
Abstract
Background:
An emerging literature suggests that violence against women (VAW), particularly sexual violence, may increase the risk of acquiring a sexually transmitted infection (STI) and, therefore, may be associated with cervical cancer development. The purpose of this cross-sectional analysis was to determine if women who had experienced violence had higher prevalence rates of invasive cervical cancer.
Methods:
Women aged 18–88 who joined the Kentucky Women's Health Registry (2006–2007) and completed a questionnaire were included in the sample. Multivariate logistic regression analyses were used to adjust odds ratio (OR) for confounders (e.g., age, education, current marital status, lifetime illegal drug use, and pack-years of cigarette smoking).
Results:
Of 4732 participants with no missing data on violence, cervical cancer, or demographic factors, 103 (2.1%) reported ever having cervical cancer. Adjusting for demographic factors, smoking, and illegal drug use, experiencing VAW was associated with an increased prevalence of invasive cervical cancer (adjusted OR [aOR] = 2.6, 95% CI = 1.7-3.9). This association remained significant when looking at three specific types of VAW: intimate partner violence (IPV) (aOR = 2.7, 95% CI = 1.8-4.0), adult exposure to forced sex (aOR = 2.6, 95% CI = 1.6-4.3), and child exposure to sexual abuse (aOR = 2.4, 95% CI = 1.4-4.0).
Conclusions:
Rates of cervical cancer were highest for those experiencing all three types of VAW relative to those never experiencing VAW. Because VAW is common and has gynecological health effects, asking about VAW in healthcare settings and using this information to provide tailored healthcare may improve women's health outcomes.
Introduction
Violence against women (VAW) is defined by the United Nations (UN) as “any act of gender-based violence that results in, or is likely to result in, physical, sexual, or psychological harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty, whether occurring in public or private life.” 1 Male VAW has been associated with both psychological and physical morbidity for girls and women. 2 –4 Specifically, girls exposed to sexual abuse are at increased risk of substance use, 5,6 adolescent pregnancy, 7 and subsequent sexual risk-taking behaviors. 8 Sexually abused girls are also at increased risk of forced sex during young adulthood. 9
Women who are forced into sexual activities in childhood or adulthood are also at increased risk of developing sexually transmitted infections (STI), 10 including human papillomavirus (HPV) infection. 11 Persistent high-risk HPVs are the necessary etiological agent for cervical neoplasia development 12 and occur in almost 100% of cervical cancer cases. 13 Sexual abuse, including coercive sexual experiences, has been linked to both high-risk HPV and cervical squamous intraepithelial lesions in college women 14 and among women prisoners. 15 Risk of an STI has consistently been associated with intimate partner violence (IPV) and particularly with sexual violence. 3,16 –21 Finally, IPV has been correlated with an increased risk of preinvasive cervical neoplasia in three 22 –24 of five studies. 22 –26 Only one study has explored and found an association between IPV and invasive cervical cancer. 24 This study lacked sufficient power (n = 1152) to provide an accurate estimate of the odds of cervical cancer given exposure to violence.
The present cross-sectional analysis of the Kentucky Women's Health Registry (KWHR) will add to the existing literature by addressing the association between VAW and cervical cancer in a much larger sample. This analysis will also add to the literature by comprehensively defining violence against women as our primary exposure. IPV frequently co-occurs with child and adult sexual abuse; thus, we defined VAW to include the lifetime experiences of IPV, forced sex, and child sexual abuse. We hypothesized that women who were exposed to VAW would have higher rates of cervical cancer than would women who were never exposed. Further, because cigarette smoking interacts with HPV to increase the risk of cervical neoplasia 27 and women experiencing VAW are significantly more likely to smoke, 28 we hypothesized that smokers exposed to VAW will have the highest cervical cancer rates.
Materials and Methods
Data source
We conducted a cross-sectional analysis of data available from the KWHR. The registry, begun in 2006, is a comprehensive survey open to all women, aged ≥18 years, living in Kentucky. The purpose of the registry is to better care for Kentucky women by understanding how risk and protective behavioral factors may differentially affect women's health and to give interested women the chance to participate in medical research. The goal of the survey is to enroll over 25,000 Kentucky women over the next 10 years. Women were invited to participate in the KWHR through a range of advertisement venues. KWHR brochures are available at the University of Kentucky in Lexington in all clinics providing care to women. Registry staff work across the state to recruit women through state and county health departments, county agricultural extension offices, private physicians' offices, women's professional organizations, and homemaker organizations. Women can complete the survey online (
Because this is a large convenience sample of volunteers, we do not have a refusal rate for participation. The KWHR survey data are designed as a cohort study. Women are asked to complete the survey annually. To date (May 2009), 4916 women aged ≥18 have completed at least one initial survey to enroll in the KWHR, and the number of women returning to complete the survey a second or third time is approximately 63%. The majority of women complete this survey online using a secured website; however, 12.7% completed and mailed a paper version of the survey. The KWHR was approved by the University of Kentucky Institutional Review Board. Consent and the Health Insurance Portability and Accountability Act (HIPAA) were obtained for all participants.
In this analysis, we focused on women who completed the baseline (first) survey. Of the 4916 women, 59 were excluded because of missing data on IPV, child abuse, or other forced sex, and 128 were excluded because of additionally missing data on smoking status, other substance use, or demographic data. The final number for these analyses is 4732.
Cervical cancer
Women were asked to provide details about all previous cancer diagnoses, including cervical cancer. No age at diagnosis data are available. All data are self-reported, and given consent issues, the data cannot be verified by medical records. A dichotomous variable was created to indicate a history of ever having had cervical cancer (hereafter, cervical cancer prevalence).
Violence against women
Five items were used to measure lifetime exposure to VAW. We operationally defined VAW as IPV or forced sexual experiences as an adult or during childhood. Three items were used to measure IPV: for physical IPV: Has an intimate partner hit, kicked, punched, or otherwise hurt you?; for sexual IPV: Has an intimate partner used force (like hitting, holding down, or using a weapon) to make you have sex?; for stalking: Has an intimate partner ever repeatedly followed you, spied on you, made unsolicited phone calls to your place of work or at home, damaged your property, or stalked you in any way? Although answers to these questions included experiences in the past year as well as lifetime experiences, we grouped the positive responses to indicate lifetime IPV because we do not know the age at cervical cancer development, nor do we know the age at first IPV. We created one dichotomous variable for each of the three IPV types, as well as an indicator variable for having experienced any of the three types of IPV. One item measured childhood sexual abuse: When you were a child, did any parent, stepparent, guardian or any other person make you have sex (any sex act, not just intercourse) by using force or by threatening to harm you or someone close to you? One item was included to assess if the woman had ever experienced forced sex by someone other than an intimate partner: Has anyone other than an intimate partner or anyone else used force (like hitting, holding down, or using a weapon) to make you have sex? Again, responses were dichotomized.
Women may have experienced multiple forms of VAW during their lifetime; the combined effects of violence as a child and adult may increase the risk of STIs and cervical cancer. Therefore, we created the following categories of VAW: experiencing all three forms, experiencing any two of the three forms, and experiencing any one of the three forms. The referent group for these categories was those women who never experienced VAW.
Potential confounders/effect modifiers
The KWHR includes the following sets of variables used here as either potential confounders or effect modifiers. Demographic factors included were age (continuous variable), current marital status, race/ethnicity (white non-Hispanic vs. other), education (ordinal variable ranging from no high school diploma through postgraduate education), and private health insurance coverage (current private health insurance vs. no private health insurance). Smoking was characterized as lifetime smoking status (dichotomous variable), duration of smoking (age at first and last smoking), and pack-years of smoking. Pack-years are based on years of smoking and the average number of packs of cigarette usually smoked per day. Illegal drug use was defined as ever having used cocaine, heroin, methamphetamines, or ecstasy (dichotomous variable). The survey included a question characterizing lifetime Pap smear screening frequency, but we chose not to include this variable because we do not know the screening patterns prior to cervical cancer development. Further Pap screening recommendations change after cervical cancer diagnosis and treatment.
Smoking, along with high-risk HPV, is an etiological factor in cervical cancer development. Therefore, effect modification by smoking was evaluated for the relationship between VAW exposure and cervical cancer prevalence. The following combined exposure groupings were used: (1) VAW (+) and smoking (+), (2) VAW (+) and smoking (−), (3) VAW (−) and smoking (+), compared with VAW (−) and smoking (−) as the referent group.
Statistical analysis
Chi-square tests were performed for dichotomous analyses, and t tests were used for continuous and ordinal outcomes (e.g., age, years smoked, and pack-years of smoking). Decisions about the inclusion of confounders were based on the variable being association with VAW, being known risk factors for cervical cancer, and not being in the causal pathway between VAW and cervical cancer. Given the large sample size, only associations with VAW of p < 0.01 were noted. Given the small number of cervical cancer cases, we explored additive interactions and used multivariate models to adjust for other confounders.
Results
Lifetime prevalence of VAW among those completing the KWHR was relatively high (41.1%). In this sample, 35.9% experienced IPV, 9.7% of women reported forced sex by someone other than an intimate partner during their adult life, and 8.4% experienced sexual abuse during their childhood. Further, among the 1700 women who had ever experienced IPV, 20.2% reported forced sex and 13.8% reported child sexual abuse.
Compared with women never experiencing VAW, those who had ever experienced VAW were significantly younger, had less education, and were less likely to currently have private health insurance and to be married (p < 0.01) (Table 1). Additionally, women experiencing VAW were significantly more likely to have ever had an STI, to have ever used illegal drugs, to smoke cigarettes, and to smoke more cigarettes over a longer period than those never experiencing VAW. The following factors were included as confounders in subsequent multivariate models: age, education, current marital status, lifetime illegal drug use, and pack-years of cigarette smoking. Our two indicators of socioeconomic status (SES), current health insurance and education, were correlated (coefficient = 0.292, p < 0.0001). We opted to include education level in multivariate models because educational attainment reflects lifetime status vs. current SES. We did not have a measure of SES at the time of cervical cancer development. History of having an STI was not included as a confounder because it may be in the causal pathway from VAW (particularly sexual) and cervical cancer.
Illegal drugs use includes cocaine, heroin, methamphetamines, or ecstasy.
Nonsmokers received value of 0.
Table 2 presents the multivariate logistic regression analysis estimating odds ratios (ORs) for cervical cancer and all forms of VAW combined and by three types of VAW: IPV, forced sex by nonpartner, and child sexual abuse. Two percent (n = 103) of the 4732 women included in this analysis reported ever having cervical cancer. Among the 1945 women who had ever experienced VAW, 3.5% had ever had cervical cancer, compared with 1.3% of women never experiencing VAW (aOR = 2.6, 95% CI 1.7-3.9). Cervical cancer rates were also higher for women experiencing IPV (aOR = 2.7, 95% CI 1.8-4.0), forced sex by a nonpartner (aOR = 2.6, 95% CI 1.6-4.0), and child sexual abuse (aOR = 2.4, 95% CI 1.4-4.0).
Odds ratio (aOR) adjusted for age, education, current marital status, pack-years smoking, ever used an illegal drug.
Defined to include ever experiencing stalking, physical or sexual abuse within a partnership, adult exposure to forced sex by someone other than a partner, or child exposure to sexual abuse.
60.1% IPV and forced sex by a nonpartner, 30.7% IPV and child sexual abuse, 9.2% forced sex by a nonpartner and child sexual abuse.
85.5% IPV, 8.8% child sexual abuse, and 5.7% forced sex by a nonpartner.
When summing the total number of the three possible VAW types queried (e.g., IPV, child sexual abuse, and forced sex by a nonpartner), there was a trend of increasing cervical cancer prevalence with increasing types of VAW experienced (chi-square = 7.66, p for trend = 0.007). Women who experienced all three types of VAW had the highest cervical cancer rates (aOR = 6.4, 95% CI 2.7-14.9) (Table 2).
Lifetime smoking status and VAW appear to interact to increase cervical cancer rates. Among the 980 women who had ever smoked and experienced VAW, 45 women (4.6%) had ever had cervical cancer compared with 17 women (0.9%) who never smoked or experienced VAW (aOR = 4.9, 95% CI 2.6-8.9). Among the 965 women who were never smokers but did experience VAW, 23 (20.4%) had cervical cancer (aOR = 2.7, 95% CI 1.4-5.1). Similarly, among the 834 women never experiencing VAW who were smokers, 18 (2.2%) had ever had cervical cancer (aOR = 2.3, 95% CI 1.1-4.7).
Discussion
To our knowledge, this is the first study to report an association between cervical cancer and three forms of VAW: IPV, exposure to child sexual abuse, and adult forced sex. Experiencing multiple types of VAW increased the prevalence of cervical cancer. Cigarette smoking, an acknowledged cause of cervical cancer, appears to further increase cervical cancer rates in combination with VAW. Because cervical cancer is a rare event, we needed the large sample from the KWHR (n = 4732), which has sufficient study power (95%) to detect a rate ratio of 2.0 with a cervical cancer prevalence in the population of 2.0%. We were able to measure both physical and sexual abuse and adjust for confounding factors (e.g., age, education, marital status, smoking, and illegal drug use).
Our finding that all three forms of VAW were associated with cervical cancer is consistent with the growing literature showing that sexual assaults and abuse are associated with an increased risk of an STI, including infection with human immunodeficiency virus (HIV) 29 and HPV, 30 and with an increased risk of cervical dysplasia. 15,22,24
Mechanistically, how might VAW increase the risk of cervical cancer? Figure 1 provides a conceptual model for pathways by which VAW may be associated with cervical cancer. For this analysis, we only had data on VAW, smoking, and cervical cancer; however, it is also plausible that VAW may impact cervical cancer risk through important constructs depicted in Figure 1. For example, VAW, particularly sexual violence, influences a woman's control over her choice to engage in sexual intercourse and use of contraception. Abusive partners may not be monogamous and may also refuse barrier methods of contraception, thus limiting women's ability to protect themselves from STIs, 18 including HPV. VAW may thus directly influence the risk of cervical cancer through increasing risk of acquiring and maintaining a persistent HPV infection, the necessary event for cervical cancer development. 12 A consistent literature documents that women experiencing VAW are at increased risk of acquiring an STI. 3,19,20,31 –42 VAW may influence cervical cancer risk indirectly through stress and associated immune suppression. Women experiencing VAW are well documented to have higher self-perceived stress levels and higher rates of depression and anxiety disorders. 3 Increased stress may affect cervical neoplasia risk through changes to a woman's immune surveillance. 43 –47 Immune compromised subjects are more likely to develop a range of infections, including cervical dysplasia and genital condyloma. 48 Women infected with HIV are known to be at increased risk of invasive cervical cancer. 47 Two recent studies indicate that higher stress levels increased the odds of cervical neoplasia progression 49 or being diagnosed with a higher grade lesion. 22 VAW may influence cervical cancer risk through smoking; women who have experienced VAW are significantly more likely to smoke. 28 In addition to HPV infection, cigarette smoking has been identified as an important cofactor for development of cervical cancer. 13,50 Smoking may affect cervical cancer risk by influencing early immune responses to HPV and result in persistent HPV infection. 51 Smoking and high-risk HPVs biologically interact to cause cervical cancer. 27 Our finding that women who smoke and were exposed to VAW had the highest cervical cancer rates is consistent with this observation, yet we lack biological measurement of HPV.
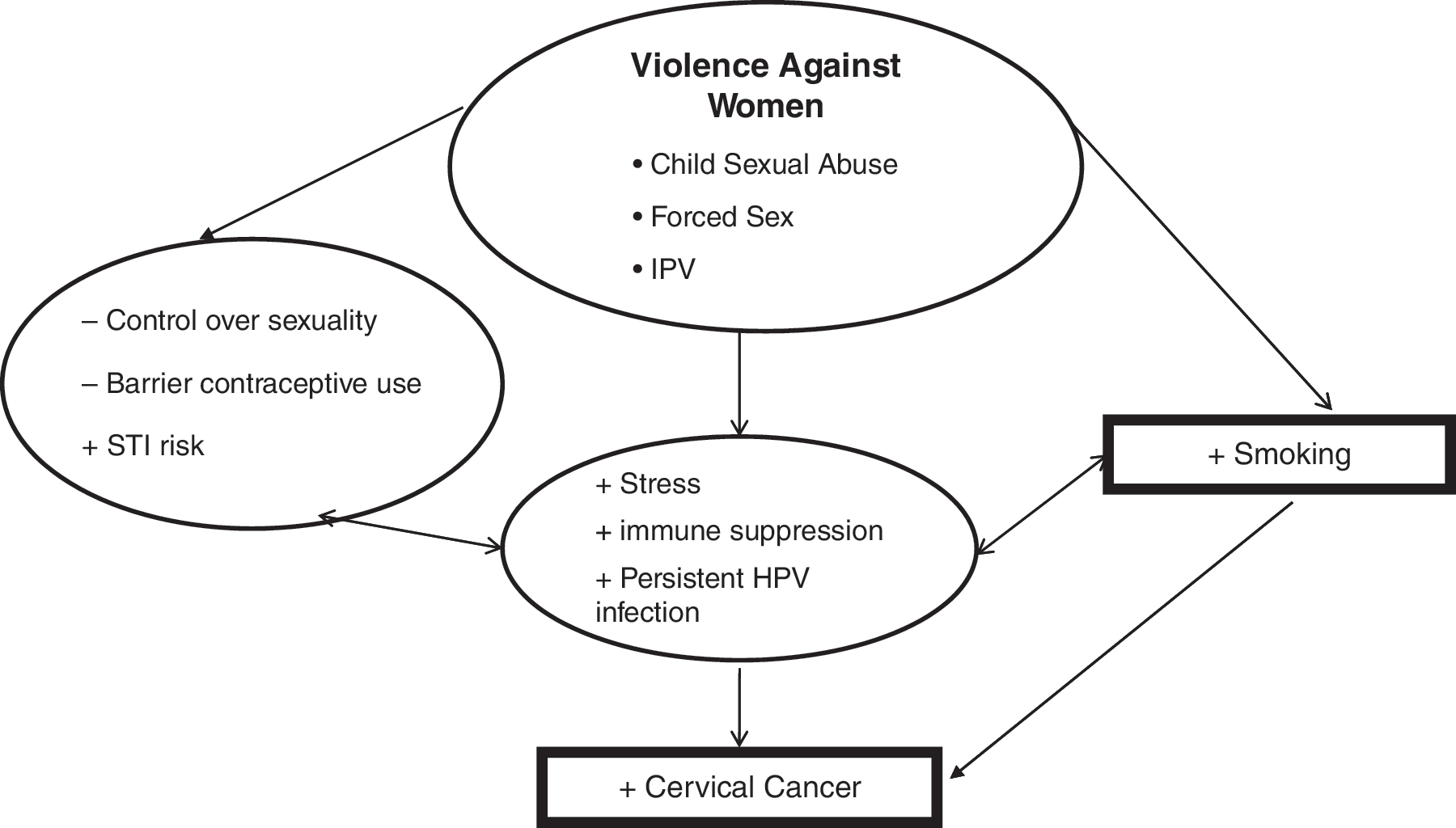
Conceptual model for VAW and cervical cancer.
Finding that VAW is associated with cervical cancer in this cross-sectional sample suggests that confirmatory results should be sought using a study design better able to address the risk of preinvasive cervical lesions. Future studies are also needed to investigate potential biological mechanisms by which violence heightens the risk for cervical cancer. Additional studies are needed to address the life course of VAW and its potential impact on cervical cancer risk. Such an understanding may inform intervention development to reduce the impact of abuse on cervical cancer risk.
There are limitations to this cross-sectional analysis that deserve mention. It is impossible to infer causality from observational data. As with most cross-sectional analyses, we do not know the timing of VAW relative to cervical cancer development because we do not have dates of violence or cancer occurrence. We can be reasonably certain that child sexual abuse occurred prior to cervical cancer. The greater uncertainty lies with the temporal sequence for IPV and cancer. The average age at first IPV is 25.7 years,
52
and the mean age at cervical cancer diagnosis was 49.8. (
Selection bias may result from the voluntary nature of the KWHR sample, such that women experiencing VAW may be less likely to participate. The rates of VAW would then be lower in this sample. To explore this possibility, we compared the lifetime rates of physical or sexual IPV based on the KWHR (24.4%) with the rate from a report by the Centers for Disease Control and Prevention's Behavioral Risk Factors Surveillance System (BRFSS) of 23.6% lifetime physical or sexual violence by a current or former intimate partner. 53 The BRFSS uses a similar approach to defining lifetime IPV, yet subjects are sampled using random digit dial telephone survey methodology. Additionally, the VAW items were included at the end of the survey, and much like the BRFSS survey, VAW was not the focus of the KWHR survey. Finding similar rates provides some evidence that selection bias may not be operational.
The women included in the KWHR are of higher SES than Kentucky women in general. To better describe how this KWHR sample differs from other population-based samples of Kentucky women, we compared the demographic profile of women completing the KWHR survey with Kentucky women who recently completed the Kentucky BRFSS telephone survey. 53 BRFSS uses a random digit dialing approach to sample household to participate in an annual phone-based survey of health behaviors. Based on 2005 BRFSS data for Kentucky women, 17.2% had no health insurance compared with 12.7% of women in the KWHR. Women in the KWHR were less likely to have ever smoked (38%) than were women completing the BRFSS (49%). However, women in the KWHR were more likely to currently be overweight (59%) than were women completing the BRFSS (55%). Because smoking is more prevalent in lower socioeconomic populations, our finding of an association between IPV and cervical cancer in a higher socioeconomic population suggests these findings may be generalized to all women in Kentucky or the United States.
How do the prevalence rates of cervical cancer compare with population-based rates of cervical cancer prevalence in Kentucky? Although Kentucky does have a Surveillance and Epidemiology End Results Registry begun in 1995, this registry has not been collecting both incidence and survival data for sufficient time to accurately calculate prevalence; therefore, we cannot compare our 2% prevalence in women participating in the KWHR with a population-based estimate for Kentucky women.
From a clinical perspective, VAW is common and does influence gynecological health. Physicians and other healthcare providers caring for women should consider asking women about violence and develop protocols to address the short-term and longer-term consequences of this violence. Efforts to address substance use, including smoking, and other risk-taking behaviors may be important interventions to reduce the risk of subsequent violence revictimization.
Footnotes
Acknowledgments
We wish to thank Mary Johnson, Dongying Zhong, Ashley McCorkle, Cady Blackey, and Sara Madison Davenport for their work on the KWHR project.
Disclosure Statement
The authors have no conflicts of interest to report.