure adequate support for wound care during hospice transitions.
Finally, people with diabetes also have an increased risk of cognitive impairment (60% vs. 10% in the general population, according to one study 23 ), which can impact their ability to perform self-care tasks and engage in goals of care conversations. Palliative care clinicians taking care of patients with diabetes should have a high level of suspicion to screen for and identify difficulties with understanding medication regimens or impairments to decision-making capacity; identification of these difficulties should prompt involvement of care partners in education about medication plans and/or complex medical decision-making.
Tip 9: Steroids, Which Are Commonly Used in EOL Care, Can Impact Glycemic Control and Symptoms
Blood glucose often increases in response to systemic corticosteroids. Intermediate-acting glucocorticoids (e.g., prednisone and methylprednisolone) demonstrate peak effects within 4–6 hours of administration that may be more persistent with divided dosing, while long-acting glucocorticoids (e.g., dexamethasone) may have effects longer than 24 hours. Corticosteroids reliably affect postprandial glucose, making short- or intermediate-acting insulin administered with meals a reasonable treatment strategy. 24
Corticosteroids are used frequently at EOL for management of fatigue, nausea and vomiting, anorexia and cachexia, and pain. This may result in steroid-induced hyperglycemia, raising the question of how to best manage hyperglycemia in patients at the EOL. Other risk factors for hyperglycemia, particularly in inpatients, include older age, prolonged steroid treatment, medical comorbidities, and a history of diabetes. 24 A survey of endocrinologists, diabetes nurse educators, palliative care doctors, and palliative care nurses found that most clinicians regularly monitor blood glucose levels in patients with steroid-induced diabetes to recognize hyperglycemia and that clinicians commonly utilize sliding scale insulin when needed to address hyperglycemia. There was no consensus on the frequency or method of monitoring. Interestingly, 36% of participants reported not having awareness of when their patients were hyperglycemic. 25
Treatment of steroid-induced hyperglycemia should follow the same approach as described above. For patients with a prognosis of months-to-years or those working towards further disease-directed therapies, it is appropriate to treat steroid-induced hyperglycemia to prevent hyperglycemia syndromes and facilitate disease-directed therapy. For patients with a prognosis of weeks-to-months, treatment of steroid-induced hyperglycemia can provide symptomatic benefit and prevent hyperglycemia syndromes. Insulin is usually the preferred agent for steroid-induced hyperglycemia. The insulin product should mimic the pharmacokinetic properties of the steroid used. For example, NPH insulin (intermediate-acting insulin) can be used for hyperglycemia caused by intermediate-acting steroids, starting with 0.1 units per kg for each 10 mg of steroid, with basal insulin considered for long-acting glucocorticoids24,26 For patients with persistent hyperglycemia, postprandial insulin may be considered and adjusted as needed to reach desired blood glucose targets.24,26 For patients with a shorter prognosis, there is likely minimal benefit to treatment of steroid-induced hyperglycemia, particularly in the absence of symptoms.
Tip 10: Use of Continuous Glucose Monitoring is Increasing Due to its Effectiveness in Promoting Glycemic Control and Preventing Hypoglycemia; More Research Is Needed to Guide ITs Use in EOL Settings
Use of Continuous Glucose Monitoring (CGM) is increasing in many settings due to evidence that it improves glycemic control for patients on insulin (in inpatient, outpatient, and long-term care settings).27–29 ADA guidelines now recommend offering CGM for all older adults on insulin therapy to prevent hypoglycemia and improve glycemic control. 9 Most studies of CGM have excluded older adults and those at the EOL, though some studies have found CGM use near EOL to be associated with a greater sense of empowerment, decreased fear of hypoglycemia, and decreased burden of blood glucose monitoring. 2
Wang and colleagues reported two cases of CGM in patients at the EOL. In one case, a patient’s spouse became distressed as blood glucose levels from her CGM device became increasingly lower near EOL, and hypoglycemic readings did not correspond with capillary blood glucose values. In the second case, the CGM sensor was removed after the transition to the palliative care ward in favor of once-daily fingerstick blood glucose checks. With the support of the inpatient diabetes team, CGM was later resumed due to family concerns about discomfort caused by the finger sticks. This patient’s family reported finding comfort in the use of the CGM during the palliative phase of care. 30
CGM may have both benefits and challenges at EOL. Reducing discomfort associated with capillary finger prick tests and availability of blood glucose values to respond to symptomatic hypo- or hyperglycemia may be beneficial. However, information made available by CGM may compel clinicians and/or care partners to act when doing so may not align with a patient’s goals or may cause harm. The availability of information may also cause distress to care partners who witness the expected gradual decline of blood glucose levels in the final hours to days of life. Additionally, even in situations when CGM may be useful, it may not be available for patients enrolled in hospice services due to logistic and reimbursement difficulties. These considerations reinforce the need for intentional discussions with patients and care partners of the potential benefits and burdens of either scenario to guide the role of CGM at EOL in patients for whom it is initiated, as well as consultation with experts in endocrinology for guidance in these scenarios. 25
Conclusion
The high incidence of diabetes in the general population ensures that palliative care and hospice clinicians will regularly take care of patients with diabetes as they near the EOL. Patients with diabetes often have years of experience managing their blood glucose levels, but their care partners may need additional information as they take over the patient’s daily medical tasks. In addition, symptomatic hyper- and hypo-glycemia, chronic diabetes complications, and side effects from diabetes medications can all contribute to symptom burden at EOL. Both patients with diabetes and their care partners need guidance in shifting the focus of diabetes care towards what is most important at the EOL. Adequate management of symptoms associated with diabetes and clear, patient-focused advice regarding diabetes management can improve the quality of EOL care for patients and their care partners.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.