
Abstract
Objective:
Caffeine has relevance for women's health and pregnancy, including significant associations with spontaneous abortion and low birth weight. According to scientific data, pregnant women and women of reproductive age should be advised to limit their caffeine consumption. This article reviews the implications of caffeine for women's psychological and physical health, and presents data on obstetrician-gynecologists' (ob-gyns) knowledge and practices pertaining to caffeine.
Methods:
Ob-gyns (N = 386) who are members of the American College of Obstetricians and Gynecologists' Collaborative Ambulatory Research Network responded to a 21-item survey about caffeine.
Results:
Although most knew that caffeine is passed through breast milk, only 24.8% were aware that caffeine metabolism significantly slows as pregnancy progresses. Many respondents were not aware of the caffeine content of commonly used products, such as espresso and Diet Coke,® with 14.3% and 57.8% indicating amounts within an accurate range, respectively. Furthermore, ob-gyns did not take into account large differences in caffeine content across different caffeinated beverages with most recommending one to two servings of coffee or tea or soft drinks per day. There was substantial inconsistency in what was considered to be “high levels” of maternal caffeine consumption, with only 31.6% providing a response. When asked to indicate the risk that high levels of caffeine have on various pregnancy outcomes, responses were not consistent with scientific data. For example, respondents overestimated the relative risk of stillbirths and underestimated the relative risk of spontaneous abortion. There was great variability in assessment and advice practices pertaining to caffeine. More than half advise their pregnant patients to consume caffeine under certain circumstances, most commonly to alleviate headache and caffeine withdrawal.
Conclusions:
The data suggest that ob-gyns could benefit from information about caffeine and its relevance to their clinical practice. The development of clinical practice guidelines for caffeine may prove to be useful.
Introduction
Caffeine (1,3,7-
Sources: Juliano LM and Griffiths RR: Caffeine. In Substance Abuse: A Comprehensive Textbook, Fourth Edition. Lowinson JH, Ruiz P, Millman RB, Langrod JG Baltimore: Lippincott Williams & Wilkins; 2005. McCusker RR, Fuehrlein B, Goldberger BA, Gold MS, Cone EJ: (2006a) Caffeine content of decaffeinated coffee. J Anal Toxicol. 2006;30(8):611. McCusker RR, Goldberger BA, and Cone EJ: Caffeine content of specialty coffees. J Anal Toxicol. 2003;27(7):520. Caffeine values for all brand name products were obtained directly from product labels, or the manufacturer's website or customer service department. SBK, Starbucks.
Caffeine has important clinical implications in the context of women's emotional and physical health as well as pregnancy outcomes. Physicians and particularly obstetrician-gynecologists (ob-gyns), due to their expanding role as primary care providers, 3 may benefit by having background knowledge about caffeine and its clinical implications. However, little is known about ob-gyn's general knowledge about caffeine, assessment of caffeine use, and recommendations given to patients.
Clinical implications of caffeine
Caffeine may affect individuals seeking medical care, and women in particular, in a variety of clinically significant ways. Caffeine produces various CNS and peripheral nervous system effects, primarily via antagonism of A2A and A1 adenosine receptors. 4 It produces positive subjective effects (e.g., happiness, alertness) at low to moderate doses (e.g., <200 mg) and negative subjective effects (e.g., jitteriness) at higher doses (e.g., >200 mg). 5 The potential for caffeine to produce insomnia 6 and anxiety 7 is well documented, and both of these problems occur at much higher rates in women. 8,9 There are also a number of physiological effects of caffeine that may pertain to patient care, including increased blood pressure, gastric acid secretions, colonic activity, urine volume, calcium excretion, and increased levels of adrenocorticotropic hormone (ACTH), insulin, and cortisol. 5 Heavy caffeine use (>300 mg per day) also has been shown to be associated with shorter menses and shorter menstrual cycles. 10
The average half-life of caffeine is 4–6 h; however, there is as much as a 10-fold difference in metabolism across individuals, 11 with metabolism slowed by oral contraceptives 12 and hastened by cigarette smoking. 13 Furthermore, caffeine metabolism is slower during the luteal phase relative to the follicular phase of the menstrual cycle. 10 Due to hormonal influences, caffeine metabolism slows during the second and third trimesters of pregnancy, 14 which can lead to elevated caffeine levels in women who maintain their usual pre-pregnancy intake of caffeine. Elevated levels of caffeine (as low as 250 mg, according to the DSM-IV-TR) can produce caffeine intoxication symptoms (e.g., heart arrhythmias, nervousness) and other physical and psychological consequences, 15 as well as allow for greater fetal exposure to caffeine. Caffeine metabolism is very slow among fetuses and neonates (i.e., 80–100 h half-life) due to immature liver systems, which don't fully develop until around 6–8 months of age. 16
The potential for caffeine to produce physical dependence is well-documented even at relatively low daily doses (e.g., 100 mg per day). 17 This could have important clinical implications, especially for pregnant women who may abruptly stop using caffeine due to medical advice, health concerns, nausea, or requirements of medical tests (e.g., 3-h glucose challenge test). In fact, in one study of pregnant women, 54% of those who ceased caffeine use reported withdrawal symptoms, and 26% of those with withdrawal symptoms reported that these symptoms significantly interfered with their daily functioning. 18 Symptoms of caffeine withdrawal (e.g., headache, fatigue, difficulty concentrating, mood disturbances, and flu-like symptoms 17 ) could be misattributed to other causes, including pregnancy symptoms. Furthermore, caffeine abstinence has been identified as a significant cause of post-operative headaches 19 and has been documented in neonates after exposure to high doses of caffeine in utero. 20,21 The International Classification of Diseases (ICD-10) recognizes a caffeine substance dependence syndrome, which comprises a cluster of symptoms indicative of problematic use of a drug. 22 Individuals meeting criteria for substance dependence on caffeine, including pregnant women, have been identified. 18,23
It is also important for health care providers to recognize that caffeine can interact with commonly prescribed medications (e.g., benzodiazepines, cimetidine) 12 and exacerbate certain medical conditions (e.g., urinary incontinence, anxiety). 24 It is used therapeutically as a respiratory stimulant in neonates 25 and as an analgesic adjuvant (e.g., Fioricet, Excedrin). 26,27 Interestingly, epidemiological studies have identified a potential protective effect of caffeine and/or coffee consumption in the risk of developing Parkinson's disease, liver disease, and Type II diabetes. 28 –30 There is no conclusive evidence that caffeine negatively affects bone density in postmenopausal women 31,32 or fibrocystic breast disease, 33 –35 or increases breast cancer risk. 36
Caffeine and pregnancy
There has been a substantial amount of research on caffeine consumption and pregnancy outcomes. Caffeine readily crosses the placental barrier and is distributed to all fetal tissues, including the CNS, 14 allowing for the fetus to be exposed to caffeine at levels similar to the mother's. A recent large scale study and a meta-analysis of previous studies suggest that maternal caffeine use increases the rate of spontaneous abortion in a roughly dose-dependent fashion. 37,38 Associations between high caffeine use and decreased fecundity and reduced fetal growth have also been observed, 39,40 including a recent study that showed that reduced fetal growth was associated with consumption of as little as one to two cups of coffee per day. 41 It has been suggested that individual differences in the CYP1A2 gene, which is involved in caffeine metabolism, may interact with caffeine exposure in influencing the risk of pregnancy loss and other negative pregnancy outcomes. 42,43 The most consistent generality to emerge is that, when caffeine is associated with negative pregnancy outcomes, it is typically among women who consume high doses of caffeine. 40
Caffeine consumption recommendations
Comprehensive scientific reviews of research on caffeine and pregnancy have concluded that reproductive aged women should consume no more than 300 mg caffeine per day. 39,40 In line with such recommendations, governmental agencies in North America and Europe have made statements regarding safe consumption levels during pregnancy. Health Canada 44 and the American Dietetic Association 45 advises that pregnant women consume no more than 300 mg caffeine per day, while the Food Standards Agency of the United Kingdom 46 recently lowered their recommended upper limit to 200 mg per day for pregnant women. Presently, neither the American Medical Association nor the American College of Obstetricians and Gynecologists (ACOG) has put forth guidelines for caffeine consumption in pregnant women.
Physicians' knowledge and advice about caffeine
No previous studies have examined ob-gyns' knowledge and assessment practices pertaining to caffeine despite the fact that most women consume caffeine, caffeine can have important clinical implications for patients, and scientific reviews have concluded that reproductive-aged women should limit consumption to 300 mg of caffeine per day or less. 39 In fact there has been only one published report pertaining to physician's recommendations pertaining to caffeine, which was conducted over two decades ago and consisted of one question. 47 In this survey, medical specialists from two geographical regions were asked to check medical conditions for which they think patients should be advised to reduce or eliminate caffeine use. The most common conditions for which reduction or cessation of caffeine was advised were palpitations, arrhythmias, anxiety and insomnia. Furthermore among a sub-sample of 38 ob-gyns who were surveyed, 79% and 68% recommended caffeine reduction or cessation for fibrocystic disease and pregnancy, respectively.
This report describes the first comprehensive survey to examine knowledge and beliefs about caffeine among ob-gyns as well as their assessment and advice practices pertaining to caffeine use in pregnant and non-pregnant women.
Methods
Participants
A total of 785 Fellows of the ACOG were invited to participate in a cross-sectional survey study that asked about their beliefs and knowledge of caffeine's effects and their assessment and advice to pregnant and non-pregnant patients concerning caffeine use. Participants were all members of ACOG's Collaborative Ambulatory Research Network (CARN), a group of ACOG Fellows who agree to participate in four to six surveys every 12 months. CARN members are a representative sample (by age, gender, and geographic location) of the ACOG membership, of which over 90% of ob-gyns in the United States are members. Half of CARN was randomly selected for this survey sample. The first mailing was sent in June 2007, and second and third mailings were sent to non-responders between July and August 2007.
Survey questions
All questions were developed for this study due to the lack of previous survey studies on the topic.
Demographics and personal caffeine consumption
Demographic questions included gender, age, practice status (practicing/retired), practice focus (e.g., obstetrics, gynecology, maternal fetal medicine), and geographical location of practice. To assess whether personal consumption was related to practice patterns as has been shown in previous research, 48 ob-gyns were asked to report their typical consumption of caffeinated beverages (average weekly number of servings of coffee, tea, soft drinks, or other, and the typical serving size).
Caffeine knowledge
Ob-gyns were asked to estimate the number of milligrams of caffeine in the following caffeinated beverages: an 8-oz cup of coffee, a shot of espresso, a 12-oz can of Diet Coke®, and an 8-oz cup of black tea, and were asked the number of servings of caffeinated beverages that are safe for pregnant women to consume. They were asked whether caffeine is passed through breast milk (true/false). They were asked whether the rate of caffeine metabolism stays the same or changes during the menstrual cycle and whether caffeine metabolism becomes faster, slower, or stays the same throughout pregnancy. Ob-gyns were asked what they considered to be “high levels of maternal caffeine consumption (in mg)” and to rate the degree to which high levels of caffeine consumption increases the risk of various birth complications on a scale from 0 (no increased risk) to 10 (substantial increased risk) and to indicate what they considered to be “high levels of maternal caffeine consumption” (in mg/day). Physicians gave separate ratings for each of the following pregnancy outcomes: overall health of fetus, low birth weight, shorter gestational age, spontaneous abortion, congenital abnormalities, nausea, stillbirths, or long-term health of the child. Ob-gyns were asked whether they consider caffeine to be a drug of clinical dependence and to indicate the minimum amount of caffeine consumption per day that can lead to withdrawal symptoms if someone abruptly stops using caffeine.
Caffeine assessment and advice
Ob-gyns were asked about the following: if and when they discuss caffeine use, methods they use to assess caffeine consumption, caffeinated products they routinely ask about, how frequently they initiate a conversation about caffeine use, what advice they usually give their pregnant patients, and if they ever advise their pregnant patients to consume caffeine. Finally, they indicated which of their non-pregnant patients (adolescent patients/patients of childbearing age/perimenopausal patients/postmenopausal patients) they ask about caffeine consumption.
Statistical analysis
Analyses were conducted using SPSS 15.0 (SPSS Inc., Chicago, IL) with alpha set at p < 0.05. For the analysis of assessment practices relating to pregnancy, only physicians who were currently practicing (n = 379) and treating (n = 332) pregnant patients were included. Due to large variability in response rates across questions, raw numbers are presented with percentages for added clarity.
Results
Demographics
A total of 386 ob-gyns returned the survey, a response rate of 49.1%. A comparison of responders and non-responders indicated no differences in age or gender. The sample was predominantly white (62.7%) with an average age of 48.6 (SD + 10.1) years, which is representative of the fellows of ACOG. The majority of respondents practice general obstetrics and gynecology (78.9%). Just under half (40.5%) also provide primary care to their adolescent, women of child-bearing age, or post menopausal patients.
No meaningful differences were observed based on age, gender, or other demographic variables, and thus all data is reported for the sample as a whole.
Personal use of caffeine
Of the 83.9% (n = 324) who provided information about their caffeine consumption, 90.1% (n = 292) reported consuming caffeine on a weekly basis with an estimated mean of 1188.2 mg/week (SD = 1046.3) ranging from 68 to 6016 mg/week.
Knowledge about caffeine
When asked to estimate the amount of caffeine in milligrams contained in common caffeinated beverages, responses were considered correct if they were within a wide range of possible values for each type of beverage. As shown in Table 2, respondents largely over estimated the amount of caffeine in a serving of espresso with only 14.3% (18/126) providing a value in the accepted range 24 (i.e., 60–95 mg). Accurate estimates for a serving of coffee (i.e., 71–280 mg), tea (i.e., 40–120 mg), and Diet Coke® (i.e., 22–69 mg) were provided by 66.70% (92/138), 63.90% (85/133), and 57.80% (78/135) of respondents, respectively.
When asked to report what was considered to be “high levels of maternal caffeine consumption,” 15.8% (61/386) wrote in that they did not know and 52.6% (203/386) left the question blank. Of the 31.6% (122/386) that did provide an answer, the mean response was 242.2 mg (SD = 215.7), with a median of 200 mg. Only 13.2% (51/386) of all participants and 41.8% (51/122) of those who provided an answer indicated 300 mg or above.
When asked to rate the effect of high maternal caffeine consumption on various pregnancy outcomes, low birth weight had the highest mean response (greatest increase risk; M = 4.5, SD = 2.5) and congenital abnormalities had the lowest mean response (least increased risk; M = 1.9, SD = 2.1; Fig. 1). The mean response for spontaneous abortion was 3.62 (SD = 2.88). Low birth weight was rated significantly higher than spontaneous abortion (t = 5.28, p < 0.001).
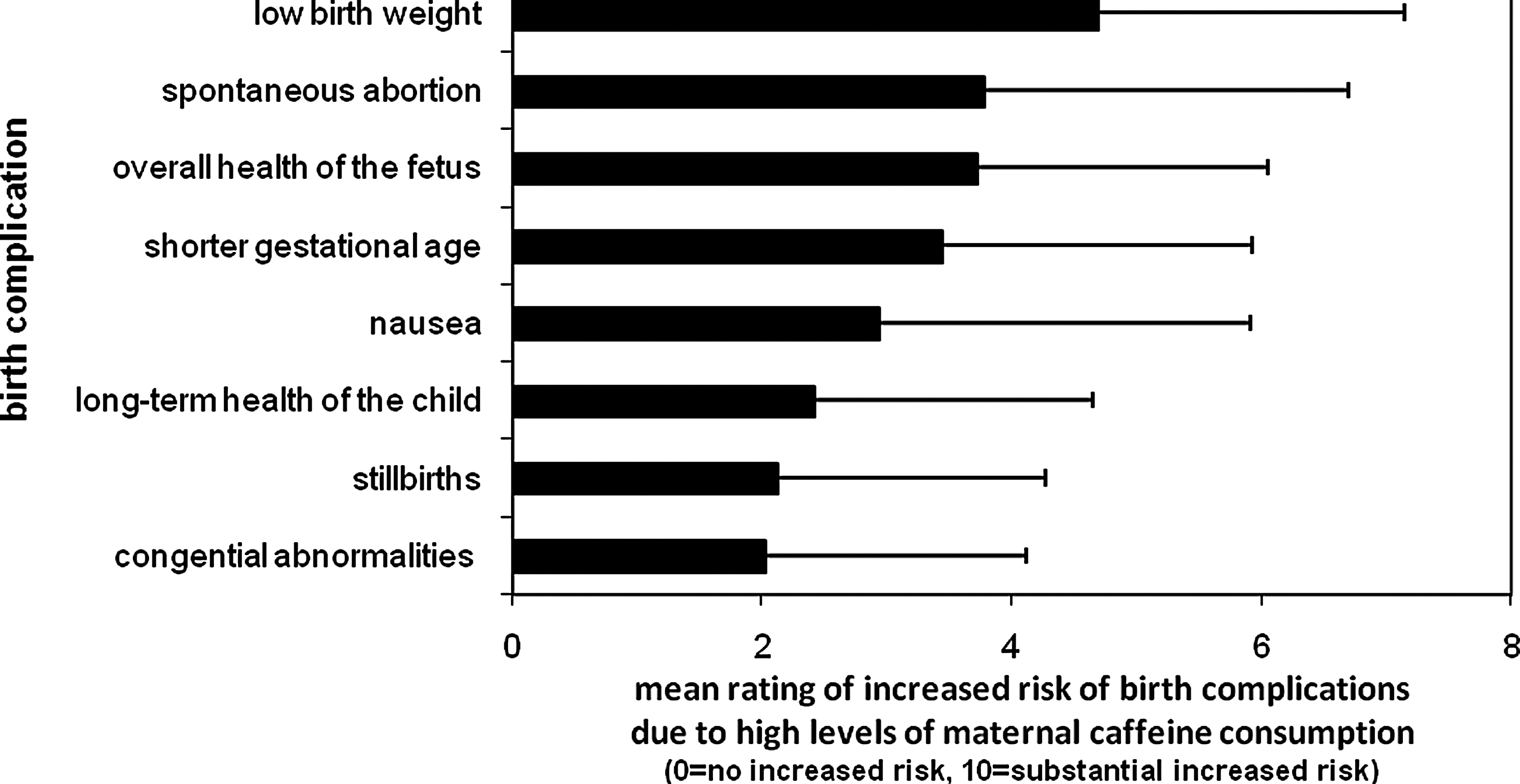
Ob-gyns' rating of the impact that high caffeine use has on birth complications.
As shown in Table 2, 96.0% (313/326) of those who provided an answer correctly indicated that caffeine can be passed through breast milk. However, only 24.8% (77/310) indicated that the metabolism of caffeine slows as women progress through pregnancy, with the majority indicating that the rate of metabolism becomes faster (39.7%, 123/310) or stays the same (35.5%, 110/310). Furthermore, only 46.3% (143/309) indicated that caffeine metabolism changes during different stages of the menstrual cycle.
Only 34.2% (132/386) provided an estimate for the minimum daily amount of caffeine consumption that will lead to withdrawal symptoms when someone abruptly stops using caffeine, the mean response was 197.01 (SD = 209.49), though there was great variability in responses. Nearly half of all respondents (49.2%, 65/132) incorrectly overestimated the amount that can cause physical dependence.
Almost three-fourths of respondents (73%, 265/365) consider caffeine to be a drug of clinical dependence. Only 5.4% (21/386) did not respond to this question.
Assessment of caffeine use
Notably, 58.2% (188/323) reported that they always discuss caffeine consumption with their pregnant patients and 31.3% (101/323) never do. Ten and a half percent (34/323) reported discussing caffeine under certain patient circumstances, with the following conditions indicated by respondents: osteoporosis, irregular heartbeat, insomnia, diabetes, hypertension, poor weight gain, fetal arrhythmia, vascular disease, headaches, breast pain, and palpitations.
When asked when ob-gyns discuss caffeine consumption with their pregnant patients, most participants indicated doing so at patients' first visit (64%, 218/386) or when the pregnant patient brings up the topic of caffeine consumption (45.9%, 177/386). Twenty-five percent (97/386) discussed caffeine consumption when discussing other drug use (e.g., alcohol, nicotine), and 18.4% (71/386) indicated that they discuss caffeine consumption with their pregnant patients when a “pregnant patient is complaining of what seem to be caffeine-related effects” with the following types of effects reported: headache, palpitations, breast tenderness, and difficulty sleeping.
When asked how often ob-gyns initiate a conversation about caffeine consumption with their pregnant patients, 24.0% (78/325) always do, 20.0% (65/325) often do, 26.2% (85/325) sometimes do, and 23.1% (75/325) rarely do. Caffeine consumption is most often assessed via a routine question asked by the ob-gyn or a member of his/her staff (40.4%, 156/386), followed by assessment using questions on a form (20.2%, 78/386). One-third (30.8%, 119/386) indicated that they had no formal routine method. Most ob-gyns ask about caffeine consumed from coffee (73.7%, 241/327), soft drinks (71.8%, 234/326), and tea (62.0%, 202/326) but fewer ask about energy drinks (38%, 124/326), foods (29.4%, 96/326), medications (21.2%, 69/326), and energy aids (19.3%, 63/326). However, 13.2% (43/326) indicated that they do not ask about specific sources of caffeine.
The majority of respondents (64.5%, 238/369) reported that they do not assess caffeine use in their non-pregnant patients. Around one quarter assess caffeine use in adolescents, women of child bearing age, perimenopausal, and postmenopausal women (20.3%, 75/369; 28.7%, 106/369; 26%, 96/369; and 25.2%, 93/369, respectively).
Caffeine consumption advice
Most respondents reported that it is safe for pregnant women to consume either one or two servings of coffee or soft drinks or tea per day. To evaluate how consistent their recommendations were across different products in terms of caffeine exposure, all responses were converted to milligrams amounts, and the differences among the various products (coffee–soft drinks, coffee–tea, tea–soft drinks) were computed for each respondent. We chose a very liberal cutoff of a 100-mg or less difference to be considered to be a consistent recommendation. Only 10.5% (29/277) of ob-gyns were consistent across coffee and tea, and 11.0% (31/282) across coffee and soft drinks. However, 98.5% (271/275) were consistent across tea and soft drinks.
Most ob-gyns indicated that they did not know what they considered to be a “healthy daily intake” of caffeine for non-pregnant women (64.8%, 250/386) or left it blank (10.6%, 41/386). Of those who responded (24.6%, 95/386), the mean amount reported was 199.3mg (SD = 153.1) and responses ranged from 0 to 1000 mg, with 87.4% (83/95) of responders or 21.5% (83/386) of all participants reporting an amount 300 mg or below.
Participants were asked what advice they usually give their patients about caffeine, one quarter (25.4%, 82/323) of ob-gyns tell their patients that research about caffeine's effect in pregnant women is largely inconclusive. Still, 31% (82/266) wrote in a response that indicated that they tell their pregnant patients to limit caffeine consumption to one drink/glass/serving, 20% (53/266) recommend one to two servings per day, and 18% (48/266) recommend two servings per day. Only 2% (5/266) wrote in trimester specific advice for caffeine use. Only 11.3% (37/326) of respondents advise their patients that “it is best to stop all caffeine consumption during pregnancy.”
Most participants indicated if they advise their patients to consume caffeine (84.5%, 326/386). More than half of the respondents (61.7%, 201/326) advise some patients to consume caffeine during pregnancy for the following reasons: alleviate headaches (51.8%, 169/326), relieve caffeine withdrawal symptoms (32.8%, 107/326), improve mood (2.8%, 9/326), other (4.0%, 13/326; e.g., fatigue, constipation, low blood pressure). Thirty-eight percent of respondents (125/326) indicated that they never advise their pregnant patients to consume caffeine.
Discussion
Caffeine is a widely used drug that has many clinically relevant physiological and psychological effects, some of which are specifically related to women's health and pregnancy outcomes. This is the first study to examine ob-gyn's knowledge and practices pertaining to patients' use of caffeine.
Ob-gyn's knowledge about caffeine
It appears that many ob-gyns are not aware of the caffeine content of commonly used beverages. As shown in Table 2, more than a third of respondents did not provide values within a wide range of possible values for coffee, tea, and soft drinks; with a tendency to overestimate the caffeine content of soft drinks and underestimate the caffeine content of coffee and tea. More than 85% of respondents either significantly overestimated or underestimated the caffeine content of espresso.
When ob-gyns were asked to define “high levels” of caffeine consumption there was great variability in their responses and 13.2% of all respondents indicated 300 mg or above. However, it is interesting to note that more than two-thirds did not answer the question or wrote that they did not know. Together, the wide variability, inaccuracy, and low response rate suggest that physicians need guidance and information about acceptable levels of caffeine use for pregnant women. Scientific reviews have concluded that pregnant women should consume no more than 300 mg of caffeine per day, 45,46 while some recent studies suggest that no more than 200 mg may be a more appropriate cut off.
While the actual risk of caffeine causing adverse pregnancy outcomes is a complicated and often discrepant body of literature, our data suggests that perhaps ob-gyns are overestimating the relative risk of stillbirths and underestimating the relative risk of spontaneous abortion. Empirical evidence is inconclusive about caffeine's effect on many adverse pregnancy outcomes, however, research supports that spontaneous abortion and low birth weight are associated with caffeine consumption. 37,38,41,49 –51 For example, a recent study found as little as two cups of coffee per day is associated with an increased risk of spontaneous abortion, 37 and one to two cups of coffee per day is associated with low birth weight. 41 The ACOG has produced a Practice Bulletin on the Management of Recurrent Early Pregnancy Loss for ob-gyns that states that caffeine and other drugs “may act in a dose-dependent fashion or synergistically to increase the rate of sporadic pregnancy loss,” but is not associated with recurrent pregnancy loss. 52
Although most respondents knew that caffeine is passed through breast milk, fewer than one-fourth knew that caffeine metabolism slows during pregnancy, and nearly 40% incorrectly answered that caffeine metabolism increases during pregnancy. Because caffeine remains in the body longer during this period of slower metabolism, the physiological and psychological effects of caffeine are likely to be exacerbated, particularly for women in their final months of pregnancy.
A substantial amount of research supports that caffeine is a drug of physical dependence, 17 meaning that its cessation will produce withdrawal symptoms. About three-fourths of ob-gyns indicated that they consider caffeine to be a drug of clinical dependence. However, “clinical dependence” was not operationalized, and some may have taken this to mean physical dependence rather than a cluster of symptoms indicative of problematic drug use. Nevertheless, features of clinical dependence (e.g., use despite harm, unsuccessful efforts to reduce consumption, tolerance) have been noted among caffeine consumers across various studies. 18,23,53 In one recent study, a sample of pregnant women meeting criteria for substance dependence on caffeine was identified, 18 and a caffeine dependence diagnosis predicted greater use of caffeine during pregnancy despite being advised by their ob-gyn to eliminate caffeine.
Ob-gyns appeared to overestimate the amount of caffeine exposure that is necessary to become physically dependent, and thus experience withdrawal symptoms upon acute abstinence, with the mean response being about twice as much caffeine as research has shown is necessary to produce physical dependence. This along with the fact that over two-thirds of the respondents failed to respond, suggests that caffeine withdrawal is poorly understood by ob-gyns. It is important that health care providers be aware that if a patient abruptly stops consuming even relatively small amounts of caffeine (i.e., 100 mg per day), as some pregnant women are likely to do, 18 they may experience caffeine withdrawal symptoms such as headache, fatigue, difficulty concentrating, mood disturbances and flu-like symptoms. 17 Thus, it is recommended that when patients complain of such symptoms physicians assess caffeine use and recent consumption patterns. Patients who would like to cease their caffeine use should be advised to gradually reduce their caffeine consumption to reduce the severity of withdrawal symptoms. There is no empirical data available to suggest a specific time-frame for reduction, but some have suggested that reducing consumption by 10–25% every few days or so may be effective. Additional guidelines for reducing or eliminating caffeine can be found elsewhere. 5
Assessment of caffeine use
Compared with other commonly used recreational drugs, ob-gyns discuss consumption of caffeine, with their pregnant patients less often. In our sample, 58% of ob-gyns discuss caffeine, where other studies have reported that 97% discuss alcohol 54 and 98% discuss tobacco. 55 There was little consistency in the methods, frequency, and timing of the assessment of caffeine among ob-gyns. It is possible that ob-gyns do not believe that caffeine is an important topic to discuss and/or it could be a result of the lack of practice guidelines pertaining to caffeine. It is also possible that it is due to difficulty interpreting often conflicting research findings pertaining to caffeine associated health risks. Lastly, the amount of time necessary to accurately assess caffeine exposure may present another barrier.
When assessing caffeine use, most ob-gyns reported that they ask about coffee, soft drinks, and tea; however, only 30% ask about caffeine intake from food and 21% ask about medications. A recent study estimated that 80.6% of pregnant women consume caffeine from multiple sources with 36.7% obtaining caffeine from all non-coffee sources. 37 It is important to note that food and medications can be a significant source of caffeine as shown in Table 1.
Some, though a minority, of our respondents discuss caffeine use under specific patient circumstances including insomnia, diabetes, hypertension, poor weight gain, fetal arrhythmia, vascular disease, headaches, breast pain, and palpitations and/or assess for caffeine use when pregnant patients complain of what seem to be caffeine-related effects. Due to caffeine's well-established effects on sleep and anxiety, 6,7 ob-gyns should assess caffeine consumption whenever patients complain of sleep disruption or anxiety-related symptoms. Women presenting with urinary incontinence may benefit from advice to reduce or cease caffeine use. 56 Caffeine use should also be assessed in patients presenting with hypertension as it has been shown that caffeine can raise blood pressure by 5–15 Hg systolic and 5–10 Hg diastolic in healthy adults. 39 Symptoms of caffeine excess/intoxication and caffeine withdrawal have symptoms that overlap with many other health conditions, including some pregnancy symptoms and ob-gyns should keep these in mind as potential differential diagnoses. For example, caffeine excess/intoxication should be considered in differential diagnoses of conditions such as medication/drug induced side effects (e.g., akathisia), substance withdrawal (e.g., benzodiazepines), hyperthyroidism, anxiety, mania, insomnia, and pheochromocytoma. Caffeine withdrawal can mimic medication-induced side effects, migraine and other headache disorders, viral illness, dehydration, withdrawal from other drugs, and pregnancy symptoms.
Advice
Many ob-gyns in our study advise patients to limit caffeine consumption to one or two servings of coffee or tea or soft drinks per day. Thus, it does not appear that physicians are taking into account the wide differences in caffeine content across different products when providing advice to their patients. For example, the amount of caffeine in two servings of coffee (roughly 266 mg) is about three times as much as the amount of caffeine in two servings of soft drinks (roughly 80 mg). Knowledge of the various sources of caffeine and variability across products should help physicians provide consistent advice to their patients.
Thirty two percent of respondents reported that they would never advise their pregnant patients to consume caffeine, while 50.8% of ob-gyns reported that they sometimes advise their patients to consume caffeine. Reasons provided included consumption to alleviate headache, withdrawal symptoms, or mood. Indeed caffeine typically alleviates caffeine withdrawal symptoms including headache and poor mood in about 30–60 min. 17 There is evidence that caffeine increases the effectiveness of analgesic medications in the treatment of headache with more modest therapeutic effects when given. 26
Study limitations
As this was the first study of its kind, replication and psychometric evaluation of the questionnaire is warranted. Furthermore, the data collected is limited by self-report and potential retrospective biases. This sample of ob-gyns reported using less caffeine than the typical American adult caffeine consumer (i.e., 170 mg vs. 280 mg per day). 2 It is possible that individuals who chose to complete this survey were more sensitive to issues pertaining to caffeine and thus may use less caffeine than the general population. It is also possible that our crude measurement of caffeine consumption underestimated use, or respondents underreported their use. At least one study has found that self-reported caffeine consumption has questionable validity. 57 Furthermore, some of the open ended questions had very low response rates. However, the low response rates appeared to be question specific and not a function of the location in the survey, which may suggest a lack of knowledge rather than lack of desire to complete the survey. The response rate for the survey was 49.1%, which is consistent with typical response rates for the CARN group. There were no differences on any demographic variable between those that returned the survey and the CARN group at large. Furthermore, previous analyses have been done to assess whether responses from CARN members are different from responses from ACOG members in general, 58 and have concluded that there are few, if any, differences between samples.
Conclusions
Although it is acknowledged that additional research is needed to clarify limits of caffeine consumption during pregnancy, major health reviews have suggested that pregnant women or women trying to conceive should limit their caffeine consumption to no more than 300 mg per day. It is acknowledged that physicians have limited time with patients and that other issues may take priority over routine assessment of caffeine consumption. At the very least, it is important for health care providers to be aware of the clinically relevant effects that caffeine has on physical and psychological health and to consider these effects when treating patients. Furthermore, as obstetricians and gynecologists continue to provide an expanding range of care to women, their knowledge and awareness of caffeine's general effects on health and psychological well-being is becoming even more significant to their practice.
Our study confirms that physicians frequently counsel patients to reduce or eliminate caffeine use during pregnancy. Among those who reported providing recommendations, their advice is in line with current research recommendations, that pregnant women limit their caffeine consumption to ≤300 mg per day (i.e., many said they advise limiting use to one or two servings of coffee or tea or soft drinks per day). However, there was great variability in what was considered to be “high levels” or “safe levels” of caffeine use for pregnant women and the data suggests that many simply do not know an appropriate limit of caffeine for pregnant women. Ob-gyns in our survey were unaware of the amount of caffeine in various products, and they tended to limit their assessment of caffeine exposure to caffeinated beverages. They were also largely unaware that caffeine metabolism significantly slows as pregnancy progresses as well as changes across the menstrual cycle, or that as little as 100 mg per day of caffeine can result in withdrawal symptoms upon acute abstinence.
Future research should be aimed at education and assessment of physicians' knowledge about caffeine and its clinical implications for patients. We hope that this article serves to increase knowledge of caffeine and its clinically relevant pharmacological effects and recommend the development of practice guidelines for ob-gyns and other health care providers.
Footnotes
Acknowledgments
This study was supported by the Maternal and Child Health Bureau, Health Resources and Services Administration, Department of Health and Human Services (grant R60-MC-05674).
Disclosure Statement
The authors have no conflicts of interest to report.