
Abstract
Aims:
To examine the effectiveness and tolerability of acute treatment with frovatriptan in women experiencing menstrual migraine (MM) vs. female migraineurs with non-MM.
Methods:
This was an open-label postmarketing surveillance study (n = 7107) conducted in Germany to assess acute treatment with frovatriptan in one to three migraine attacks. This retrospective subanalysis evaluated acute frovatriptan treatment in women who experienced ≥1 MM attack vs. those women with non-MM attacks. Effectiveness and tolerability were graded using a 4-point scale (1 = very good, 2 = good, 3 = satisfactory, 4 = poor).
Results:
Demographics were similar in MM (n = 1931) and non-MM patients (n = 2080), except that mean age (38.3 vs 45.3 years, respectively) and number of migraine attacks per month were less in the MM group than in the non-MM group (both p < 0.001). Although 98% of women reported that their previous migraines were moderate or severe, only one third in each treatment group previously used triptans. Prestudy medications were rated as good or very good for effectiveness by 20.3% and 19.2% of the MM and non-MM groups, respectively. In contrast, the effectiveness of frovatriptan was rated as very good or good by 92.7% and 90.9% of women in the MM and non-MM groups, respectively. Forty-three percent and 96% of all women rated their previous medication and frovatriptan, respectively, as having good or very good tolerability. Among women rating their previous medication as poor or satisfactory, most (94%) rated frovatriptan as very good or good.
Conclusions:
Acute frovatriptan treatment improved patient ratings of treatment effectiveness and tolerability in women with migraine associated with menses.
Introduction
Migraine is a common, disabling disorder, 1,2 yet it remains underrecognized and undertreated. 1,3,4 Some patients may not recognize that their headache is a migraine and, therefore, may not treat the attack with the most appropriate medication or may not even seek medical help. 3 For many patients, simple analgesics are often the first choice because they are easily obtained (i.e., over the counter); however, they may not be the most tolerable or effective therapeutic option for relieving migraine pain and symptoms. 3 Furthermore, some patients have more difficult to treat migraines that may be unresponsive to some medications. Prescription medications, such as triptans, that target peripheral and central serotonin (5-HT1B/1D) receptors and inhibit vasoactive neuropeptide release have become a mainstay of migraine treatment because of their good efficacy and tolerability. 5 Individuality in patient response to different triptans is relatively common, 5 –8 however, and switching to a different triptan may be a good option if a patient fails to respond to a particular triptan. 5
Women are disproportionately affected by migraine, with a migraine prevalence of 17% in women vs. 6% in men. 1 Migraine in the female population appears to be closely tied with reproductive cycling, with a substantial increase in the risk of migraine at puberty and a subsequent decline after menopause. 1 Researchers evaluating the link between migraine and the menstrual cycle have found that from 50% to 68% of women experience menstrual migraine (MM) attacks, which occur during the perimenstrual period, 9 –13 generally between day −2 and day +3 (menses = day 1, no day 0). Thus, there appears to be a strong relationship between MM and fluctuating estrogen levels, with occurrence of migraines increasing when estrogen levels are at their lowest. 14
MM is often reported as more severe 15 and of longer duration than non-MM 10,16 ; thus, MM may be more disabling than headaches at other times of the month. Additionally, many women report to their physicians that their acute medications are less effective during the perimenstrual period. To evaluate possible differences in female migraineur response to therapy based on the timing of the migraine (i.e., MM vs non-MM attacks), a subset analysis was performed using data from a large (n = 7107) prescription postmarketing survey study of frovatriptan (Frova®, Endo Pharmaceuticals Inc., Chadds Ford, PA) conducted in Germany. A previous publication details study results for the full population. 17 For the current subset analysis, the effectiveness and tolerability of acute treatment with frovatriptan 2.5 mg were compared with previous migraine therapy in women with self-reported MM or non-MM attacks.
Materials and Methods
Study design
This open-label postmarketing surveillance study of frovatriptan was conducted at multiple sites in Germany from January through June 2003. 17 Patients whose primary care physician prescribed frovatriptan for the acute treatment of migraine, as defined by the International Headache Society (IHS), 18,19 were enrolled in the postmarketing survey. A total of 7107 patients provided survey data, including baseline data on the characteristics of previous attacks and treatments, as well as data on one to three migraine attacks treated with frovatriptan 2.5 mg. A subanalysis of the original dataset was performed to evaluate the effectiveness and tolerability of frovatriptan in women with MM attacks vs. those with self-reported non-MM attacks. MM was defined through patients' self-report when they answered Yes to the question: Start of attack associated with menstruation? (migraines that occur ± 2 days of normal bleeding/menses start). This question was asked for all three attacks during the study. Women not answering this question (i.e., missing data) for all three attacks were excluded from the analysis. The MM cohort was defined as women who answered Yes to this question for ≥1 of the 3 attacks. Women with no attacks associated with menstruation were classified into the non-MM group. Because of the design of the patient questionnaire, no differentiation could be made between women with pure MM (migraines that occur only during the perimenstrual period) vs. women with menstrually related migraine (migraines that occur during menses but also at other times of the cycle). Data were evaluated within the MM subset and between women in the MM and non-MM groups.
Effectiveness and tolerability assessments
Effectiveness and tolerability of prior medication (rated by patient) and frovatriptan (rated by patient and physician) were assessed by questionnaire. Patients and physicians rated each parameter according to a 4-point scale: 1 = very good, 2 = good, 3 = satisfactory, and 4 = poor. Within-patient analyses evaluated the effectiveness or tolerability of prior treatments compared with the current acute frovatriptan treatment. For the within-patient analysis, patients were grouped into three categories: improved by ≥1 grade, unchanged, and worsened by ≥1 grade.
Statistical analysis
Descriptive statistics were used and included the number of patients, mean, SD, minimum, and maximum for continuous variables. The number and percentage of patients were also summarized for categorical variables (e.g., migraine attacks per month). Chi-square tests (categorical variables) and t tests (continuous variables) were used to compare patient demographic characteristics across the MM and non-MM groups. Intrapatient comparisons for effectiveness and tolerability of frovatriptan were performed using the McNemar test of agreement. All statistical evaluations were done using SAS/STAT version 8.02 (SAS Institute, Cary, NC).
Results
Patient disposition and demographics
Approximately 82% (5772 of 7011) of the original study population were women; of these, a total of 4011 female migraineurs were evaluated, and 1761 women were excluded because they did not provide responses for one or more of their migraine attacks. Among the remaining patients, slightly fewer women associated migraine with menses (MM group, n = 1931, 48.1%; non-MM group, n = 2080, 51.9%). Among the women with reported MM attacks, 1185 (61.4%) associated all three migraines with menses, 428 women (22.2%) associated two of three migraines with menses, and 318 women (16.5%) associated one of three migraines with menses. Overall, the demographics were similar between the MM and non-MM groups, except that women with MM attacks had a lower mean age (38.3 vs. 45.3 years) and reported fewer migraine attacks per month on average (both p < 0.001) (Table 1). Approximately one third of patients had previously used triptans in both the non-MM (37.4%, n = 777 of 2080) and the MM groups (34.4%, n = 665 of 1931).
Percentages based on actual group sample.
MM, menstrual migraine.
In the MM group, 98% (n = 1880 of 1918) of women reported headaches of moderate to severe pain intensity, 52.6% (n = 1011 of 1924) reported pulsating pain, and 72.0% (n = 1385 of 1924) reported unilateral pain. Nausea, photophobia, vomiting, and phonophobia, respectively, occurred in 91.2% (n = 1722), 73.9% (n = 1395), 55.1% (n = 1041), and 49.2% (n = 929) of 1889 women in the MM group. Migraine duration of ≤12 hours was experienced by 45.5% (n = 872 of 1917) of women; 29.8% (n = 572) and 24.7% (n = 473) experienced a duration of 12–24 hours or >24 hours, respectively. The non-MM and the MM groups showed considerable similarity for all migraine characteristics.
Effectiveness and tolerability ratings
Both the MM and non-MM groups of women reported substantial improvements in effectiveness with acute treatment with frovatriptan compared with previous therapies. The majority of women rated the effectiveness of their previous therapy as satisfactory or poor in both the MM (79.7%, n = 1494 of 1874) and non-MM (80.8%, n = 1648 of 2040) groups (Fig. 1). Conversely, 92.7% of women in the MM group (n = 1785 of 1926) and 90.9% of women in the non-MM group (n = 1884 of 2072) rated the effectiveness of acute frovatriptan as very good or good. Less than 2% of women in each group rated the effectiveness of frovatriptan as poor (MM, n = 30 of 1926; non-MM, n = 38 of 2072). As with ratings of effectiveness, both the patients with MM and those with non-MM exhibited improvements in ratings of tolerability after switching from previous therapies to frovatriptan. A minority of women in each group rated the tolerability of their previous therapy as good (MM, 37.2%, n = 673 of 1809; non-MM, 36.2%, n = 717 of 1980) or very good (MM, 6.5%, n = 117 of 1809; non-MM, 6.5%, n = 128 of 1980). In contrast, 96.4% (n = 3817 of 3958) of women in both groups rated the tolerability of frovatriptan as good (35.2%, n = 1394 of 3958) or very good (61.2%, n = 2423 of 3958) (Fig. 2).

Patient ratings on the effectiveness of previous migraine therapies and frovatriptan in women with menstrual migraine (MM) and non-MM. n = the number of women within each category.
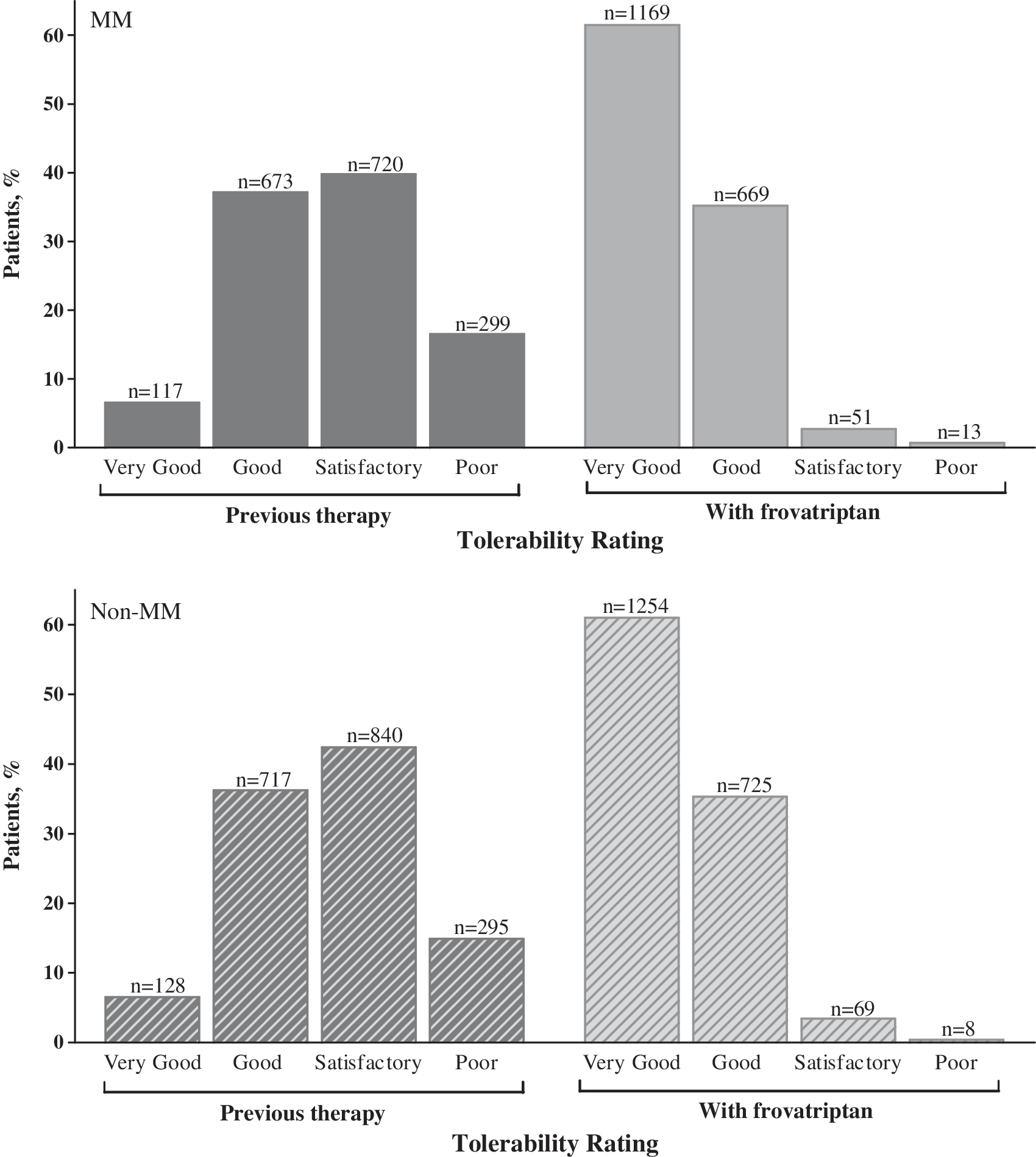
Patient ratings on the tolerability of previous migraine therapies and frovatriptan in women with menstrual migraine (MM) and non-MM. n = the number of women within each category.
Within-patient comparisons of women in the MM group confirmed that ratings of effectiveness and tolerability of frovatriptan were higher compared with ratings of previously used medications (p < 0.001 for both effectiveness and tolerability). Effectiveness and tolerability improved by ≥1 grade in 84.2% (effectiveness, n = 1573 of 1869) and 77.1% (tolerability, n = 1377 of 1786) of patients (Fig. 3). Very few patients with MM attacks reported that effectiveness (3.4%, n = 63 of 1869) or tolerability (2.1%, n = 38 of 1786) of frovatriptan worsened by ≥1 grade compared with previous therapy. Of the patients with MM who graded the effectiveness of their previous therapy as poor, 98.5% (n = 465 of 472) reported improvement while taking acute frovatriptan (very good, 54.5%, n = 257 of 472; good, 37.5%, n = 177 of 472; satisfactory, 6.6%, n = 31 of 472). Similarly, in menstrual migraineurs who had rated the effectiveness of previous therapy as satisfactory, the large majority (94.9%, n = 968 of 1020) reported improvement while taking acute frovatriptan (very good, 50.7%, n = 517 of 1020; good, 44.2%, n = 451 of 1020). Most (84.6%, n = 319 of 377) menstrual migraineurs who rated the effectiveness of their previous therapy as very good or good maintained that rating or improved (went from good to very good) with frovatriptan. In patients who had poor tolerability with their previous therapy, 98.3% (n = 292 of 297) reported satisfactory, good, or very good tolerability with acute frovatriptan treatment. Likewise, 97.4% (n = 1451 of 1489) of women with MM attacks who had tolerability ratings for previous therapy listed as satisfactory to very good maintained or improved those ratings with frovatriptan. The women with non-MM headaches reported ratings for both effectiveness and tolerability almost identical to those of women in the MM group.
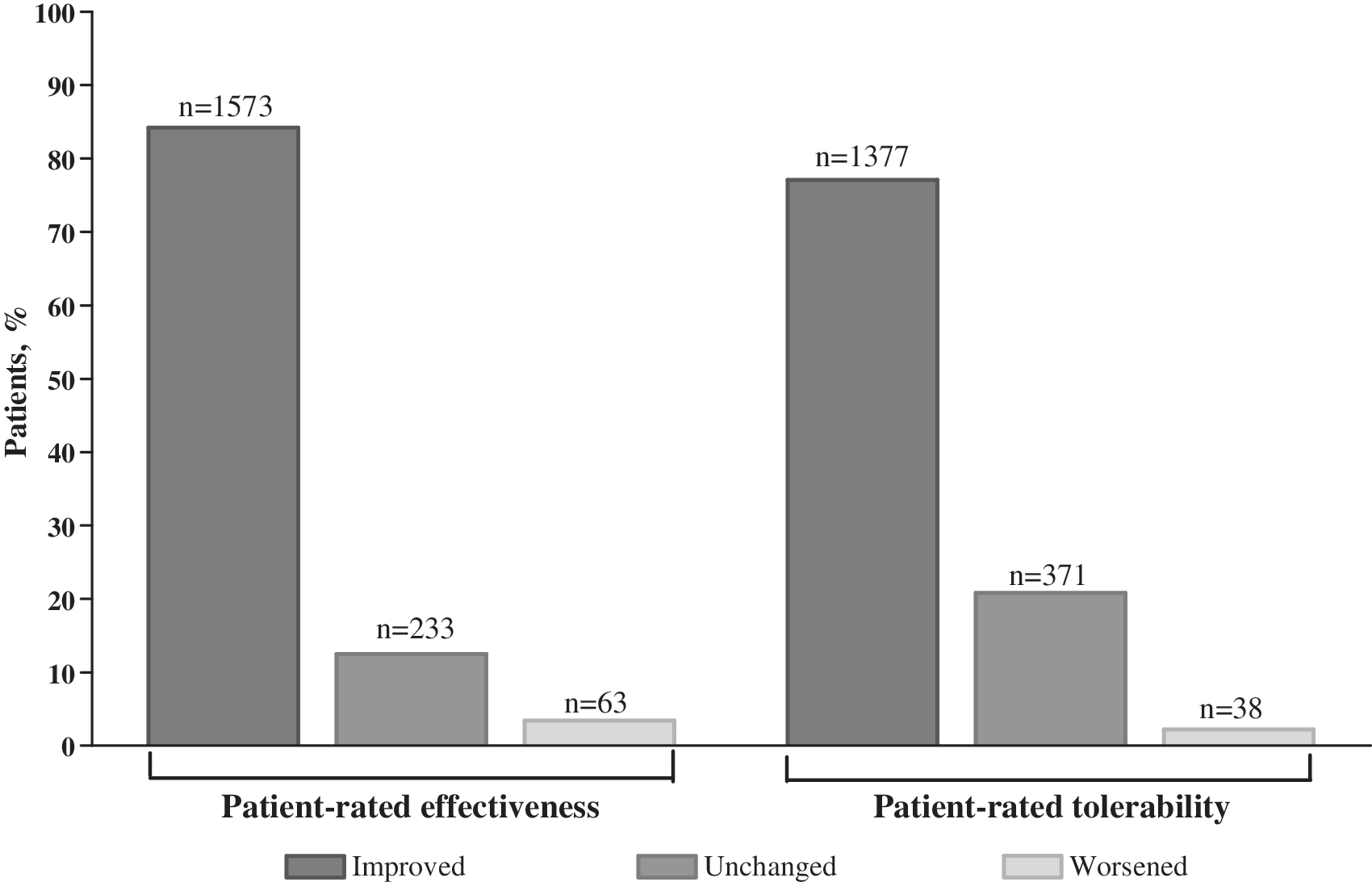
Within-patient comparisons evaluating the effectiveness and tolerability of frovatriptan therapy compared with previous therapies as rated by patients with menstrual migraine (MM). Data are categorized by those women who improved by ≥1 grade, those who remained unchanged, and those who worsened by ≥1 grade. Patients rated the effectiveness and tolerability of their previous therapy and frovatriptan using the following scale: 1 = very good, 2 = good, 3 = satisfactory, and 4 = poor. Numbers listed above the bars are the number of women within each category.
Physicians also provided positive responses on the effectiveness and tolerability of acute treatment with frovatriptan for both groups, generally corroborating patient responses (Fig. 4). For patients with MM and those with non-MM, physician ratings of effectiveness and tolerability were similar. In most cases, physicians reported the effectiveness of frovatriptan treatment as very good or good (93.3%, n = 3728 of 3994). Likewise, they reported that tolerability was very good or good in 97.4% (n = 3851 of 3953) of patients. Few physicians rated the effectiveness (1.5%, n = 61 of 3994) or tolerability (0.4%, n = 15 of 3953) of acute frovatriptan as poor.

Physician assessments of the effectiveness and tolerability of frovatriptan in the total population (menstrual migraine [MM] and non-MM combined). Numbers listed above the bars are the number of patients within each category.
In each subsequent attack, the percentage of patients treating severe migraine diminished in the MM group (Fig. 5). A similar pattern was observed in the non-MM group. Of 1931 women with MM attacks, 318 (16.5%) reported on the severity of a single treated attack, whereas 428 (22.2%) and 1185 (61.4%) women reported on attack severity at treatment of two and three migraine attacks, respectively, during the study period. By definition, all patients with non-MM reported on the severity (at time of treatment) of three attacks. Recurrence was low in both groups and declined during the three migraine attacks treated with frovatriptan, with 15.0% (MM, n = 289 of 1921) and 14.6% (non-MM, n = 301 of 2065) recurrence during the first attack, 9.9% (MM, n = 160 of 1609) and 11.1% (non-MM, n = 228 of 2055) recurrence during the second attack, and 8.4% (MM, n = 100 of 1185) and 8.6% (non-MM, n = 176 of 2052) recurrence during the third attack. Both groups of women averaged 1.3 ± 0.4 (mean ± SD) tablets of 2.5 mg frovatriptan during an attack (n = 1924 and 2074, for the MM and non-MM groups, respectively), with a range of 1.0–4.0 tablets and 0.3–6.0 tablets for the MM and non-MM groups, respectively. Most patients in both groups (92% each) chose to continue treatment with frovatriptan. As previously reported, the number (n = 55 of 7107) and percentage (0.77%) of patients with adverse reactions in the original study population were quite small; similar results were observed for women reporting MM (n = 20 of 1931, 1%).
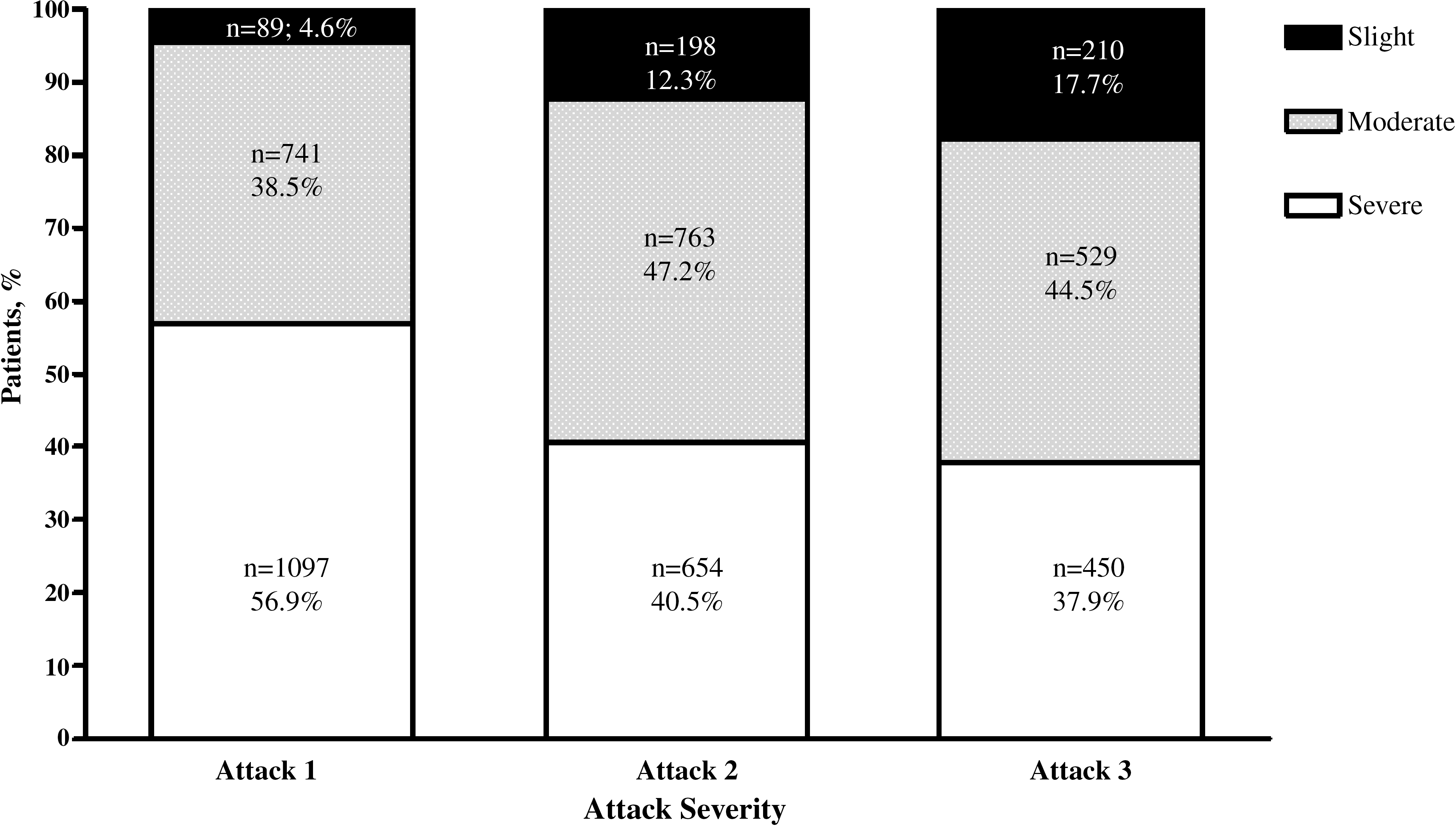
Proportion of women in the menstrual migraine population treated with frovatriptan who experienced slight, moderate, or severe pain intensity during attack one, two, and three. Number and percentage of women within each category are listed within the appropriate bars.
Discussion
This large postmarketing surveillance study describes the patient-reported ratings of previous migraine therapy compared with the current frovatriptan 2.5 mg therapy in two subsets of women, those who associated migraine with menses, and those who reported only non-MM. The majority of women in both groups (MM and non-MM) reported improved effectiveness (84.2%) and tolerability (77.1%) when switched to frovatriptan from another medication, suggesting that treatment outcomes using acute treatment with frovatriptan were not necessarily dependent on MM status. In the MM group, a limited number of women reported worsened effectiveness (3.4%) or decreased tolerability (2.1%). A total of 12.5% and 20.8% of women reported no change in effectiveness or tolerability, respectively. Similar results were seen in the non-MM group. Given the large improvements in ratings of effectiveness and tolerability, it is not surprising that >90% of women continued frovatriptan therapy.
Recurrence rates within 24 hours were low, decreasing from 15.0% to 8.4% during the course of the study in this population of female migraineurs. It is likely that the low recurrence rate was why women, on average, required only 1.3 frovatriptan tablets during an attack. The recurrence rate in this postmarketing survey is similar to the overall rate observed from several randomized, double-blind, placebo-controlled trials of acute frovatriptan therapy in which approximately 17% of patients experienced recurrence of migraine within 24 hours. 20,21 Patient satisfaction with migraine therapy is highly tied to recurrence of headache and the speed of onset of pain relief. In a previous analysis of patients who were dissatisfied with their current therapy, >70% cited pain recurrence as a problem. 22 Undeniably, pain recurrence is a common reason for patients to switch therapies. 23 Judging by the low recurrence rate, the positive response on effectiveness, and the percentage of women who remained on frovatriptan therapy, it appears that acute frovatriptan therapy is fulfilling many patients' expectations. Many women entering the study had not previously used triptans (64.1%, n = 2569 of 4011), despite 98% of them reporting moderate or severe migraine attacks. This is not necessarily surprising; undertreatment of migraine is a global problem. 1,3 It has been reported that patients believe that there are no effective treatments for migraine and often do not discuss their headaches with their physician. If they do, <10% are actually prescribed triptans for acute migraine. 3 Similar to our results, approximately one quarter of patients believed that their current treatment was effective. 3 However, the large number of patients previously using nontriptan medications may only partly explain why our study showed large improvements in reported satisfaction.
A change in treatment class (i.e., from a nontriptan to a triptan) would not fully account for the substantial improvements seen. In our study, approximately two thirds of the women switched from a nontriptan to frovatriptan, but approximately 80.3% (n = 3142 of 3914) of women rated their previous therapy's effectiveness as less than good. Even if all the nontriptan users fall into this category, approximately half of the triptan users must have rated their previous therapy as less than good. Hence, switching triptans to frovatriptan was effective for many women in this population. Although this study does not provide information about the outcome of switching from a specific triptan to frovatriptan, the data are consistent with other research that suggests that patients unable to achieve satisfactory outcomes with one triptan may benefit from switching to another. 6 –8 Additional studies are needed to address whether there are differences in the outcome of switching to frovatriptan based on the specific triptan or nontriptan therapy.
The female migraineurs in this subset analysis reported similar results to the overall study population (n = 7107). 17 Like the overall population (which was 81.2% [n = 5772 of 7107] female), the majority of women ranked previous therapy as satisfactory or poor for both effectiveness (>76%) and tolerability (>56%). Less than one quarter of women rated the effectiveness of the previous therapy as very good or good. Both the overall population and the female migraineur subpopulations (MM and non-MM groups) showed substantial improvement when switched to frovatriptan. This subanalysis excluded 1761 women who did not provide responses for all three migraine attacks treated with frovatriptan. Theoretically, if these women failed to report all three attacks because of poor effectiveness or tolerability of frovatriptan, excluding these patients could have skewed the data. However, 90% of patients in the original study (which included the 1761 women who were excluded from this subanalysis) and 92% of women in each subgroup in this subanalysis wanted to continue frovatriptan. 17 Therefore, it does not appear that exclusion of these women from the subanalysis introduced bias related to frovatriptan efficacy or tolerability.
This study has some potential limitations. First, it was a retrospective analysis of an open-label prescription postmarketing surveillance study. The findings must be interpreted with the understanding that patients and physicians were not blinded to the migraine treatment; thus, their ratings were subject to any bias they may have had regarding frovatriptan. Also, patients had to be willing to switch to a new medication, and this may have introduced selection bias.
Second, there is the potential for patient recall bias with regard to the effectiveness of their previous medications. To our knowledge, sources of bias that affect patient recall of previous therapy have not been investigated per se. In general, bias arises because patients' recall of a parameter either underestimates or overestimates the parameter compared with their response at the time of the event. For example, patients who previously experienced only satisfactory therapy might be biased, upon recall, to report previous therapy as poor. In the present study, there were 472 women in the MM group who reported the effectiveness of previous therapy as poor; of these, 92% reported frovatriptan as good or very good. We are unaware of any evidence that recall bias can produce differences of this magnitude.
We also note that potentially confounding issues, such as timing of medication, were not controlled. Because patients receive new instructions when switching medications, it is possible that they medicated differently, perhaps earlier, with frovatriptan. Such differences could affect reported effectiveness and tolerability, particularly if most women were previously treating moderate or severe attacks and switched to treating with frovatriptan when attacks were mild. However, this appears not to be the case in the current study; >80% of women treated with frovatriptan when attacks were moderate or severe, although there did appear to be a trend of earlier use comparing attacks one and three (approximately 5% and 18% of patients in attacks one and three, respectively, treated when attacks were mild).
It must also be kept in mind that this surveillance study was conducted in Germany, and the study population had ready access to healthcare under the German health system. Differences exist between healthcare systems (e.g., barbiturates are banned in Germany), and these differences could affect study generalizability. It can also be argued that the current study may not accurately characterize migraineurs who infrequently seek medical advice on migraine therapy or do not regularly use prescription medications that have been prescribed for them. 22,24 In many respects, however, our study population probably more closely mirrors the migraine population who seeks medical therapy, especially when compared with randomized controlled trials that recruit patients from migraine specialists. Viewed from this perspective, the information from this large open-label study complements the data from the randomized controlled trials because this information was gathered from a much larger patient population recruited through primary care, which may be more representative of the general population.
Finally, there is a potential limitation in how the MM subgroup was determined from the overall population. Although all women met the International Classification of Headache Disorders (ICHD) 19 criteria for migraine, they were not prospectively assessed for possible secondary diagnosis of MM because this study was performed before the second edition of the ICHD, which included criteria for MM. Migraine episodes were classified (MM or non-MM) based on patient self-report in response to the query: Start of attack associated with menstruation? (migraines that occur ± 2 days of normal bleeding/menses start). Those who answered Yes for one to three migraine attacks were placed in the MM cohort. The time frame for defining MM attacks in this study is identical to the current ICHD definition (day −2 to day +3, menses = day 1, no day 0). The definition in the present analysis may be less precise than in some other studies in which MM was confirmed as occurring regularly over multiple perimenstrual periods. 9,10,13 With our definition, it may be possible that some women were placed in the MM cohort because by chance they had a migraine attack during menses but were not true menstrual migraineurs. However, >80% of the MM group reported that two to three treated migraines were associated with menses; therefore, misclassification into the MM group is unlikely to be a significant source of error in this study. Because of the time frame imposed by our definition, however, it is possible that some patients with MM may have been misclassified as having non-MM if they experienced one to three migraine attacks (e.g., the full duration of the study) that all occurred by chance outside the perimenstrual period.
Despite these limitations, the percentage of women with MM (48.1%, n = 1931 of 4011) reported in this surveillance study is within the range reported in the literature. Dzoljic et al. 9 found that in 245 university students, 60% had menstrually associated migraine or pure MM and 21% had menstrually unchanged migraine (occurred during menses without worsening and at other times of the cycle) using the IHS criteria and MacGregor's definition of MM. 25 Granella et al. 10 used a similar definition and included patients who had from two to six migraine attacks per month (within a 6-month period) and at least one attack occurring during the perimenstrual period in 5 of the 6 months; in this population of 64 women, perimenstrual migraine attacks represented 49.7% of the total migraine attacks (n = 459 attacks). In another study, Granella et al. 13 retrospectively analyzed data from 1277 women and found that migraines occurred predominantly (50.8%, n = 649) or exclusively (9.1%, n = 116) during menses.
Some recent reports have indicated that MM attacks may be more severe and difficult to treat than non-MM attacks. 10,15,26 These observations predict that larger increases in patient satisfaction would be seen in one group vs. the other, but such a difference was not observed in the present study. Women in each group were essentially assessing frovatriptan vs. previous therapy, however, and because both groups showed large improvements, the study may not have had the sensitivity to discern differences between the MM and non-MM groups.
Conclusions
This study has scientific value because it is based on a large, diverse population of women seeking migraine-specific care from primary care physicians. More than 7000 respondents and more than 4000 women who had either MM or non-MM attacks were studied. The highly consistent responses on the effectiveness and tolerability of frovatriptan within the total population and in the two subgroups of women confirm that frovatriptan provides effective migraine pain relief and that different groups of women have very similar needs in terms of migraine therapy. In addition, although menstrual migraineurs may have a different or additional trigger (e.g., estrogen) for their headaches, their response to frovatriptan is very similar to that of women whose migraines are not triggered by menses. These postmarketing data should provide physicians with additional support when counseling female patients on the benefits of frovatriptan for both MM and non-MM.
Footnotes
Acknowledgments
This research was supported by Berlin-Chemie AG, Berlin, Germany, and the presentation was supported by Endo Pharmaceuticals, Inc., Chadds Ford, Pennsylvania.
Disclosure Statement
L.C.N. has been a part of speaker bureaus and a consultant for Endo Pharmaceuticals Inc., GlaxoSmithKline, Merck & Company Inc., and OrthoMcNeil. He has also received grants from Endo, GlaxoSmithKline, Merck & Company Inc., and OrthoMcNeil. S.H. and J.C. are full-time employees of the study sponsor, Endo Pharmaceuticals Inc. B.A.J. is a contractor for Endo Pharmaceuticals Inc.