
Abstract
Objective:
Informed decision making for preventive and screening services in primary care is receiving increased emphasis, yet the actual practice of informed decision making in clinical settings is limited. Lack of training, time, and standardized approaches to engage patients in decision making have been cited as barriers. In initiating screening mammography for women in their 40s, most organizations advise clinicians to educate women about the benefits and potential harms of screening, yet provide no practical guidelines on how to do so in clinical practice.
Methods:
We describe an ethically sound, practical model dialogue that may be used to communicate with women in their 40s about initiating screening mammography and include a discussion of the potential benefits and harms. The dialogue is based on a previously described informed decision-making framework, synthesis of evidence from the breast cancer screening and patient-physician communication literature, field testing with practicing academic and community-based general internists and recommendations by health communication experts.
Conclusions:
The dialogue may be used in office and in academic clinical settings to engage women in decision making about initiating screening mammography, to educate them about the potential benefits and harms, and may also serve as a foundation for teaching medical students and residents about patient-centered communication.
Introduction
From simple tasks such as suggesting routine blood work or recommending a screening test, to treating complicated medical conditions, primary care clinicians make daily medical management decisions for and with their patients. Recently, emphasis has been placed on engaging patients in their care and incorporating informed decision making into a clinical encounter. 1 Informed decision making is a model for clinician-patient communication that is founded in medical ethics, related to the legal concept of informed consent, reinforced by patient-physician communication research and is consistent with the Institute of Medicine recommendation for informed decision making as an important dimension of quality health care. 2 The goal of informed decision making is to foster the informed participation of patients in clinical decisions, an approach that has been shown to improve patient-oriented outcomes. 3,4
Though not universal, most patients desire to participate in informed decision making regarding their clinical care, 5 –9 yet informed decision making in the outpatient setting appears to be limited. 10 This may be due in part to lack of formal clinical training in medical schools and residencies, lack of time during time-pressured clinical encounters, patients' lack of interest or capacity to participate in the decision-making process, a concern that engaging patients in informed decision making may have untoward effects on their utilization of screening, and/or lack of practical guidelines on how to incorporate informed decision making in primary care, among others. 4,11 Decision aids aimed at educating patients about the benefits and potential harms of interventions and/or treatments have been introduced in clinical settings, 3 but their utility in real-world clinical settings is not clear. 12 Further, informed decision making is at the core of patient-centered care and is emphasized in medical student and resident education. Yet, to our knowledge, there are also no standardized methods to help medical educators teach informed decision making. Several approaches have been previously described and have reported success in learners' self-reported understanding of the importance of engaging patients in decision making. 13 –16
Despite these challenges, informed decision making is emphasized in many areas of primary care, including cancer screening. 1,4 For breast cancer screening, most recommendations now call for initiating screening mammography for women beginning at age 40, but encourage clinicians to discuss the benefits and potential harms of screening with their patients and engage them in the decision-making process. 1,17 –20 Data also suggest that women themselves want to be involved in the decision to initiate screening mammography and desire specific information prior to their first mammogram. 8 In this article, we apply a framework for informed decision making to provide an evidence-based model dialogue that may be used in office and in academic clinical settings to engage women in their 40s in decision making about initiating screening mammography, educate them about the potential benefits and harms, and may also serve as a foundation for teaching medical students and residents about patient-centered communication.
Methods
Development of the model dialogue
Our methodology for developing an idealized dialogue for communicating with women about initiating screening mammography involved several steps. First, we adopted a previously developed informed decision-making model 10,21 that outlined the following seven criteria: (1) discussion of the patient's role in decision making; (2) discussion of the clinical issue and the nature of the decision to be made; (3) discussion of the alternatives; (4) discussion of the benefits and risks of each alternative; (5) discussion of uncertainties; (6) assessment of the patient's understanding; and (7) exploration of the patient's preference. Next, we reviewed published studies, guidelines, and recommendations for best available evidence on the content-based points in the discussion. 8,18,19,22 –46 With these discussion points, we developed a model dialogue for an idealized discussion of breast cancer screening in primary care.
We pilot tested the content and feasibility of this model and talking points with academic general internists in workshops held at two national scientific meetings. We incorporated feedback from these workshops, mostly pertaining to time restrictions and feasibility of using the guide in office settings, into the next iteration of the model dialogue. We then conducted three focus groups with practicing primary care providers in Massachusetts and California. The focus groups were audio-recorded and transcribed. We analyzed the transcripts and notes from the focus groups and modified the dialogue through iterative analysis and discussion between the authors. One investigator (L.N.) also incorporated this model for teaching residents about screening mammography during attending teaching rounds. Finally, because health literacy is critical to effective cancer risk communication, 47 the model dialogue and the supplemental materials were reviewed by health communication experts at the Dana-Farber/Harvard Cancer Center.
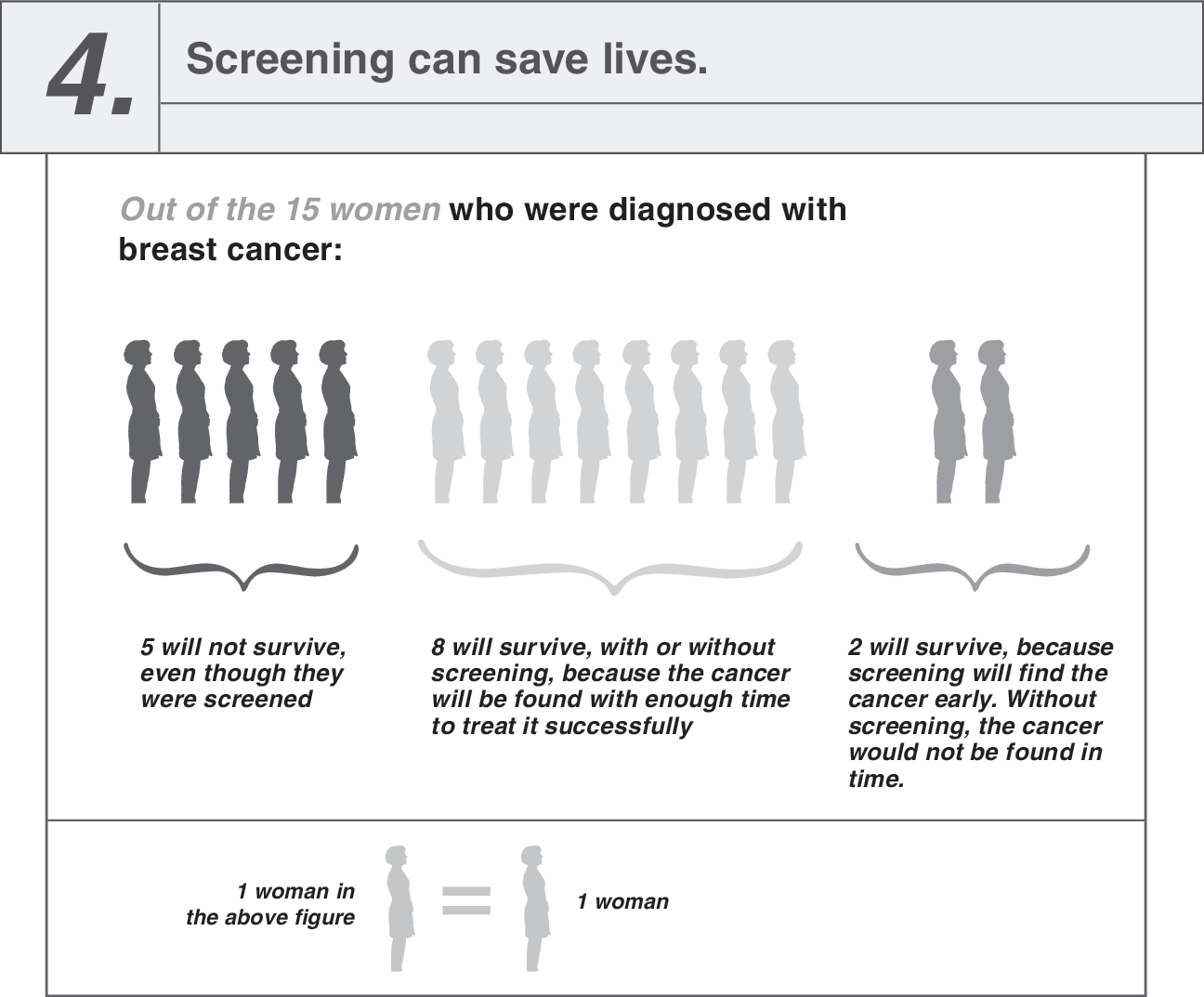
The final model dialogue presented in this article includes the following items: (1) a summary of the essential minimum dialogue, along with samples of actual wording, for any discussion of screening mammography (Table 1); (2) dialogue about specific items relating to breast cancer screening that may be included in a more thorough discussion and in response to individual patient needs (Table 2, which also provides references intended to serve as a resource for the clinicians, but not serve as an exhaustive review of the literature); and (3) visual materials that may be used in clinical settings to assist in the discussion of breast cancer risk factors (Table 3), the risks of developing and dying of breast cancer in relation to other causes (Fig. 1) and the benefits and limitations of screening mammography (Fig. 2).
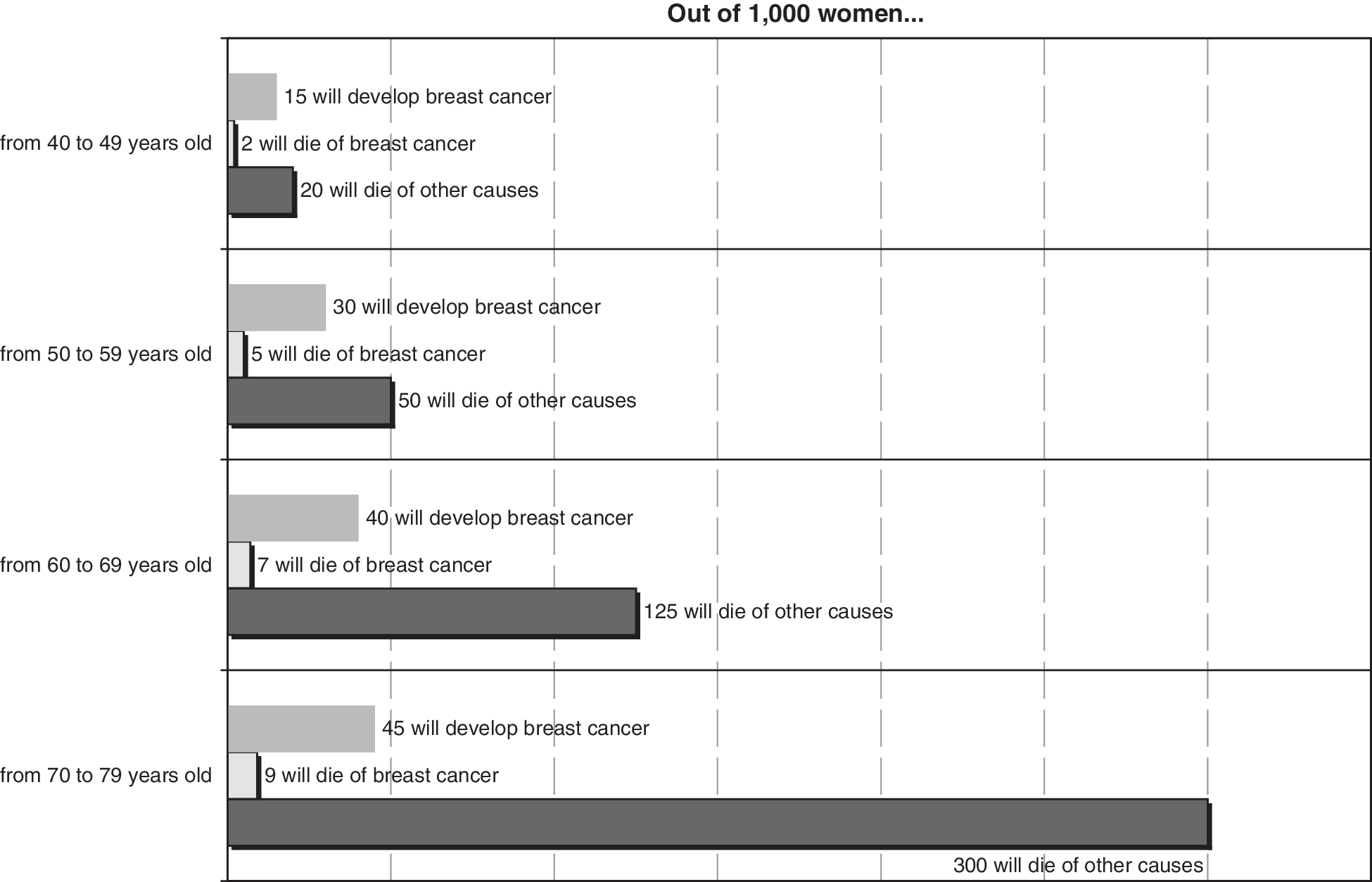
This figure is based on previously published estimates (NEJM 2003;348:1672–1680), derived from Feuer and Wun (NCI, 1999) for breast cancer rates and death from breast cancer, and from Anderson and DeTurk (National Center for Health Statistics, 2002) for the rates of death from any cause.

This figure is based on prior data from Elmore et al. (NEJM 1998;338:1089–1096) and estimates previously reported by Fletcher (NEJM 2003;348:1672-1680), derived from the Surveillance, Epidemiology, and End Results program (SEER Cancer Statistics Review, 1997; 2002). All estimates are based on women beginning annual screening at age 40.


Results
Putting it into practice: the clinical vignette
Ms. Daniels is a 40-year-old female in good health who presents for her annual examination. She has no personal or family history of breast cancer. She has had regular clinical breast examinations but has never had a mammogram. She tries to perform breast self-examinations but admits to frequently forgetting. She approaches you (her primary care clinician) to discuss breast cancer screening and to address her questions. She has been hearing and reading different opinions about the value of breast cancer screening tests. She wants you to clarify the information and help her figure out what to do.
Discussing the patient's role
The initial element of informed decision making is critical in establishing how the patient will participate in the decision-making process. It is important to note that for personal, cultural, or other reasons, not all patients wish to engage in decision making and prefer a more passive role. 7 It is not appropriate, therefore, to make assumptions regarding the patient's wishes to take part in decision making, nor to force a role where the patient is declining participation. Other patients may be hesitant to become involved and may need an explicit invitation to participate in decision making. It is always appropriate for the clinician to explore the patient's preferences regarding participation in decision making and offer an opportunity for a participatory role. Table 1 includes a suggested dialogue that may be used by the clinician to assess the patient's desired role in the discussion about initiating screening mammography.
Discussing the nature of the decision
Once the patient's role in the decision-making process has been established, the clinician should outline the issue to be addressed, advising the patient of the major factors the clinician and the patient should consider when making their decision. This information is critical in preparing the patient to be an informed participant in decision making. Ascertaining the patient's baseline level of knowledge or familiarity with the issue at hand can greatly facilitate this discussion and enhance time efficiency, as well as guide the subsequent content-oriented parts of informed decision making. 48 For suggested dialogue on how a discussion of the decision may be approached with the patient, see Table 1.
Discussing the alternatives
The next component of informed decision making is the discussion of the alternatives. Like other elements of informed decision making, this is motivated by the critical role that adequate information plays in fostering patient autonomy and eliciting genuine preferences. 49 The clinician should discuss all reasonable alternatives with the patient, but should avoid introducing an exhaustive list of possible alternatives. Because of the common observation that the extent of discussion desired by patients varies substantially between in dividuals, we recommend that providers briefly introduce the concept of alternatives (Table 1) and then apply a patient-centered approach to elaborating on specific needs and/or questions. This entails the use of question prompts to determine which specific information will be most salient for the individual (Table 2). It is important to note that while breast cancer risk assessment is presented in the optional information on Table 2, all patients need to have a thorough review of their past medical and surgical history, prior medications, as well as social and family histories taken, irrespective of their interest in participating in an informed discussion about breast cancer screening.
Discussing the potential benefits, harms, and uncertainties
As in the discussion of the alternatives, the discussion of the benefits, harms, and uncertainties has the potential to become quite time-consuming for the clinician and overwhelming for the patient. Nevertheless, it is critical that the informed patient has an understanding of each and that they are presented in a balanced manner. We recommend that the clinician introduce this concept (Table 1) and then allow the patient to drive the content and extent of the discussion (Table 2).
A discussion about the potential benefits, harms, and uncertainties requires an introduction of numerical concepts and information which is often challenging. Prior research has shown that qualitative descriptions, such as “this is very unlikely” may be used but caution should be applied as perceptions of such terms may differ. 50 Quantitative statements such as “there is only about a 5% chance of this” may be more accurate, yet are often difficult to understand; visual aids may be of use. 51,52 In Table 3, we have provided an overview of the risk factors associated with developing breast cancer using qualitative descriptions. To provide a visual guide to patients during clinical encounters, Figure 1 may be used to assist in the discussion of the absolute risks of developing and dying of breast cancer compared with the risk of dying of other causes. Figure 2 may be a useful adjunct to discuss the numerical benefits and potential harms of annual screening by women beginning at age 40, including the probability of follow-up testing after screening and the likelihood of screening mammography in finding breast cancer and saving lives.
An additional aspect of information that may be included in this discussion relates to the logistics about the procedure itself, such as when the results will be available and how they will be contacted, about the pain or discomfort that women experience during a mammogram, and about the costs of the mammogram. 8 Anticipating and addressing these concerns allow for a more patient-centered interaction. We have included these items in Table 2.
Assessment of the patient's understanding
Because the ultimate goal of this discussion is to enhance the patient's informed involvement in their care, assessing the patient's understanding is crucial. This is an opportunity for the clinician to encourage the patient to seek clarification and ask questions. Similar to discussing the patient's role in decision making, some patients need an explicit invitation to ask for further explanation or to inquire about concerns of particular relevance to them. The clinician should pay careful attention to non-verbal cues throughout the discussion and pause for clarification if the patient appears confused. Occasionally, the clinician may want to explore the patient's understanding in more depth, for example, by asking the patient to restate what they have just heard. This approach is most applicable when the decision is particularly weighty or complex or when the clinician is uncertain that the patient understands. This “teach-back” approach is supported by the health literacy literature. 53,54 For the suggested dialogue, see Table 2.
Exploration of the patient's preference
Patients should have an opportunity to express their preference for screening as they do for medical treatment. Providing the patient such an opportunity can also open the door to questions, many of which may prove crucial to the patient attempting to formulate an informed opinion on the decision at hand. If the patient disagrees with a recommendation or cannot reach a decision, this is acceptable as long as the clinician has relayed adequate information, made a clear professional recommendation, and established that the patient understands the information. The patient must also be assured that expressing indecision or disagreement will not lead to reproach or abandonment by the clinician. Some clinicians may worry that inquiring into patient preferences may inadvertently discourage acceptance of screening, but should be reassured by evidence that women generally value screening and do not alter their screening uptake following disclosure of information. 55,56 Providers are encouraged to document patient decisions in the medical record to avoid future questions about care and to follow up on the decisions at a later time. Suggested dialogue for this discussion is presented in Table 2.
Conclusions
Informed decision making for preventive and screening services in primary care is increasingly promoted and is consistent with the Institute of Medicine recommendations for patient-centered quality health care. 2 We have presented a model dialogue for a discussion of initiating screening mammography with women in their 40s that is grounded in the ethical model of informed decision-making framework, reflects basic precepts of patient-centered communication, is evidence-based, has been vetted by practicing clinicians, and is consistent with principles of effective health communication. This model may be used in clinical settings and may also be used to teach residents and medical students about patient-centered communication breast cancer screening.
This model is the first attempt to develop an evidence- and theory-based approach to educating women in their 40s about the benefits and potential harms of screening mammography. The data presented in this tool is based on women aged 40–49 and are only applicable to women in this age group.
Further, we acknowledge that we have not formally evaluated the impact of this approach on decision quality. Nevertheless, we feel that the constructs imbedded in the approach, the inclusion of informational items desired by women, and the qualitative vetting by practicing clinicians add validity to the approach. Since there are no existing theory- or evidence-based practical approaches to educating women about the benefits and potential harms of screening mammography and engaging them in decision making, our approach is an important step forward. Further, the approach we have outlined is primed for empiric testing in clinical practice and may also be the beginning of development of a formal interactive computerized decision aid that may be used prior to or during an office visit. It may also be incorporated into a booklet that women could be asked to read prior to a discussion with a clinician. Alternatively, the dialogue may be part of an educational outreach by a nurse or a health educator rather than a physician. Application and testing of this guide in various formats and different settings may help practicing and future clinicians provide women with ethically optimal participation in their care, thereby fostering the goal of improving patient satisfaction and clinical outcomes.
Footnotes
Acknowledgments
We thank our colleagues, particularly Drs. Suzanne Fletcher, Antoinette Peters, and Richard Frankel, who gave us feedback on the concept for this article and the dialogue, and also provided insightful review of earlier drafts. These include the researchers and clinicians who attended our sessions at the Society of General Internal Medicine meetings, and focus groups with members of the Division of General Internal Medicine at Stanford University and practicing internists at Harvard Vanguard Medical Associates (Wellesley, MA). We also appreciate the technical assistance provided by the Health Communication Core at the Dana-Farber/Harvard Cancer Center.
Disclosure Statement
No competing financial interests exist.