
Abstract
Purpose:
To determine the reasons why urology has become an increasingly popular career choice for women medical students and to uncover challenges they face during their training period.
Methods:
A mailed survey was sent to all 176 female urology residents.
Results:
Fifty-five surveys were received, for a return rate of 31%. General surgery was the most common alternative specialty choice considered by female urology trainees, although there was wide representation from other disciplines. Diversity of procedures was the most frequently cited reason for choosing urology. The majority of respondents interested in fellowships expect to seek training in pediatric or female/reconstructive urology. More than half of these residents have been confronted with negative behavior by male patients and by male colleagues in relation to their gender.
Conclusions:
Understanding the perspectives, concerns, and predilections of women urology applicants and trainees is essential to maximize the contributions women will make to the specialty and its patients.
Introduction
Over the past 40

The 12-year trend of females filling first-year urology residency positions.
The reasons for the expanding interest in and choice of urology by distaff medical students have not been specifically considered. Previous reports have addressed related issues. Andriole et al. 3 investigated the views of women surgical residents, with a particular focus on orthopedics. Kerfoot et al. 4 assessed the attitudes of medical students toward the possibility of a career in urology and the problems they might face in practice, and Lightner et al. 2 studied the opinions of fully trained female urologists.
A recent article in The New York Times entitled “Urology Field Slowly Altered, by Women,” by Barron H. Lerner, M.D., speaks to the level of interest in this trend among both the medical field and the lay public. 5 We undertook this investigation to evaluate the experiences and predilections of women urologists currently in residency programs. We were particularly interested in responses to questions assessing why the residents chose urology, whether they sought or plan to seek further training through fellowships, and what challenges related to their gender they had to deal with during the training period.
Materials and Methods
After obtaining IRB approval, we mailed a self-administered five-item, one-page questionnaire to all female urology residents in the United States in December 2006. The trainees' names and addresses were obtained from the American Medical Association mailing list of physicians in graduate medical education programs. Responses were kept anonymous but were recorded on an Excel spreadsheet (Microsoft Corporation, Redmond, WA) for frequency evaluations. The five questions were: Before deciding to complete a urology residency, what other fields did you consider? What factors influenced your decision to choose urology? Do you plan on applying for a fellowship? If so, what type? What specific challenges have you faced as a female urology resident?
Respondents were asked to choose the most appropriate response among the options given and were allowed to choose more than one response where appropriate. The possible answer choices are outlined in Figures 2, 3, and 4 and Table 1.
Results
Of the 176 questionnaires, 55 were returned, for a response rate of 31%. When queried about considerations of other specialties as career choices (Fig. 2), by far the most common response was general surgery, which was reported by 60% of the respondents. Thirty-six percent were attracted to obstetrics/gynecology, 24% were somewhat inclined toward pediatrics, and 14% mulled over family or internal medicine before ultimately deciding on urology. Specialties having a presumed manageable lifestyle, such as pathology, dermatology, and radiology, were potentially attractive to relatively few of the respondents (Fig. 2).

Response to the question: What other fields did you consider?
Nonetheless, the perceived lifestyle of a urologist was the third most frequently cited factor that influenced the decision to pursue training in the specialty (Fig. 3). It was deemed important by 67% of the respondents. Even more popular as reasons for deciding on urology were the diversity of procedures practiced by the specialty, chosen by 88%, and diversity of practice, cited by 75% of those who completed the questionnaire. A slight majority affirmed the influence of the patient population treated by urologists, whereas less than half of the respondents cited the importance of long-term care, financial compensation, or medical management of urological diseases to be motivating factors for choosing this specialty.
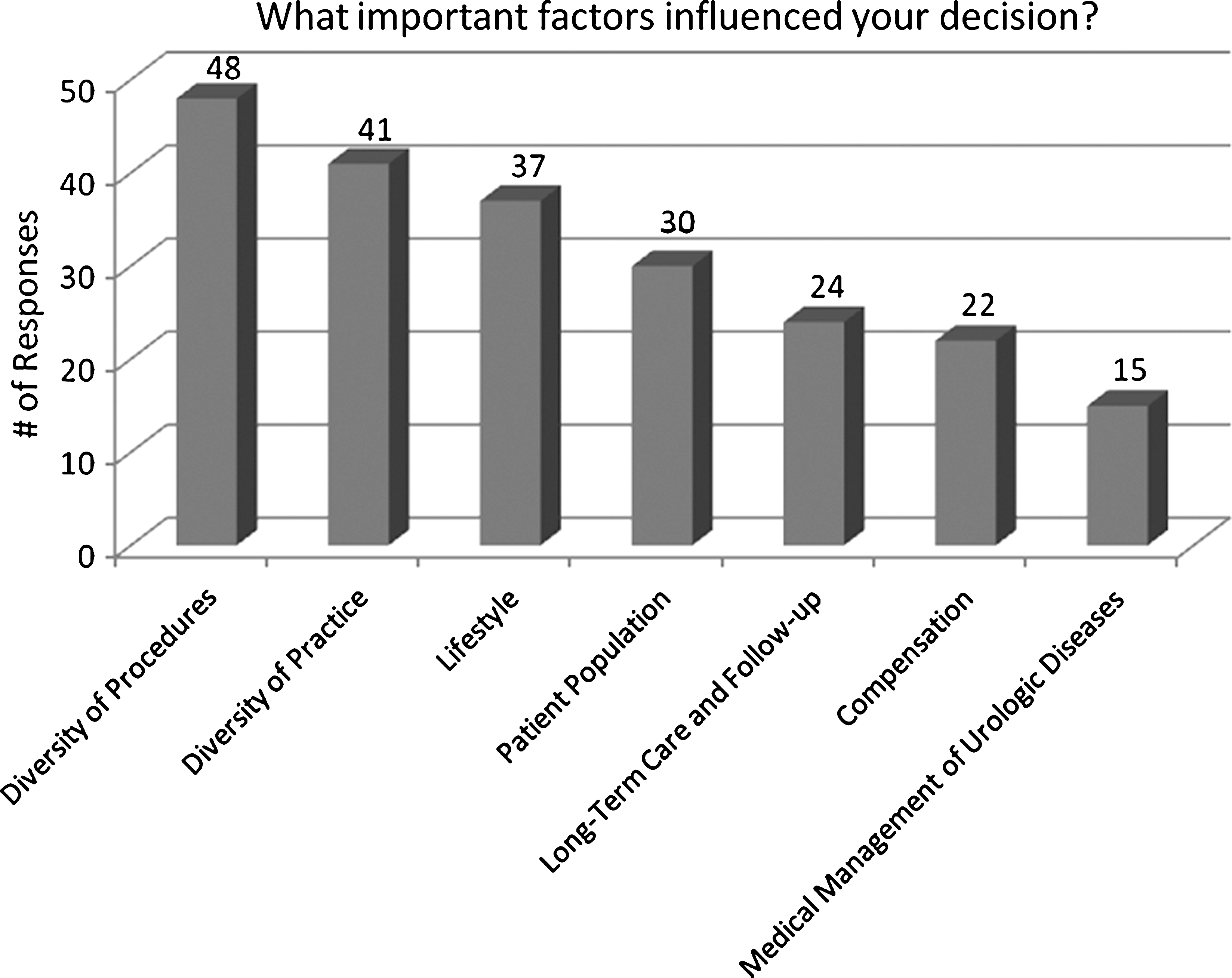
Response to the question: What important factors influenced your decision?
Sixty percent of the respondents planned to apply for a fellowship, with 5% still undecided. The actual percentage of fellowships that female residents may pursue may be higher because trainees in all postgraduate years were queried; junior residents are apt to become more interested in fellowships as their interests become more focused and their mastery increases with the length of training. The two most common fellowship choices were pediatrics and female/reconstructive urology (Fig. 4).
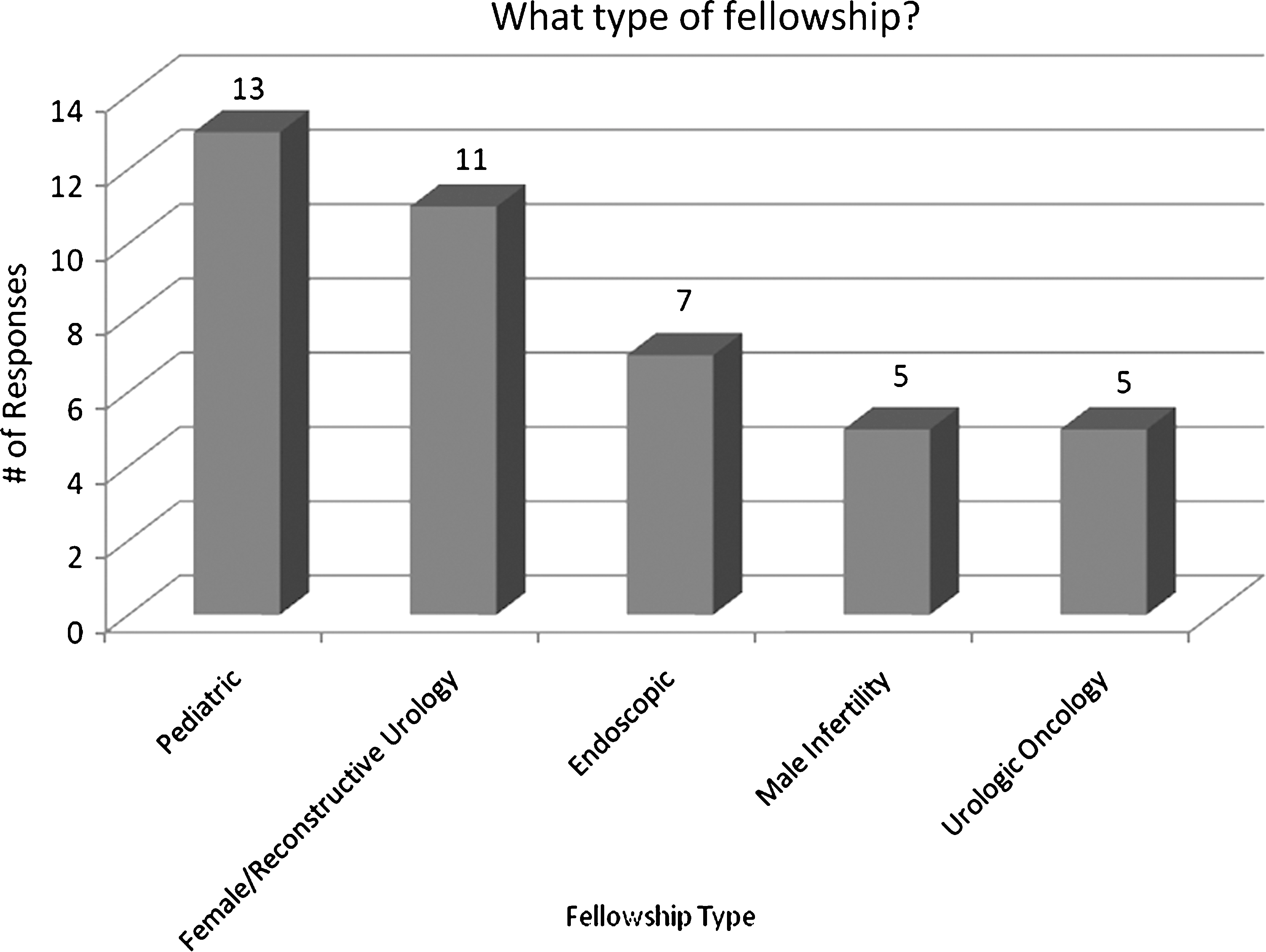
Response to the question: What type of fellowship?
When asked what specific challenges were faced as a female urology resident, refusal by male patients to be seen by a woman urologist was cited by 60% and inappropriate treatment by male patients was recollected by 29% (Table 1). Inappropriate treatment by male superiors, colleagues, and ancillary staff was a complaint reported by 36%, and sexual harassment was noted by 22%. A range of written comments volunteered by the respondents supplemented their acknowledgment of discrimination.
Discussion
Alternative specialties
It is tempting to believe that women in medicine maintain shared views that affect to some degree their preferences for some specialties. The notion of a so-called manageable lifestyle could explain the increasing penetration of women in dermatology, which is predominantly an outpatient, office-based specialty with limited requirements for after-hours duty. Yet lifestyle determinism cannot account for the fact that specialties with generally limited after-hours, patient-centered responsibilities, such as radiology, are no more frequently sought by women now than a decade ago, despite the concomitant steady increases in the percentage of female medical students. The specialties associated with a nurturing lifestyle have been purported to be more aligned with positive career expectations held by female medical students and is offered as the reason for the greater participation by women in pediatrics, internal medicine, and family medicine. The fact that nearly all surgically related specialties are also increasing their complement of women, both relatively and absolutely, in residencies and beyond, however, argues against the imputation of a simplistic rationale about what constitutes alluring specialties related to gender. The frequent consideration of general surgery by the respondents of this survey as an alternative residency raises the possibility that men and women choose urology because it is a surgical specialty.
Regardless of the existence of supposedly differing attitudes toward career choice in medicine held by men and women, lifestyle was the third most frequently cited factor influencing the decision for urology. This collective view underscores an awareness and acceptance of the demands of surgical practice and its accompanying satisfactions, which are deemed more desirable then disheartening. Implicit in this sensibility is the fact that there is no de facto conflict between the assumed polarities of surgical time obligations and after-hours leisure. In effect, this response suggests that for such residents, pleasure in work, even when daunting, is not an oxymoron.
The rapidly growing number of women in urology residency positions reflects a steady trend. Over the past 12 years, it has advanced from slightly more than 7% in 1994 to 18% in 2005, an increase of 150%. What is more, that increasing percentage is a phenomenon unsurpassed by any other specialty. From 1994 to 2005, the contribution of women to the resident pool in ophthalmology rose 30% from 25.5% to 38%, and in anesthesiology, the increase was 27%, as women now comprise 30.7% of trainees in that specialty. In dermatology, the number of women in the resident workforce expanded by 22% to 30.7% of trainees; in the same period in internal medicine, female representation grew by 31%, in psychiatry 24%, and in pediatrics 12%. In these three specialties, the percentage of women in training ranges from a large minority to an overwhelming majority occupying, respectively, 42% of resident slots in medicine, 53.7% in psychiatry, and 70% in pediatrics. In none of these disciplines, however, has the rate of rise in female participation been as steep as in urology.
The progressive attractiveness to women of urology has occurred despite the recognition of challenges specific to their gender. More than half of current trainees have had to contend with male patients refusing to be seen by them, a significant minority report inappropriate treatment by male colleagues and patients, and >20% reported evidence of sexual harassment directed toward them by either male patients, male staff, or male colleagues.
The pattern of fellowship choice by the respondents may reflect both push and pull factors. Hostile attitudes and actions by male providers and patients may direct women to those areas in urology where contact with men would be lessened, or they may be assigned to such areas by more senior male urologists, a practice known as “pigeonholing.” There also might be a presumption that female urologists generally treat and desire to treat a patient base comprising primarily women. Despite these perceptions and difficulties, the reality is not monolithic, as not every woman urologist seeks to disengage herself from the more surgically related components of this specialty.
The practice of urology has broadened to include a spectrum of conditions categorized as female-specific disorders. Hence, such an expanding variety of patients offering opportunities to treat individuals of both sexes and all ages appears to be important to women medical students and residents in the choice of urology in general and fellowship opportunities in particular.
The experience of a female urologist is somewhat unique among the surgical specialties, in that it affords more possible interactions with men than are experienced by surgeons in general because of the preponderance of male patients in the specialty. Sexual harassment and discrimination, once sequestered from view by the attitudes of the press, administration, and the general public, has now been brought into the open in all fields of endeavors, including the various forms and formats of medical practice. Among female urologists in practice, Bradbury et al. 6 reported that 63% believed that gender discrimination affected their practice and 44% noted they were discouraged from choosing urology because of gender.
That gender-related instances of discrimination and even harassment remain prominent in perception and fact is validated by the responses in this survey. Many respondents were forthcoming with information about specific comments and incidents related to bad behavior by men toward them. Several reported alarmingly inappropriate comments about motherhood, pregnancy, and lack of physical stamina and the impact of each on professional performance and potential. One respondent noted in her comments that male coresidents have “complained that women should not be allowed to get pregnant during residency” and “should not be allowed to take maternity leave.” Another resident who reported being pregnant at the time of her participation in the survey recounted multiple inappropriate and even hostile comments made regarding her sex life and her “irresponsibility in not using contraception.” Another resident reported that “sexist comments/issues” were a “biweekly occurrence,” and get another reported having to contend with a pervasive assumption that “women are less dedicated” and stated that she has been “treated differently” as a result. Although such comments and attitudes by male patients and health workers cannot be abolished, their persistence should not be tolerated.
The study has several weaknesses. It is, therefore, informative but not definitive. The low response rate of 31% may be a result of the heavy work schedules of potential respondents and the fact that there was only one mailing. Our response rate was, however, identical to that of an analogous recently published survey of female radiology residents in which questions of discrimination and barriers to advancement were raised. 7 In addition, we speculate that women who had negative experiences related to gender may have been more likely to answer the questionnaire and provide written comments than those who did not.
This may have biased the results such that our population of respondants have an artificially higher likelihood of having had such experiences versus the general population of women urology residents.
We chose not to redistribute the survey to those who did not respond to the first mailing because we would then have to contend with the validity of responses obtained from previously reluctant residents. We conducted the survey via regular mail rather than online to overcome the possible concern that a respondent's identity could be revealed electronically.
The effect of the relatively new residency duty hour restrictions may also have an impact on the number of women choosing careers in urology. This was not specifically addressed in our survey. One might conclude that a perception among female medical students that the demands of a urology residency have been lessened by duty hour restrictions may make a career in urology more palatable to women. In order to reach this conclusion, however, one must also assume that women place a significant emphasis on lifestyle in choosing a specialty. This may not be the case, as our survey respondents cited many different factors as being important in this decision. Although we did not specifically seek information about the role of new duty hour restrictions in the choice to enter the field of urology, this may represent a very interesting area for future study.
Conclusions
At this juncture, rapid changes are taking place in the composition of members of urology training programs. Understanding the perspectives, concerns, and predilections of female applicants and trainees is essential to maximize the contributions women will make to the specialty and its patients. Meeting their expectations and taking measures to promote professional fulfillment will become increasingly important as representation of women in training programs and practice expands. Addressing and preventing instances related to gender discrimination and harassment should be central to the agenda of accommodation to women's needs and the enhancement of opportunities for them within the specialty.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.