
Abstract
Bisphosphonates are first-line treatment for postmenopausal osteoporosis and women with low bone mass and risk factors for fracture. These agents are often perceived as having equivalent effectiveness and safety and are even used interchangeably by some practitioners. Research suggests, however, that differences between them are meaningful to the patient and clinician. Data from randomized controlled trials and observational database studies have demonstrated variations between bisphosphonates in the scope of fracture protection, such as vertebral and nonvertebral, as well as the speed of onset of this antifracture effect. It has been proposed that unique properties of each compound related to their mechanisms of action could explain, at least in part, differences observed in clinical outcomes. Although the bisphosphonates share a similar core structure, they also contain two side chains or groups, R1 and R2, attached to the central carbon atom. All bisphosphonates approved by the FDA for postmenopausal osteoporosis contain a hydroxyl side group at position R1, increasing their binding to bone and distinguishing them from earlier bisphosphonates not approved for this clinical use. Differences in the physicochemical and biological properties of the approved bisphosphonates are due to differences in the R2 side group. The presence of nitrogen and its orientation within the R2 side chain can influence each bisphosphonate's overall potency. For the physician to optimally determine the bisphosphonate that best suits an individual patient, it is important that they are aware of the differences between them.
Introduction
Osteoporosis is a major and growing health problem. It is estimated that approximately 50% of all women and 25% of all men over the age of 50 years will have an osteoporosis-related fracture in their remaining lifetime. 1 The incidence of hip fractures, in particular, is expected to increase worldwide from 1.7 million in 1990 to 6.3 million by the year 2050. 2 Notably, one in five women sustaining a vertebral fracture will sustain another fracture within 1 year, 3 20% of those with a hip fracture die within 1 year, 4 and wrist fractures, although often not considered osteoporotic fractures, can signal possible osteoporosis, particularly for women in their mid-50s. 5 It is, therefore, important that this disease is treated with a safe and effective therapy. In addition, it is well known that patients are at different levels of fracture risk, so determining the optimum therapy for each patient is crucial.
Bisphosphonates have been used in the treatment of medical conditions since the 1960s, and they have become the treatment of choice for various bone diseases, including Paget's disease of bone, metastatic bone disease, hypercalcemia of malignancy, and osteoporosis. Bisphosphonates are currently a first-line treatment for postmenopausal osteoporosis, and many perceive all bisphosphonates to be the same. However, some studies suggest that differences do exist among them. Data from clinical trials and observational database analyses have demonstrated variations in the scope and onset of fracture protection among the various bisphosphonates, particularly with regard to the prevention of nonvertebral fractures. As more is learned about the mode of action of each bisphosphonate, it has been proposed that clinical differences may be explained, at least in part, by differences in the particular bisphosphonate's properties associated with its mechanism of action. Differences among the bisphosphonates, which are related to fundamental differences in structure, affect how these agents work and where they are distributed throughout the skeleton. It is important that the physician be aware of the relevance of the differences among the available agents.
Evidence for Bisphosphonate Use in Postmenopausal Osteoporosis
The first commercially available bisphosphonate for the treatment of osteoporosis was etidronate, which was approved over 30 years ago. Although it is still in use worldwide, etidronate is not approved for the treatment of postmenopausal osteoporosis in the United States; it is approved for the treatment of Paget's disease. Alendronate, a nitrogen-containing bisphosphonate, was approved by the U.S. Food and Drug Administration (FDA) for the treatment of postmenopausal osteoporosis in the mid-1990s and was followed in the marketplace by other nitrogen-containing compounds, including risedronate, ibandronate, and zoledronate (zoledronic acid).
Although bisphosphonates are a first-line treatment for postmenpausal osteoporosis, they are not alike with respect to their evidence of clinical efficacy. They are also not identical in potency and affinity for distribution at skeletal sites throughout the body. Randomized controlled trials (RCTs) have demonstrated differences among these agents in the reduction of both vertebral and nonvertebral fractures. There is ample evidence from RCTs to support the vertebral antifracture efficacy of alendronate, 6,7 risedronate, 8,9 ibandronate, 10 and zoledronate 11,12 in postmenopausal women with osteoporosis, but not all of these agents have shown nonvertebral antifracture efficacy. It should be noted that although many trials have been conducted to evaluate the efficacy of the bisphosphonates, these trials can differ with regard to their design and patient/study subject's baseline characteristics. Therefore, cross-trial comparisons should be made with caution.
Randomized controlled trials
Vertebral fracture risk reduction
All the bisphosphonates approved for treatment of osteoporosis display efficacy in reducing the risk of vertebral fracture. The efficacy of alendronate against vertebral fractures was evaluated in the Fracture Intervention Trial (FIT), which consisted of two distinct arms including 2027 women, aged 55–81 years, with an existing vertebral fracture (FIT-1) 6 and 4432 women with osteoporosis but without a vertebral fracture (FIT-2). 7 Alendronate significantly reduced the risk of new vertebral fractures, defined by radiograph, in both groups at 36 months: this risk reduction was 47% in women with an existing vertebral fracture (p < 0.001) 6 and 44% in women with low bone mineral density (BMD) but no vertebral fracture (p = 0.001). 7
The vertebral antifracture efficacy of risedronate in women with osteoporosis is supported by the Vertebral Efficacy with Risedronate Therapy (VERT) trial, which had North American (VERT-NA) 8 and multinational (VERT-MN) 9 arms. The VERT-NA included 2458 postmenopausal women, <85 years, with ≥1 vertebral fracture at baseline. 8 After 3 years, the incidence of new vertebral fractures, defined radiographically, was reduced by 41% with risedronate compared with placebo (p = 0.003). 8 A similar pattern of response was observed when new and worsening vertebral fractures were also evaluated. The VERT-MN included 1226 postmenopausal women with ≥2 vertebral fractures. 9 Risedronate reduced the incidence of vertebral fracture by 49% (p = 0.001). 9 In the VERT-NA and VERT-MN studies, a significant reduction in the risk of morphometric vertebral fracture, 65% and 61%, respectively, was seen at 1 year.
Ibandronate has been shown to be efficacious against vertebral fractures in women with documented osteoporosis in the oral iBandronate Osteoporosis vertebral fracture trial in North America and Europe (BONE). Oral daily ibandronate (2.5 mg) and intermittent ibandronate (20 mg every other day for 12 doses every 3 months) were compared with placebo in a group of 2946 postmenopausal women who had osteoporosis and a prevalent vertebral fracture. At 3 years, the risk reduction for new morphometric vertebral fractures was 50% with the intermittent regimen (p = 0.0006) and 62% with the daily regimen (p = 0.0001). 10
The efficacy of zoledronate against vertebral fractures in women with postmenopausal osteoporosis has been demonstrated in the Health Outcomes and Reduced Incidence with Zoledronic acid ONce yearly (HORIZON) Pivotal Fracture Trial. 11 In this study, 3889 women who received a single 15-minute infusion of zoledronate at baseline and at 12 and 24 months were compared with 3876 women who received placebo. Treatment with zoledronate reduced the risk of new morphometric vertebral fracture by 70% at the end of a 3-year period compared with placebo (p < 0.001). 11 A similar reduction in the risk of vertebral fracture was seen at 1 and 2 years, 60% and 71%, respectively. 11 In the HORIZON Recurrent Fracture Trial, patients with a recent hip fracture were randomly assigned to zoledronate (n = 1065) or placebo (n = 1062), and these were administered by 15-minute i.v. infusion within 90 days after surgical repair of the hip fracture and every 12 months thereafter. 12 Zoledronate was shown to reduce the rate of new clinical vertebral fractures. At follow-up (median 1.9 years), this rate was 1.7% for the zoledronate group and 3.8% for the placebo group (p = 0.02). 12
Nonvertebral fracture risk reduction
Some of the clinical trials discussed were also designed to include prospective end points regarding the incidence of nonvertebral fracture, a composite end point that often comprises the skeletal sites—clavical, humerus, wrist, pelvis, hip, and leg—and where the efficacy of the bisphosphonates has been shown to differ. The FIT trial in women with existing vertebral fractures (FIT-1) had a secondary end point of any clinical fracture, which included any nonvertebral fracture, but the reduction in any nonvertebral fracture incidence in the alendronate treatment group did not reach statistical significance. 6 Analysis of the pooled data (FIT-1 and FIT-2) showed that alendronate reduced risk of any nonvertebral clinical fracture by 27% (p < 0.001). 13
In the VERT trials, nonvertebral osteoporosis-related fractures were included as an additional efficacy measure. 8,9 After 3 years, the cumulative incidence of nonvertebral fractures was reduced by 39% in VERT-NA with risedronate compared with control (p = 0.02), 8 but the 33% reduction in this end point found in VERT-MN did not reach statistical significance. 9
A study by Boonen et al. 14 investigated the effects of osteoporosis treatments on the risk of nonvertebral fracture. Meta-analysis of data from alendronate and risedronate trials, using the intention-to-treat population, demonstrated that both drugs significantly reduced the risk of nonvertebral fracture (p = 0.012 and p = 0.001, respectively). 14
The efficacy of ibandronate for the reduction of nonvertebral fracture risk has not been demonstrated prospectively. 10 In a post hoc analysis, it was shown that the daily regimen of ibandronate reduced the risk of nonvertebral fractures by 69% (p = 0.012) when the data were stratified according to low BMD (T-score <−3.0) at the femoral neck. 10 Recent studies have suggested ibandronate may provide nonvertebral fracture risk reduction. 15,16 A meta-analysis conducted by Harris et al. 15 evaluated 8710 patients from the BONE, IV fracture prevention, Monthly Oral iBandronate In LadiEs (MOBILE), and Dosing IntraVenous Administration (DIVA) studies for nonvertebral fracture risk reduction. Patient data were grouped into three dose levels based on annual cumulative exposure (ACE). The findings suggested that ibandronate at ACE ≥10.8 mg (equating to 150 mg monthly or 3 mg i.v. quarterly) may provide nonvertebral and clinical fracture risk reduction. However, the results from this study were limited by incomplete patient baseline data, and some clinical trial data were not placebo controlled. 15 Another meta-analysis of eight randomized clinical trials evaluating ibandronate investigated a dose-dependent effect with regard to nonvertebral fracture risk reduction. 16 Definitions of high and low doses were also based on ACE. There was a significant reduction in the risk of nonvertebral fractures when data were pooled from trials using ACE doses of ≥10.8 mg vs. ACE ≤7.2 mg and 5.5 mg. 16
In the HORIZON Pivotal Fracture Trial, the incidence of all nonvertebral fractures was reduced by 25% (p < 0.001) in women receiving zoledronate. 11 The secondary end points in the HORIZON Recurrent Fracture Trial included nonvertebral fracture, and it was demonstrated that the incidence of new nonvertebral fractures was also reduced by 27% (p = 0.03) in the zoledronate group. 12
Hip fractures are the most common nonvertebral fractures and are associated with significant morbidity and mortality. 17,18 Few trials have been designed to include hip fracture as a prospective end point, although trials that have examined this outcome have also indicated differences among the bisphosphonates.
In the FIT trial in women with existing vertebral fractures (FIT-1), the secondary end point of any clinical fracture was further grouped as hip and wrist as well as any nonvertebral fracture. In contrast to any nonvertebral fracture risk, there was a significant reduction in the risk of hip (p = 0.047) and wrist (p = 0.013) fractures with alendronate compared with placebo. 6 In the post hoc analysis of the pooled data, it was also demonstrated that alendronate reduced the risk of hip fracture by 53% (p = 0.005) and wrist fracture by 30% (p = 0.038). 13
The Hip Intervention Program study was designed to evaluate risedronate treatment over a period of 3 years in elderly women, with a primary efficacy end point of hip fracture. 19 Risedronate was shown to reduce the risk of hip fracture by 40% in women (70–79 years) with confirmed osteoporosis when compared with placebo (p = 0.009). 19 Hip fracture was a primary end point in the HORIZON Pivotal Fracture Trial, and its risk was reduced by 41% with zoledronate compared with placebo (p = 0.002), 11 which was consistent with any nonvertebral fracture risk reduction. The secondary end points in the HORIZON Recurrent Fracture Trial also specified hip fracture, but unlike any nonvertebral fracture risk reduction, the 30% relative risk (RR) reduction of new hip fracture with zoledronate was not statistically significant. 12
The available RCT data on bisphosphonates are greatly limited to the comparison of a single treatment against placebo. No head-to-head comparisons exist in which fracture risk reduction is assessed. There have been three trials comparing bisphosphonates head-to-head, and for each of these, BMD was the primary end point. The Fosamax Actonel Comparison Trial (FACT) 20,21 compared once-weekly alendronate with once-weekly risedronate, but BMD, rather than fracture incidence, was the primary end point. There were greater increases in BMD and greater reductions in bone turnover markers seen with alendronate. The Monthly Oral Therapy with Ibandronate for Osteoporosis iNtervention (MOTION) study was designed as a noninferiority trial where once-monthly ibandronate (150 mg) was compared with weekly alendronate (70 mg). The primary efficacy end points were change from baseline in mean lumbar spine and total hip BMD after 12 months therapy, and the two therapy regimens were shown to be clinically comparable. 22 A recent 1-year study demonstrated that a single 5-mg i.v. infusion of zoledronate was noninferior and superior to 5 mg of risedronate daily in increasing lumbar spine BMD. 23 Unfortunately, given the high cost and large sample size required to design a comparative study that would have the statistical power to demonstrate a significant difference in fracture risk reduction between two treatments, such a trial is unlikely to be undertaken.
Onset of efficacy
In addition to differences in antifracture efficacy, in particular nonvertebral fracture reduction, bisphosphonates also differ with respect to their speed of onset of action. In the majority of clinical studies, onset of efficacy is not a prespecified outcome measure, and so analysis is often conducted post hoc. The pooled post hoc analysis of FIT showed a clinical vertebral fracture risk reduction by 1 year and a reduction in nonvertebral fractures by 2 years after treatment with alendronate. 13 The reduction in hip fracture was evident by month 18. In the VERT studies, spinal radiographs were available after 1 year of treatment, so that the onset of the antifracture effect could be evaluated in a retrospective analysis. A significant risk reduction was shown for vertebral fractures as early as 6 months with risedronate compared with placebo. 24 A meta-analysis of four RCTs showed a significant reduction in the risk of nonvertebral fractures at 6 months after treatment with risedronate compared with control. 25 Retrospective analysis of the BONE study demonstrated the efficacy of ibandronate in reducing the risk of combined new moderate and severe vertebral fractures within 1 year of treatment. 26 Zoledronate was demonstrated to have efficacy in reducing new morphometric vertebral fractures after 1 year in the HORIZON Pivotal Fracture Trial. 11
Observational database studies
An RCT is the most methodologically rigorous design and remains the most appropriate means for determining drug efficacy. With their tightly controlled conditions, RCTs maximize the likelihood that observed differences between treatments are, indeed, a reflection of actual differences between comparators. However, the required conditions of an RCT are not reflected in the real world setting of the clinic. Most osteoporosis patients in a clinical practice would be ineligible to participate in an RCT because of inclusion/exclusion criteria, such as comorbidities, previous treatment with bone-active agents, or the use of other medications known to affect the skeleton. 27 To address this limitation and to complement the results obtained from RCTs, the appeal of observational studies using information from large-scale databases continues to grow. In these studies, the impact of a treatment is evaluated in large, diverse patient populations, providing clinicians with information applicable to a broader spectrum of patients, who are more likely to resemble those they find in their own practices. They can more readily provide data on long-term drug effectiveness and safety because they are often able to evaluate data from longer observation periods, 28 and they offer evaluation of real world treatment persistence and compliance data that have been shown to influence clinical outcomes. Data obtained from observational studies can never be completely adjusted for all potential confounders, however, and do not reflect inherent comparative efficacy between various drugs. Despite this, well-designed observational studies offer an alternative approach with which to evaluate the relative effectiveness of two treatments and can complement existing data from RCTs. 29
Several observational studies using large databases have evaluated the impact of selected osteoporosis treatments on fracture prevention. One such study used data from an integrated administrative, medical, and pharmacy claims database to evaluate the impact of early treatment on subsequent fracture prevention in 7233 women with a clinical vertebral fracture. 30 Women who received treatment had a significantly lower risk of sustaining a subsequent fracture compared with those who received no treatment. Furthermore, the RR of subsequent fracture compared with no treatment differed among the osteoporosis treatments: risedronate (RR = 0.30, p < 0.01), alendronate (RR = 0.47, p < 0.01), and nasal calcitonin (RR = 0.67, p = 0.03).
Another observational study comparing risedronate, alendronate, and calcitonin used a proprietary administrative claims database. Patient records were analyzed for the incidence of nonvertebral fractures in the first 6 and 12 months after initiation of treatment. The RR reduction (adjusted for differences in the patient groups) for nonvertebral fractures at 6 and 12 months, respectively, was 69% and 75% for risedronate vs. calcitonin, 54% and 59% for risedronate vs. alendronate, and 26% and 25% for alendronate vs. calcitonin. 31 These results are similar to fracture risk reductions observed in RCTs and demonstrate that observational data can complement and support findings from RCTs. 13,25
The RisedronatE and ALendronate (REAL) study 32 also illustrates the value of observational database research in supporting RCT findings in actual clinical settings. The incidence of nonvertebral fractures in U.S. women aged ≥65 years was evaluated from healthcare utilization records of 12,215 risedronate and 21,615 alendronate users. After 12 months of treatment, the incidence of nonvertebral fractures in the risedronate cohort (2.0%) was 18% lower (95% CI 2-32, p ≤ 0.05) than in the alendronate cohort (2.3%). The incidence of hip fractures with risedronate (0.4%) was 43% lower (95% CI 13-63, p < 0.05) than in the alendronate cohort (0.6%).
A recent, head-to-head, observational database study evaluated fracture rates of monthly ibandronate and weekly bisphosphonates. 33 The study included women aged ≥45 years and evaluated hip, nonvertebral, vertebral, and any clinical fracture risk in 7,345 patients receiving monthly ibandronate and 56,837 patients receiving weekly bisphosphonates. After the 12-month observational period, fracture rates were <2%, and fracture risk was not found to be significantly different between patients receiving monthly and weekly bisphosphonates for hip, nonvertebral, or any clinical fracture (adjusted RR [ARR], 95% CI: hip = 1.06, 0.61–1.83, p = 0.840; nonvertebral = 0.88, 0.71–1.09, p = 0.255; any clinical = 0.82, 0.66-1.00, p = 0.052). Patients receiving monthly ibandronate were shown to have a significantly lower risk of vertebral fractures than patients receiving weekly bisphosphonates (ARR 0.36, 95% CI 0.18-0.75, p = 0.006). 33
Osteonecrosis of the jaw and pathological fracture
There have been reports in the literature of rare phenomena associated with bisphosphonate use, such as osteonecrosis of the jaw (ONJ) and low-energy subtrochanteric fractures. The first reports of ONJ in 2003 were in cancer patients receiving high-dose i.v. bisphosphonates for the treatment of hypercalcemia of malignancy, and the first review appeared in the literature in 2004. 34 The occurrence of ONJ is uncommon in cancer patients and is even rarer in osteoporosis patients. It has been estimated that the risk of ONJ in individuals receiving bisphosphonate therapy for osteoporosis is between 1 in 10,000 and <1 in 100,000 patient-treatment years. 35 Furthermore, its incidence in the general population not receiving bisphosphonates is unknown. Reports of subtrochanteric insufficiency fractures being associated with long-term alendronate use have been published recently. 36 –38 Although it has been hypothesized that long-term use of bisphosphonates may lead to oversuppression of bone turnover, to date there has been no evidence for a causal link between bisphosphonates for the treatment of postmenopausal osteoporosis and ONJ or pathological fracture; further studies are warranted, however.
Studies in clinical medicine
RCTs and observational database studies have suggested differences between osteoporosis therapies. Depending on the severity of osteoporosis or the presence of multiple risk factors, some patients might require treatment with another therapy, such as teriparatide. Teriparatide is an anabolic agent approved by the FDA for the treatment of osteoporosis in men and postmenopausal women at high risk of fracture. However, treatment with teriparatide is not recommended for longer than 2 years. As some patients may have received antiresorptive treatment before subsequent treatment with teriparatide, recent studies have investigated the effects that different antiresorptives and, more specifically, the effects that different bisphosphonates have on the skeleton and its subsequent response to the anabolic effects of teriparatide. 39 –42 A recent study by Boonen et al. 40 reported that although teriparatide was effective in increasing bone formation markers and areal BMD in patients previously receiving antiresorptive therapy, regardless of type or duration, the response was less robust than in those patients who had not received prior treatment. Another recent study suggests that there are differences in the early responsiveness to teriparatide in patients previously treated with risedronate compared with patients previously treated with alendronate. 41 The study showed that bone turnover markers demonstrate greater and earlier responsiveness to teriparatide after treatment with risedronate than with alendronate. 41 The study findings also showed a greater response to the anabolic effects of teriparatide, with regard to both areal and volumetric BMD at the spine after 12 months of treatment, in patients previously treated with risedronate. Changes in 3-month procollagen type 1 amino-terminal propeptide (P1NP) correlated with changes in 12-month volumetric BMD at the spine. 41
Structure-function relationships
Recent investigations into the physicochemical properties and pharmacokinetics of bisphosphonates have provided further information about their differences, which may eventually explain RCT and observational study findings. 43 –46 All bisphosphonates are selectively taken up by the mineral surface of bone, and they further inhibit the resorption of bone by osteoclasts. 47 Seventy percent of bone is composed of hydroxyapatite (forming the acellular, mineralized matrix of bone), and osteoclasts resorb bone tissue by removing the bone's mineralized matrix. The bisphosphonates in clinical use share a common core structure that gives rise to the ability of these drugs to act on bone. The carbon-phosphonate structure of bisphosphonates resembles that of the inorganic pyrophosphate (oxygen-phosphonate) found in hydroxyapatite, and the similarity of these molecular structures underlies the ability of the bisphosphonate compounds to bind to bone. However, each bisphosphonate binds differently to hydroxyapatite: some bind quite tightly to the bone surface, and others bind to a lesser degree. Furthermore, bisphosphonates differ with regard to their ability to inhibit farnesyl diphosphate (FPP) synthase, a key enzyme in osteoclast function.
Each bisphosphonate has a unique molecular structure, and the differences in structure could be responsible for differences seen in the rapidity of onset of action, relative potency and efficacy, and, potentially, the protective effects of each bisphosphonate against vertebral and nonvertebral fractures.
Are the Clinical Differences Among Bisphosphonates Explained by Differences in Their Chemical Structure and Pharmacodynamics?
It is important to recognize that differences in the molecular structure of bisphosphonates lead to differences in their physicochemical and pharmacological properties. The central (carbon) atom in the bisphosphonate molecule is bonded to two phosphonate moieties and two other groups or side chains, often termed R1 and R2 (Fig. 1). The bisphosphonates in clinical use contain a hydroxyl (OH) group at the R1 position, which enhances their ability to bind to bone. The two phosphonate groups together with this hydroxyl group act as a “bone hook,” which is essential for binding to hydroxyapatite and for the biochemical mechanism of action. The R2 side chain appears to play a major role in the interaction between bisphosphonates and their pharmacological target, 45 where small modifications in the R2 side chain structure can afford substantial changes in the antiresorptive properties of these compounds.
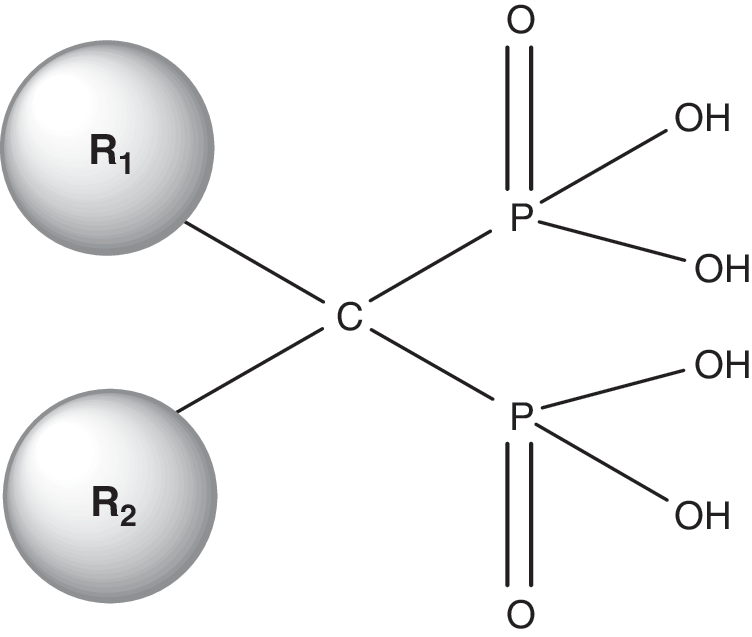
The basic structure of bisphosphonates. The carbon atom in the center of the bisphosphonate chain contains an R1 and R2 side chain. Bisphosphonates in clinical use contain a hydroxyl (OH) group at the R1 position, which enhances binding to bone. The presence of nitrogen within the R2 side chain increases potency.
Nitrogen-containing bisphosphonates
The four bisphosphonates currently FDA approved in the United States for treatment of osteoporosis all contain nitrogen in their R2 side chain. However, the orientation of nitrogen atom(s) within the R2 side chain varies significantly among the different drugs (Table 1). The inclusion of nitrogen atom(s) allows for greater efficacy than was seen in an earlier generation of bisphosphonates. 47 For example, alendronate, which contains a primary nitrogen atom within its R2 side chain, is 10–100 times more potent than etidronate, which has a methyl (CH3) group at the R2 position. 47 Further, the orientation of nitrogen atom(s) in the R2 carbon chain plays a role in the relative potency of each bisphosphonate. For instance, risedronate and zoledronate, in which the nitrogen is located within a heterocyclic ring, have been shown in experimental systems to be up to 10,000-fold more potent than etidronate. 47
Physicochemical properties
Differences in the molecular structures of bisphosphonates lead to their different physicochemical properties and influence their binding affinities to bone mineral. 43,44 The in vitro affinity constant (a measure of the binding affinity of a bisphosphonate to hydroxyapatite under conditions likely to simulate those seen in vivo) varies with the composition of the R2 side chain. There are considerable differences in the binding constants of the bisphosphonates, with the rank order of them being zoledronate > alendronate > ibandronate > risedronate > etidronate. 43 In addition to differences in binding constants, there are significant differences in the ability of these compounds to alter zeta potential (the electrical potential that exists across the interface of all solids and liquids) and, therefore, have an effect on the localized surface charge on bone. At physiological pH, the effect of bisphosphonate binding to hydroxyapatite on the surface charge is in the rank order alendronate > ibandronate > zoledronate > etidronate > risedronate. 48 Modulation of the surface charge can play a role in the further adsorption of other charged molecules to the bone's surface, the amount of bisphosphonate that can bind to the bone surface, and the distribution of the bisphosphonate across various skeletal sites. 49
It has been hypothesized that there is continuous recycling of bisphosphonate onto and off bone, which is supported by the observation that bisphosphonates can be found in the plasma and urine for months after discontinuation of administration. 47 There are also considerable differences among bisphosphonates with regard to their uptake and persistence in bone, such as timing of onset/offset of effect, length of half-life, action at the bone surface, and distribution of the drug to various skeletal sites. 43 Marked differences in the binding of bisphosphonates to hydroxyapatite may explain potentially important differences in their potencies and durations of action, and the variation in drug retention and persistence of effect after administration. 47 High-affinity bisphosphonates, such as zoledronate and alendronate, undergo rapid and avid uptake by bone and have a strong attachment to bone, low desorption, and less diffusion in bone. In contrast, lower-affinity bisphosphonates, such as risedronate, undergo weaker uptake and have lower attachment, higher desorption, and more diffusion in bone. 43 These observations may account for the prolonged duration of action of some bisphosphonates and the quicker offset of effect demonstrated by others.
Cellular effects
Bisphosphonate binding to the mineral portion of bone brings them into close proximity to osteoclasts. Earlier-generation bisphosphonates, such as etidronate, cause osteoclast death by being metabolically incorporated into nonhydrolyzable analogs of adenosine triphosphate (ATP). In contrast, nitrogen-containing bisphosphonates act by inhibiting the function of key enzymes (including FPP synthase) in the osteoclast biosynthetic mevalonate pathway. 45,46 Differences in the antiresorptive potency of bisphosphonates may be due to the varying degrees to which they inhibit these enzymes, where the rank order has been shown to be zoledronate > risedronate > ibandronate > alendronate >>>>> etidronate. 48 There is a clear correlation between the ability of different bisphosphonates to inhibit bone resorption in vivo and their ability to inhibit FPP synthase in vitro. 45 Minor changes in the composition and structure of the R2 side chain lead to variation in enzyme inhibitory potency, which in turn can lead to variation in the degree of bone resorption. 45 In addition to their role in osteoclast activity, more recent data have suggested that bisphosphonates may also play a role in preventing osteocyte apoptosis. 51,50 However, further studies are required to investigate this.
Although bisphosphonates share a common backbone structure, differences in the composition of their R2 side chain have been shown to affect how they bind to bone mineral and inhibit key enzymes. This could account for the differences observed in their bone-remodeling properties. Bisphosphonate binding affinity is enhanced by the presence of nitrogen in the drug's molecular structure. Bisphosphonate enzyme inhibitory potency is related to the presence of nitrogen in the R2 side chain, as well as its orientation within the side chain and, subsequently, the shape adopted by the bisphosphonate molecule. A clearer understanding of the structure-function relationships of different bisphosphonates should allow for an improved understanding of their mechanisms of action, which could explain observed differences in the relative efficacy of these compounds demonstrated at various skeletal sites.
Summary of clinical implications
Bisphosphonates for the treatment of postmenopausal osteoporosis demonstrate fracture risk reduction at the spine, whereas evidence of fracture risk reduction at nonvertebral sites has been shown to differ. The speed of onset of antifracture efficacy has also been shown to differ among bisphosphonates (Table 2), and there are pharmacological differences among the bisphosphonates (Table 2) that can influence their skeletal uptake, duration of action, and pharmacological potency. It would seem reasonable to hypothesize that differences in mineral binding affinity and FPP synthase inhibitory potency would be predictive of the duration of action of bisphophonates. 48 Strong mineral binding affinity would likely be associated with greater suppression of bone turnover and longer persistence of effect, such as that seen with alendronate and zoledronate. 48 Greater enzyme inhibitory potency is likely to correlate well with overall antiresorptive effect, as well as with speed of onset of action, as can be illustrated with risedronate and zoledronate, particularly with regard to vertebral fracture risk reduction. 48
FPPS, farnesyl disphosphate synthase.
Relatively speaking, alendronate demonstrates a high mineral binding affinity and an intermediate enzyme inhibitory potency, which would indicate a greater reduction of bone turnover and a longer duration of effect. 48 Risedronate has moderate mineral binding affinity and a high enzyme inhibitory potency. Its lower mineral attachment suggests it has the potential to distribute more widely in bone and across skeletal sites; its high enzyme potency could contribute to a relatively fast onset of action. 48 With respect to alendronate, ibandronate has a higher enzyme inhibitory potency, and its mineral binding affinity lies between that of alendronate and risedronate. These properties would suggest it might have similar antifracture properties to both alendronate and risedronate, and although this has been demonstrated with regard to vertebral fracture efficacy, it has not been shown for nonvertebral fractures in clinical trials. 48 Relative to the other three bisphosphonates, zoledronate is the strongest inhibitor of FPP synthase and has the highest mineral binding affinity, indicating high potency and a long duration of action. 48 No two bisphosphonates share the same physicochemical or pharmacological profile, and it is important to be aware of these differences when assessing individual patients for whom bisphosphonate therapy would be appropriate.
Conclusions
RCTs and real world observational database studies have shown clinically meaningful differences among the bisphosphonates currently available for postmenopausal osteoporosis, in terms of both the scope of antifracture efficacy and the speed of onset of effect provided by each. Although these differences could be claimed to be caused by variations in study design, recent evidence suggests that the unique properties of these agents with regard to their mechanisms of action could explain the differences observed in clinical effectiveness. All bisphosphonates used in the treatment of postmenopausal osteoporosis share a similar core structure, but differences with regard to their R2 side chains and the presence (or absence) of nitrogen point to more fundamental explanations for variations within the class of therapies. Research into their modes of action continues, but it is reasonable at this juncture to speculate that all bisphosphonates are not exactly identical and, consequently, that variations in clinical study findings may very well be a reflection of these fundamental differences.
Footnotes
Acknowledgments
J.A.S. received editorial/writing support in the preparation of this article from the Alliance for Better Bone Health (Procter & Gamble Pharmaceuticals and sanofi-aventis US, Inc.). Betty Thompson, Ph.D., from Excerpta Medica provided editorial and writing assistance. J.A.S. has received grant/research support from BioSante, Boehringer Ingelheim (Ingelheim, Germany), FemmePharma (Wayne, PA), GlaxoSmithKline, Nanma/Tripharma/Trinity, Novartis (Basel, Switzerland), Procter & Gamble (Cincinnati, OH), QuatRx Pharmaceuticals, and Teva Pharmaceuticals Ltd.
Disclosure Statement
In the interest of full disclosure, J.A.S. wishes to state that he has served as a consultant on the advisory boards of Allergan (Irvine, CA), The Alliance for Better Bone Health (Cincinnati, OH), Amgen Inc. (Thousand Oaks, CA), Ascend Therapeutics (Herndon, VA), Bayer (Leverkusen, Germany), BioSante (Lincolnshire, IL), Boehringer Ingelheim (Ingelheim, Germany), Concert Pharmaceuticals (Lexington, MA), Corcept Therapeutics, Inc. (Menlo Park, CA), Depomed Inc. (Menlo Park, CA), GlaxoSmithKline (Philadelphia, PA), KV Pharmaceutical Co. (St. Louis, MO), Lipocine Inc. (Salt Lake City, UT), Meditrina Pharmaceuticals (Ann Arbor, MI), Merck (Whitehouse Station, NJ), Merrion Pharmaceuticals (Wilmington, NC), Nanma/Tripharma/Trinity (Glen Arm, MD), NDA Partners LLC (Lakewood Ranch, Florida), Novo Nordisk (Bagsvrerd, Denmark), Novogyne (East Hanover, NJ), Pear Tree Pharmaceuticals (Cambridge, MA), QuatRx Pharmaceuticals (Ann Arbor, MI), Roche (Basel, Switzerland), Schering-Plough (Kenilworth, NJ), Sciele (Atlanta, GA), Solvay (Marietta, GA), Teva Pharmaceutical Industries Ltd (Jerusalem, Israel), Ther-Rx (Bridgetown, MO), Warner Chilcott (Rockaway, NJ), and Wyeth (Madison, NJ). He has also served on the speakers bureaus of Amgen, Ascend, Bayer, Boehringer Ingelheim, GlaxoSmithKline, KV Pharmaceutical Co., Merck, Novartis, Novogyne, Sciele, Teva Pharmaceuticals, Ther-Rx, Warner Chilcott, and Wyeth.