
Abstract
Objective:
Women working in traditionally male-dominated environments are at higher risk for alcohol use disorders (AUDs). The male-dominated U.S. military has additional risk factors associated with problem drinking, including isolation from family and exposure to life-threatening stressors. In the 1980s, the military conformed to all U.S. states' 21-year minimum legal drinking age (MLDA), and established prevention and intervention policies for abusive drinking.
Methods:
Using a serial cross-sectional design, we explored trends in annual alcohol treatment rates among female veterans versus civilians. From the Department of Health's Treatment Episode Data Set, we extracted AUD admissions from years 1992–2003 for female veterans and civilians in four age categories. Using age-specific population figures, we calculated annual AUD treatment rates and odds ratios for female veterans versus civilians. We used time-series analyses to examine trends in annual AUD treatment for female veterans and civilians across the years examined.
Results:
In 1992, odds ratios of alcohol treatment episodes for female veterans compared to civilians ranged from 1.9 for 25–29-year-olds to 4.2 for 40–44-year-olds (all p < 0.01). Female veterans' annual alcohol treatment rates dropped substantially from 1992 to 2003, while rates for female civilians ages 25–34 dropped marginally and those for civilians ages 35–44 increased. Time-series analysis showed a statistically significant drop in rates for veterans from 1992 to 2003 and a significant difference between veterans' and civilians' rates, but demonstrated that female civilian annual treatment rates remained static from 1992 to 2003.
Conclusions:
Prior to the military's efforts to reduce underage and problem drinking, female veterans' alcohol treatment rates exceeded those of same-age civilians. However, with increasing exposure to an environment that discourages abusive drinking, female veterans' annual rates of alcohol treatment fell to below those for same-age civilians.
Introduction
Historically, women have had lower prevalence of problem drinking than men. Epidemiologic studies estimate the annual rates of alcohol use disorders (AUDs) at 26 per 1000 for abuse and 23 per thousand for dependence in women, compared to 69 and 54 per thousand, respectively, for abuse and dependence in men. 1 While genetic factors explain as much as 50% of the risk for alcohol dependence in women, environmental factors account for the remaining risk. Negative life events (such as physical or sexual victimization) and negative affective states are associated with higher incidence of problem drinking for women, 2,3 while motherhood and parenting are protective factors against problem drinking. 3
With more women entering the workforce during the late 20th century, social scientists have speculated about the impact of the workplace on women's drinking in general and specifically on problem drinking in women. Evidence from anthropologic studies, national surveys, and workplace studies suggests that work, or more broadly, work culture, influenced essentially all aspects of drinking. 4 Specifically, women employed outside the home are more vulnerable to problem drinking, particularly those who work in traditionally male occupations. 5 Historically, problem drinking among women in the military is significantly greater than among female civilians. 6 Bray and colleagues estimated that 6.3% of female military personnel engaged in heavy drinking, compared to 3.3% among civilian women in the mid 1980s. 7 Cultural and emotional factors may explain these findings. Military bases, like college campuses, have long had cultures of heavy drinking. 8 Alternatively, extreme psychological stress associated with military roles (combat, body retrieval), and separation from family and loved ones may encourage drinking as an escape mechanism. One study showed that military personnel were significantly more likely to report suffering from job stress than civilian workers. 9 Specifically, military women experience unique exposures: the pressure of performing a traditionally male job, an increased propensity to experience negative affective states (e.g., women are at higher risk for depression), and negative life events (physical, sexual, or combat-related trauma). In addition, military women are less likely to employ traditional coping strategies, such as use of social supports, in the military setting. 10
During the 1980s, the military sought to reduce the risk of later problem drinking by introducing comprehensive anti-drinking policies: raising the minimum legal drinking age (MLDA) to 21 in the United States (the military had previously no MLDA), adopting zero-tolerance policies for underage and abusive drinking, and establishing prevention and early intervention programs. We previously demonstrated that the military's efforts to transform its culture from pro-drinking to anti-drinking were associated with reduction in AUD treatment episodes for male veterans as compared to same-aged male civilians. 11 We wondered whether these changes affected female veterans similarly, particularly in light of the historically higher AUD prevalence among females in the military compared to their civilian counterparts, and given the unique factors associated with military life that may encourage problem drinking for women.
Methods
Our interest was twofold. First, we aimed to describe the change in legal under-21-year drinking exposure for female civilians and soldiers over the time period spanning changes in the military drinking culture, and including establishment and enforcement of a 21-year MLDA. Second, we wanted to examine the changes in annual female military personnel's rates of AUDs as measured by alcohol treatment episodes across this same period. Because national trends in AUD treatment may have changed during the period examined, we compared female veterans' and civilians' annual AUD treatment rates for each calendar year between 1992 and 2003. We defined the numerator as the total number of AUD treatment episodes identified in the Treatment Episode Data Set (TEDS) of the U.S. Department of Health in a calendar year for female veterans (or civilian women). We defined the denominator as the estimated number of female veterans (or civilian women) alive in the respective calendar year. We used assumptions and data sources described below.
Legal under-21-year drinking exposure
Female veteran exposure to legal drinking prior to the 21-year MLDA
The most comprehensive studies examining the natural progression from casual to problem drinking suggest that these changes occur over a period of 3–20 years, and the time from problem drinking to help-seeking is often years as well. Given this long latency between alcohol exposure and treatment seeking, we wanted to examine a period that would capture the eventual treatment-seeking event for those with exposure during military service. We recognized that an important environmental condition—namely exposure to legal under-21-year alcohol use—differed for female soldiers compared to civilians prior to the military's establishment of anti-problem drinking policies and adoption of the 21-year MLDA by state between 1982 and 1988. We hypothesized that female veterans who were younger than age 21 by 1988 when the MLDA applied to all military bases would experience fewer later alcohol treatment episodes than veterans who were at least age 21 before 1982. We used four age-group categories that would capture veterans whose military service extended through the transition period from a pro-drinking environment prior to 1982 to an anti-drinking environment and universal 21-year MLDA in 1988; we derived exposures for these groups from the age when the treatment episode occurred: age groups 25–29, 30–34, 35–39, and 40–44 years. For instance, if a veteran had a treatment episode in 1999 when she was in the 25–29-year-old age group, she would have been between 14 and 18 years old in 1988, and therefore would have 0% exposure to legal under-21-year drinking given that she experienced only the 21-year MLDA. Alternatively, if a veteran had a treatment episode in 1999 and was in the 40–44-year-old age group, she would have been between ages 23 and 27 in 1982 and would have 100% exposure to legal drinking under age 21, that is, exposure at ages 18, 19, and 20.
However, there was a period of transition during the mid-1980s spanning the establishment of military anti-alcohol policies, and coinciding with the adoption of the 21-year MLDA starting in 1982 when there was no military MLDA and ending in 1988 when the last state, South Dakota, raised its drinking age to 21 (DISCUS, 1993). To calculate exposure for veterans during the transition years between 1982 and 1988, we estimated pre-21-year MLDA exposure for each 5-year age group and for each treatment year as follows. We derived the years in which individuals from each age within each 5-year group were 18, 19, and 20 using their current age for each treatment year. We determined exposure to legal under-21 year age drinking for each single age within a 5-year age group for each state, by examining each state's MLDA during the years that individuals were aged 18, 19, and 20. We used U.S. Census state, gender, and age-group population figures, assumed each individual age to be equally distributed within each 5-year age group, and estimated overall 5-year age group exposure using the average exposure for each individual age within the 5-year group for each state and year. Because state distributions of military personnel by gender and year were not available, we used current military base population figures (male and female) for each state to estimate the relative proportion of female soldiers by state. 12 For each 5-year age group and treatment year, we derived a national military base personnel exposure to legal under age 21 drinking during the transition years 1982 through 1988 using 5-year age group exposures and weighting by relative state military base population proportions. We assumed all veterans entered the military at age 18, and therefore could have a maximum exposure of 3 years of legal drinking prior to establishment of the 21-year MLDA. We assumed all veterans spent some or all of their military time between ages 18 and 20 on U.S. bases; we did not attempt to correct for exposure to foreign drinking age laws.
Female civilian exposure to legal drinking prior to the 21-year MLDA
Because many states lowered their MLDA in the early 1970s, then raised the MLDA again in the 1980s, older female civilians in many states experienced an inverted U-shaped exposure to the 21-year MLDA. We derived civilian exposure to legal under-21-year drinking similar to our method for veterans by examining each state's MLDA during the years that individuals were aged 18, 19, and 20. However, we derived exposure by individual age, state, and year based on state MLDA laws between 1966, when 44-year-olds of 1992 were 18, and 1988 when all U.S. citizens were subject to the 21-year MLDA. For each treatment year and 5-year age group, we assumed equal distribution of individual ages within each 5-year age category. We derived national 5-year age group exposure to legal under-21-drinking by averaging exposure across each 5-year group and weighting each by U.S. Census–derived 16 state female population for each age group, state, and year.
Annual AUD treatment episode rates for female veterans and civilians by age category
AUD treatment episode data collection (numerator)
We obtained AUD treatment episode data from the U.S. Department of Health's TEDS. The TEDS is an administrative data system that provides client-level descriptive information about nationwide admissions to substance abuse treatment that have occurred since 1992. This database includes the number and characteristics of persons—including age, gender, and veteran status—admitted to public and private substance abuse treatment programs licensed through state substance abuse agencies that receive public funding. The dataset also includes information on service setting (e.g., ambulatory, inpatient, detoxification, methadone maintenance), number of prior treatments, employment and income status, social situation, insurance/payment status, psychiatric diagnoses, substances abused, route of administration, frequency of use, age at first use, and veteran status. As of 1997, when the latest available inclusion rates are known, reported admissions to TEDS facilities represented 83% of the TEDS-eligible admissions and 67% of the total known admissions. 13 TEDS does not include data on treatment programs operated by private for-profit agencies, state correctional institutions, or the Veterans Administration (VA).
From the TEDS, we extracted numbers of treatment episodes for female veterans and non-veterans who self-identified alcohol as an abused substance for the years 1992–2003. We used these figures as the numerators for our treatment rate calculations.
Five-year age category population (denominators)
To calculate annual AUD treatment episode rates, we extracted denominators (5-year age group populations) for each 5-year age category during years 1992–2003 for female veterans from the Veteran Data and Information demographics database. 14,15 We derived denominators for each civilian age group by subtracting each respective veteran age group population estimate from the U.S. Census estimates for females in each of the pertinent age group categories in each of the years examined. 16 We calculated annual treatment rates by dividing raw treatment numbers by relevant population for each year.
Statistical analysis
The study's primary outcome was the trend in annual AUD treatment rate by veteran status between 1992 and 2003. We calculated the annual treatment rate for women veterans by dividing the number of AUD treatment episodes in a given calendar year by the total number of women veterans alive in that year. We calculated the annual treatment rate for non-veterans by dividing the number of AUD treatments in a given calendar year by the total number of civilian women alive that year. For our main analysis, we fit a cross-sectional time-series regression model with a generalized least squares (GLS) estimator (Stata, version 10; College Station, TX). Using this model, we were able to model time-series separately for veterans and non-veterans treatment rates and compare the two time-series. We also calculated odds ratios and 95% confidence intervals using the standard dichotomous variable-dichotomous endpoint formula to compare trends for female veteran versus civilian alcohol treatment episodes over time. For female veterans in each age group category, we used corresponding female civilian rates in the same age group as the reference group for each year examined.
Results
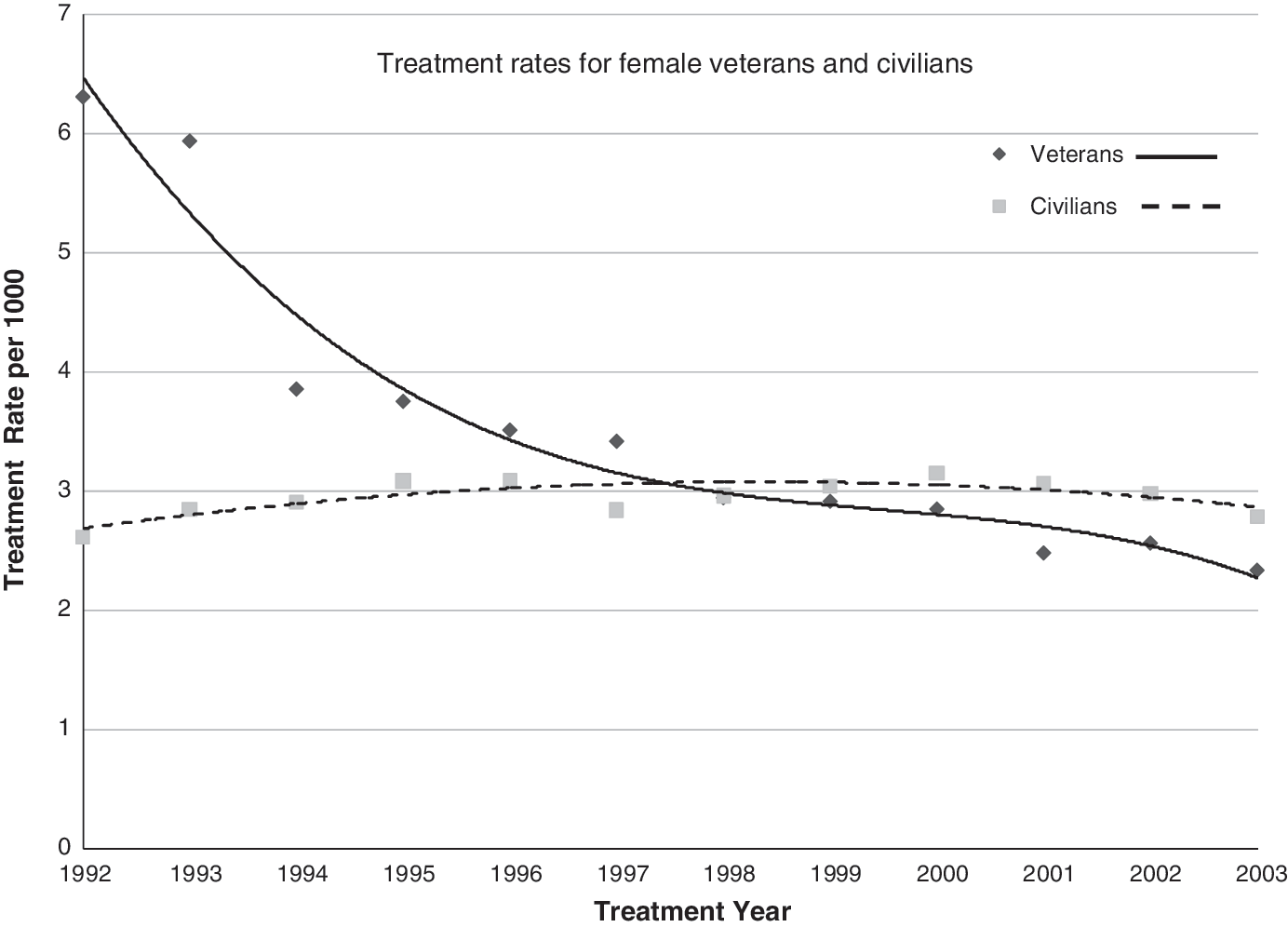
We examined 28,083 alcohol treatment episodes for veterans and 1.5 million alcohol treatment episodes for civilians that occurred between 1992 and 2003 for female patients who were between ages 25 and 44 at treatment entry. Annual AUD treatment episodes were approximately 2,340 for female veterans and 122,000 for female civilians, for whom the annual population represented between ages 25 and 44 years was approximately 756,000 female veterans and 43 million female civilians. Annual treatment episode rates were highest among female veterans aged 30–34 (6.7 episodes per thousand veterans in peak years 1992 and 1993), and lowest among female civilians aged 40–44 in year 1992, for whom rates were 1.3 episodes per thousand (Fig. 1). For all age groups, alcohol treatment rates for female veterans were double those for female civilians in 1992. By 2003, annual treatment rates for female veterans were lower than rates for civilians in all four age groups. Annual treatment rates increased by about one episode per thousand for female civilians ages 35–39 and 40–44, and decreased by about one episode per thousand for female civilians ages 25–29 and 30–34 over the years examined.

Alcohol treatment episodes for female veterans and civilians and exposure to legal underage drinking for years 1992–2003.
In 1992, the odds ratio for alcohol treatment episodes for female veterans exceeded those for female civilians for every age group, ranging from 3.5 for 40–44-year-olds to nearly 2.0 for 25–29-year-olds. However, across the years examined, odds ratios for female veterans entering treatment compared to female civilians was lower for all age groups, falling to 0.60 of civilian rates for the younger two age categories, 0.70 for 35–39-year-olds, and 0.80 for the 40–44-year-old veterans by 2003 (Fig. 2).

Odds ratios for female veterans compared to female civilians (reference group) over treatment years 1992–2003.
Female veterans' relative exposure to a pro-alcohol military culture varied by age group. Increasing exposure to legal under-21-year drinking corresponded to increasing age, and all ages had greater exposure during years prior to 1995 (Figs. 1 and 2). For the four age categories combined for treatment year 1992, approximately 99% of the military population and 46% of the civilian population had exposure to legal drinking under age 21, compared to 44% of veterans and 7% of civilians by treatment year 2003.
Time-series analysis revealed that, although veterans had higher treatment rates than civilians initially (in the early 1990s), treatment rates for veterans fell below those of civilians by 1997 (Fig. 3). This reversal of trends is significant (p < 0.01) for all age groups individually and combined. In addition, treatment rates for female veterans ages 25–44 decreased significantly between 1992 and 2003 (p < 0.001), while civilian treatment rates remained static over that time period.
Time-series analysis of treatment rates for female veterans and civilians ages 25–44 from 1992 to 2003.
Discussion
Adoption of the 21-year MLDA, implementation of policies for zero-tolerance for underage and abusive drinking, and establishment of intervention and prevention programs marked the military's desire to transform its drinking culture. These changes adopted during the 1980s were associated with fewer alcohol treatment episodes later in life for the younger female age groups effected by these policies when compared to that of older female age groups who served prior to institution of these anti-drinking policies. The decrease in alcohol treatment episodes over this period is not likely due to an overall societal trend for women's drinking, as annual alcohol treatment rates for female civilians over this same period dropped only marginally or even increased, depending on the age category. Our time-series analysis showed that female civilians' treatment rates remained static over the years examined, while veterans' treatment rates fell below and stayed below those of female civilians a decade after the military changed and enforced its drinking policies.
It is possible that selection bias affected our findings to some extent, as the military has aggressively promoted itself as a mainstream career choice for women, and indeed the military has increased its proportion of women over the past 20 years. The reversal of odds ratios for treatment episodes among female civilians and veterans over the years studied could merely be a reflection of the military's attracting a different type of woman over this time period, with potentially different drinking patterns. While this could have some impact on the findings, it alone would unlikely explain the large differences that our results show.
It is also unlikely that these findings are the result of decreased sensitivity in the detection of drinking problems in the military. Indeed, in the wake of the Tailhook scandal and other incidents that raised awareness as to the endemic hazards military women routinely face, screening for conditions ranging from military sexual trauma to substance abuse is now mandated.
It is also improbable that changes in annual alcohol treatment rates of alcohol are due to appreciable changes in the nature of women's roles in the military in regards to factors that impact drinking, such as stress and trauma. If anything, military personnel report significantly greater job-related stress than civilian workers. 9 Also, modern warfare has greatly impacted non-combat roles in the military, antiquating such prior notions as “safety in the rear.” 10
Our study has several limitations. First, this natural experiment relied on observational population data. As with any administrative database, reporting or recording of information, including veteran status, may be flawed. We cannot determine whether specific women exposed to under age 21 drinking were those represented among TEDS alcohol treatment episodes. In addition, TEDS data tracks treatment episodes rather than individual treatment; that is, an individual admitted twice in a calendar year counts as two treatment episodes. Since we were unable to distinguish between treatment episodes and unique individuals treated, we may have overestimated annual alcohol treatment rates for both civilians and veterans. To the extent that repeat admissions per individual are similar between civilians and veterans, and across veterans of different age groups, our results provide a valid estimate of relative treatment rates across groups and years. Likewise, the TEDS database does not include important variables such as socioeconomic status, family alcohol history, and co-morbid mental illness; therefore, we were unable to adjust for these personal factors that may impact the development of AUDs.
Second, treatment episodes are only a proxy for AUDs. The threshold for seeking or receiving treatment for AUDs may have increased over the years examined, thereby accounting for the observed decrease in alcohol admissions. However, there is no reason to believe the threshold for treatment of younger female veterans rose relatively more than that for civilians or older veterans, therefore leaving the reversal of annual alcohol treatment rates for veterans compared to civilians ages 25–39 years otherwise unexplained.
Third, our assumptions concerning military recruits and MLDA exposure may be incorrect. We assumed that recruits enter the military at age 18 and experienced maximum exposure to legal drinking under age 21 prior to institution of the 21-year MLDA. This assumption, while supported by U.S. Government sources, 17 may be erroneous. To the extent that average military recruitment age has not changed for the age categories and over the years examined, our analysis approximates relative exposure to the MLDA and, we believe, our “dose-response” results are valid. We also assumed alcohol use prior to military enlistment was either non-contributory or had a negligible effect on later treatment episodes. In fact, alcohol use among military personnel prior to military enlistment may confound our estimates of alcohol exposure being limited to drinking that occurred in the context of the military. Indeed, one study estimated that 75% of Naval recruits, the majority of whom were underage, had consumed alcohol in the year prior to enlistment. 18 However, to the extent that consequences of alcohol exposure are cumulative and/or additive, restricted exposure among 18–20-year-old recruits—even those exposed to alcohol prior to the military—may have ameliorative effects on later development of AUDs. Likewise, the military transitioned to the 21-year MLDA along with each state over a 6-year period between 1982 and 1988. Though we attempted to adjust for changing population exposure using current military base populations for veterans, these may inaccurately estimate relative military population by state in years past. Similarly, for both veterans and civilians, state residence at the time of treatment does not necessarily equate to that at ages 18–20. These estimates and assumptions may have either underestimated or overestimated the true exposure to legal drinking for both civilians and veterans. Since we applied this estimation procedure similarly for military personnel and civilians, and across those age groups for whom these transition years applied, we believe our results provide a valid comparison. Finally, our assumption that underage soldiers spent some or all of their service time on U.S. bases may be incorrect, and we were unable to adjust for foreign drinking age law exposure.
Fourth, changes in the general character of military recruits over the years examined may better explain our findings. Efforts to portray military service as a mainstream career choice for women may have attracted women who are simply less prone toward problem drinking. Similarly, the military's implementation of widespread screening programs for drug abuse with the 1984 Uniform Age Drinking Act 19 may have discouraged women with substance use problems from entering the military. However, military life still poses challenges unlike most mainstream careers including time away from family, potentially dangerous duty, and rigorous physical demands that may make military women more vulnerable to problem drinking than their civilian counterparts.
Finally, the relative contribution of VA treatment for AUDs among female veterans is unknown. In 1999, approximately four million of the nations' 25 million veterans were enrolled in the VA, and 82% of these received some VA care that year. 20 Since this considerable portion (about 15%) of the veteran population may have received addiction treatment services through the VA, a compensatory shift in VA alcohol treatment episodes might explain the decrease in treatment by TEDS participating facilities. However, between 1997 and 2000, concurrent with reductions in non-VA (i.e., TEDS-reporting) alcohol treatment episodes for this group, the VA experienced a 19% reduction in addiction treatment programs. This reduction in VA addiction treatment capacity suggests that veterans may have been more likely to seek addiction care outside the VA, that is, at TEDS-reporting facilities, in later years. 21 Whether or not fluctuations in VA treatment capacity significantly affected TEDS annual alcohol treatment rates over the period examined, it is unlikely that these fluctuations would affect younger veterans, who experienced a decrease in TEDS alcohol treatment episodes, differently when compared to veterans ages 40–44, who experienced a slight increase in TEDS annual alcohol treatment rates over the years examined. Similarly, any longitudinal changes in treatment capacity in TEDS-reporting facilities would have affected veterans and non-veterans alike, since veteran status would not affect access to treatment in these facilities.
While veterans' treatment episodes in VA would no doubt elevate veterans' overall treatment rates, the decrease in treatment capacity in VA over the mid to late 1990s suggests VA's relative effect on veterans' annual alcohol treatment rates would be greater in earlier years, thereby more likely underestimating the decline in total female veteran treatment episodes since the mid 1990s. If VA treatment episodes occurred in the context of static if not decreasing VA treatment capacity over the years examined, our findings—that female veterans' annual TEDS alcohol treatment episodes decreased both relative to earlier annual veterans' rates and compared to civilians' rates—are provocative.
Despite these limitations, our results suggesting an association between the military's efforts to reduce abusive and underage drinking and reduction in later alcohol treatment episodes is interesting.
Conclusions
Our findings that stricter military policies and general cultural changes around drinking were associated with reduction of alcohol treatment episodes for military women are important. These policies will impact a military population that is increasingly composed of women. Adopting similar policies that discourage underage and abusive drinking might be beneficial for other traditionally male-dominated occupations and college campuses wherein women are at higher risk for problem drinking.
Footnotes
Acknowledgments
This work was supported by the VAMC Office of Rural Health and through Dr. Wallace's VA Health Services Research and Development Advanced Career Development Award (ARDCA 04-280). The views expressed in this article do not necessarily represent the views of the Department of Veterans Affairs or of the United States government.
Disclosure Statement
Dr. Wallace has received research support from Janssen Pharmaceuticals but does not believe this constitutes a competing financial interest for this article. The other authors have no competing financial interest.