
Abstract
Background:
Chronic fatigue syndrome (CFS) is a disabling illness of unknown etiology that is characterized by fatigue associated with a reduced ability to work, lasting for more than 6 months, and accompanied by a specific set of symptoms. The diagnosis remains difficult because of the absence of laboratory tests and is, therefore, made largely on the basis of the symptoms reported by the patient. The aim of this study was to analyze differences in blood nitrate levels in CFS patients and a matched control group after a physical exercise test.
Methods:
Forty-four consecutive female patients with CFS and 25 healthy women performed an exercise test using a cycle ergometer with monitoring of cardiopulmonary response. Blood samples were obtained for biochemical analyses of glucose, lactate, and nitrates at the beginning (under resting conditions) and after the maximal and supramaximal tests.
Results:
Plasma nitrates differed between the groups, with higher values in the CFS group (F = 6.93, p = 0.003). Nitrate concentration increased in relation to workload and reached higher values in the CFS group, the maximum difference with respect to the control group being 295% (t = 4.88, p < 0.001).
Conclusions:
The main result of the present study is that nitric oxide (NO) metabolites (nitrates) showed a much higher increase after a maximal physical test in CFS patients than in a group of matched subjects. This combination (exercise plus NO response evaluation) may be useful in the assessment of CFS.
Introduction
Chronic fatigue syndrome (CFS) is a disabling illness of unknown etiology 1 that is characterized by fatigue associated with a reduced ability to work lasting for more than 6 months and accompanied by a set of symptoms, including muscle and joint pain, neurocognitive disorders, and sleep perturbations. 2 –5 About 0.5% of patients attending general practice are identified as having CFS. 6
One theory about the etiology of CFS is that it is related to elevated peroxynitrite levels.
7
Increased levels of inflammatory cytokines, including tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), interleukin-6 (IL-6), and interferon-γ (IFN-γ), stimulate the production of elevated levels of inducible nitric oxide synthase (iNOS), which in turn synthesizes increased amounts of nitric oxide (NO). NO reacts rapidly with superoxide to form peroxynitrite, a potent oxidant. The elevated peroxynitrite and NO then impact the tissues involved, producing some of the symptoms of CFS.
8
Oxidative stress and NO have been proposed to play an important role in CFS pathophysiology.
9
Maes et al.
10
found that the production of cyclooxygenase-2 (COX-2) and iNOS was significantly higher in CFS patients than in normal controls, showing significant and positive intercorrelations between COX-2, iNOS, and nuclear factor-κβ (NF-κβ) and between COX-2 and iNOS on the one hand and the severity of illness on the other. NO, synthesized from
One of the problems with CFS is that it remains difficult to diagnose, as no laboratory test is available; the diagnosis is made largely on the basis of the symptoms reported by the patient. 12
Cardiopulmonary exercise testing is a valid procedure for determining functional capacity. Maximum oxygen uptake is a standard parameter to estimate a person's functional reserve. Exercise on a cycle ergometer or treadmill, where performance involves the lower extremities, is typically used to assess aerobic capacity. Several authors have reported decreased aerobic capacity in CFS patients compared with normal subjects, with reductions in maximum oxygen uptake (
The aim of this study was to analyze differences between CFS patients and a matched control group in blood nitrate levels (which presumably reflect NO production) and their correlation with the cardioventilatory response to a physical exercise test, evaluating the possibility of its application as a marker for CFS.
Materials and Methods
The CFS group comprised 44 female patients (mean age 46.5 ± 9.4 years) with a mean weight of 64.9 ± 11.3 kg, mean height of 1.62 ± 0.05 m, and mean body mass index (BMI) of 24.7 ± 3.5. They were referred consecutively to the Department of Physiological Sciences II of the University of Barcelona for a battery of examinations, and all were free of other diseases. They all met the Centers for Disease Control and Prevention (CDC) criteria for CFS, 2 and in each case, the diagnosis was confirmed by consensus between two physicians. Twenty-five healthy women (mean age 41.0 ± 8.6 years) with a mean weight of 63.8 ± 7.7 kg, mean height 1.61 ± 0.06 m, and mean BMI of 24.8 ± 3.4 served as the control group. The controls were considered to be sedentary subjects on the following grounds: their occupation did not require physical effort, they did not perform any special physical activity, and all their other activities (e.g., hobbies) were sedentary. Mean energy expenditure in the CFS group was 1.2 ± 0.1 METS/h during the day and in the control group 1.3 ± 0.1 METS/h during the day, expressing the energy cost of daily physical activity in both groups (by convention, 1 MET equals 3.5 mL O2/kg/min or, equivalently, 1 kcal or 4.184 kg/h).
All participants were fully informed of the procedures, the possible discomfort associated with the test, and the risks involved in performing the examinations. The study was approved by the Ethics Committee of the Research Institute of Bellvitge Hospital (IDIBELL-Bellvitge Campus, University of Barcelona). Written consent was obtained from all subjects after they had been informed of the procedures to be used and the risks entailed.
Laboratory exercise tests
Exercise testing was done in the laboratory of the Department of Physiological Sciences II at a room temperature of 22–24°C and relative physical humidity of 55%–65%. Subjects were instructed not to perform any intensive physical activity during the 72 hours prior to testing. All tests were conducted in the morning after a light breakfast. Participants were tested on a precalibrated cycle ergometer (Excalibur, Lode) starting at 0 W for 4 minutes. After this period, they followed a progressive exercise schedule that increased in ramp by 20 W every minute up to exhaustion, which was the maximal test. After a recovery period of 4 minutes, the subjects performed a personalized supramaximal test, initially without load; the workload was then increased in ramp every 30 seconds with a load corresponding to the maximal value achieved in the previous test (maximal test) up to exhaustion. (Example: If the subject achieved 50 W in the maximal test, the workload would increase 50 W every 30 seconds in the supramaximal test. At 30 seconds, it would reach 50 W, at 60 seconds 100 W, at 90 seconds 150 W, and so on.)
O2 uptake and CO2 production were measured by an automatic gas analysis system (Metasys TR-plus, Brainware SA) equipped with a pneumotach and making use of a two-way mask (Hans Rudolph). Before each test, gas and volume calibration took place, according to the manufacturer's guidelines. Heart rate (HR) was monitored continuously using a pulsometer (Polar Accurex Plus, Polar Electro). Arm blood pressure (BP) was taken manually using a clinical sphygmomanometer (Erkameter 3000, ErKa). The rate of perceived exertion (RPE) 18 was recorded at rest and after the maximal and supramaximal tests.
An indwelling catheter (model BD Insyte-W, Becton Dickinson) was inserted in one of the antecubital veins. Blood samples were obtained for biochemical analyses (glucose, lactate, and nitrates) at the beginning, just before the start of physical test (the baseline condition), and at the end of the maximal and supramaximal tests during the first minute of the recovery period.
Blood nitrate determinations
Serum was isolated by centrifugation of blood. To avoid disturbances in nitrate determinations, protein in serum was eliminated by means of centrifugation at 10.00 g for 1 hour at −20°C using Millipore filters (10 or 30 kDa molecular weight cutoff filter); samples were always kept at low temperatures. Nitrate determinations were performed using the nitrate/nitrite assay kit (Cayman Chemical); in these assays, nitrates were converted to nitrites using incubations with nitrate reductase and cofactors for 3 hours in the dark. Measures were taken by evaluating the fluorescence of the reagent ç (DAN) (2,3- diaminonaphthalene). Blood nitrate determination yielded R2 = 0.9992 between absorbance and nitrate concentration. Our laboratory repeated the analysis of 12 samples to evaluate the method's reproducibility and found a very high agreement (R2 = 0.9988, p < 0.001).
Statistical analysis
The Kolmogorov-Smirnov test was applied to establish the normal distribution of the different samples. Repeated measures ANOVA was then used to assess the differences between the two groups at different time points (rest, maximal test, and supramaximal test). An independent Student's t test was performed to assess group differences. The area under the receiver-operating characteristic (ROC) curve (AUC) was calculated for nitrate values in both groups. The lack of previous studies on blood nitrate in exercise in CFS made it impossible to perform the sample size calculation.
The data are expressed as mean ± standard deviation (SD). A significance level of p < 0.05 was used. The statistical analysis was performed using SPSS v.16 (SPSS Inc.).
Results
In the maximal test, the CFS group achieved a lower maximal workload (77.4 ± 27.4 W) than the control group (132.6 ± 29.0 W) (p < 0.001). In the supramaximal test, the maximal workload in the CFS group was again lower (147.6 ± 60.9 W vs. 236.2 ± 53.9 W) (p < 0.001). The oxygen uptake pattern at the three time points (rest, maximal, and supramaximal) also differed between the groups, with lower values in the CFS group (F = 19.8, p < 0.001). The maximal peak of
Measures of CO2 production again showed different patterns in the two groups, with lower values in the CFS group (F = 27.9, p < 0.001). The maximal peak CO2 production was 41% lower in the CFS group (t = −6.95, p < 0.001): 1.13 ± 0.42 L/min in the CFS group vs. 1.93 ± 0.46 L/min in the control group.
Other parameters that differed between the two groups were maximal respiratory quotient during exercise (F = 13.3, p < 0.001), HR (F = 15.7, p < 0.001), lactate (F = 29.0, p < 0.001), and systolic BP (F = 8.6, p = 0.001), which were all lower in the CFS group. There were no significant differences in diastolic BP (Table 1).
CFS, chronic fatigue syndrome.
Plasma nitrate values were higher in the CFS group (F = 6.93, p = 0.003) (Fig. 1). These values increased 2.31 ± 1.11-fold with respect to resting levels in the CFS group, whereas in the control group, the increase was only 1.31 ± 0.43-fold (t = 3.37, p = 0.002) (AUC = 0.846, p = 0.001). The increase in nitrate concentration in relation to the test duration was higher in the CFS group, with a maximum increase of 218% (t = 4.09, p < 0.001) (AUC = 0.912, p < 0.001). With respect to oxygen uptake, the increase in nitrate concentration was again higher in the CFS group, with a maximum difference of 228% (t = 4.31, p < 0.001) (AUC = 0.881, p < 0.001). The increase in nitrate concentration in relation to workload was also higher in the CFS group, with a maximum difference of 295% (t = 4.88, p < 0.001) (AUC = 0.954, p < 0.001).
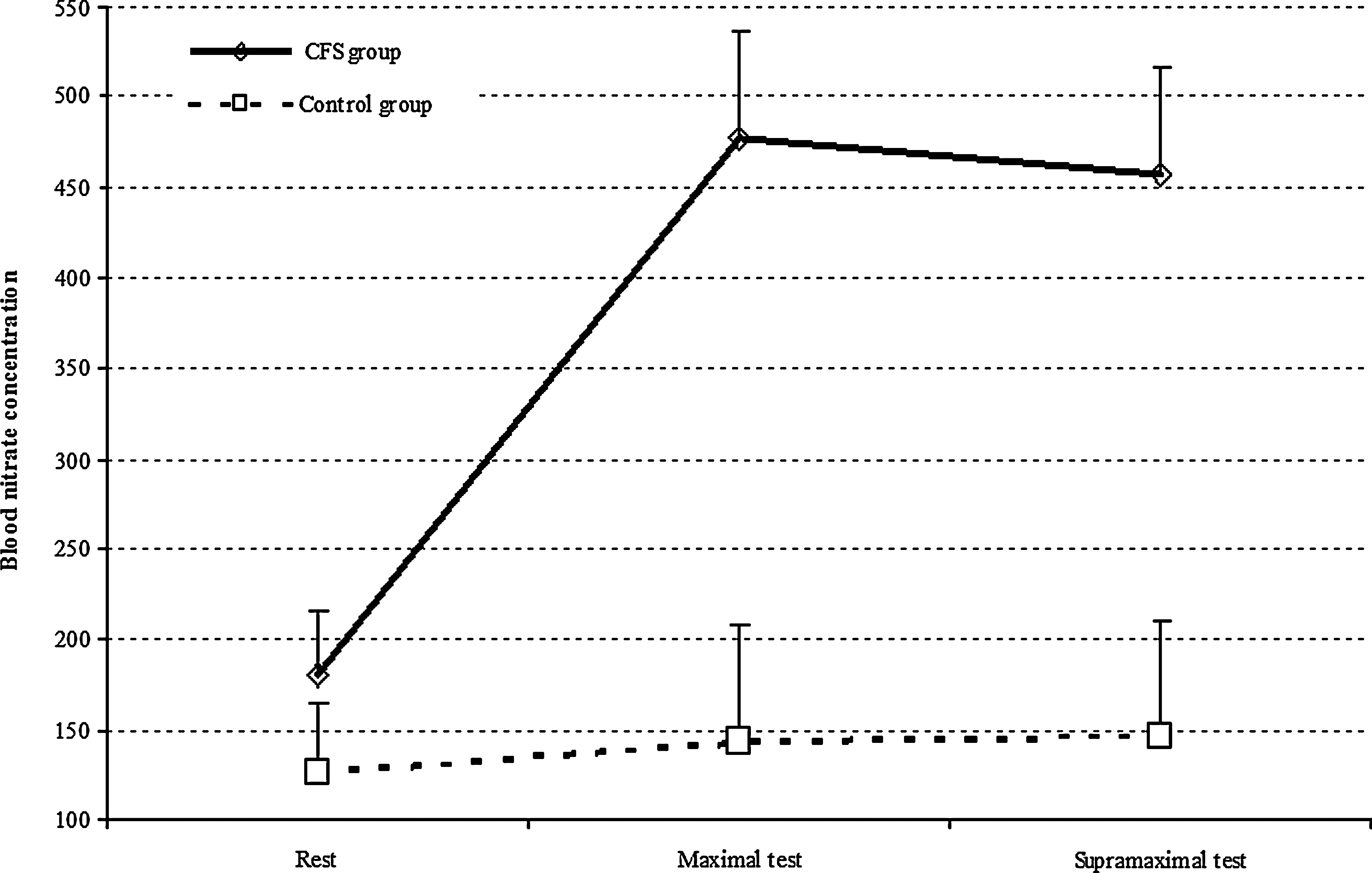
Values of blood nitrate concentrations (pmol NOx/ml) in the chronic fatigue syndrome group (solid line) and control group (broken line).
Discussion
The main result of the present study is that NO metabolites (nitrates) showed much higher increases after a maximal physical test in CFS patients than in a group of matched subjects, although there were no differences between the groups at baseline. The results of studies that involve maximal physical tests alone cannot be compared because these tests depend heavily on the subjects' characteristics, but this combination of stimulus by exercise plus NO metabolism responses may be useful in the clinical assessment of CFS.
The endothelium produces many paracrine substances, including NO.
19
NO is a labile, lipid-soluble gas that in endothelial cells is synthesized from
Other forms of NOS may not offer these physiological advantages to exercise response. For example, iNOS is induced primarily by reactive oxygen species (ROS) or inflammatory cytokines (IL-1, TNF, IFN-γ). After induction, iNOS remains active for 4–24 hours. The induction of high levels of iNOS increases NO levels 100 times more than does eNOS, raising levels of peroxynitrite considerably. Peroxynitrite reacts with and inactivates several enzymes in the mitochondria, leading to a dysfunction of mitochondrial and energy metabolism, with inhibition of mitochondrial electron transport. 25,26 Neuronal NOS (nNOS) is one of the subtypes in the central nervous system (CNS). Liu et al. 27 demonstrated that rats exposed to forced swimming for 4 weeks increased the number, area, and gray degree value of nNOS immunopositive neurons, suggesting that the increase in NOS expression may be closely related to the occurrence of chronic fatigue stress.
With respect to the assessment of physical capacity in CFS, several authors have reported a reduction in maximal oxygen uptake peak, 13 –15 whereas others have found aerobic performance to be at the lower end of the normal range. 28 These differences could be because the CFS population is very heterogeneous and that only a small number of subjects have been studied; the presence of comorbidity may also affect the results. Furthermore, kinesiophobia may be a factor of theoretical, clinical, and research relevance, for example, by reducing exercise performance on a cycle ergometer. 16 Another possible explanation for the different findings is what is termed the “hypoactivity syndrome” and its deconditioning-related effects on physiological responses. 14
It is difficult to include all these factors in a functional assessment for use in clinical practice. Here, we propose a very important stimulus (maximal effort) and analyze the biochemical response, a simple evaluation that can be applied to a large number of samples. Our study shows a lower power output capacity in the CFS group, as well as a lower peak oxygen uptake (33% lower than in the control group). It is true that the theoretical maximal effort, according to the classic criterion, is very difficult to achieve in CFS patients because of their reduced motivation or increased discomfort or pain. 29,30 It should be noted, however, that very often the cardiac and respiratory responses and lactate production in relation to the achieved workload do not differ from those of healthy sedentary people. The addition of a supramaximal test enabled us to confirm the peak oxygen uptake reached and to evaluate both the immediate recovery capacity and the impact of the first maximal effort. All patients performed the two workload tests. The difference reached between the groups in the maximal workload highlights the poorer functional capacity in the CFS group.
Only women were evaluated in this study, and the CFS group was diagnosed by two different physicians with extensive experience of the illness. The control subjects had no history of medical illness in the 3 years prior to the study, and they were considered sedentary if their occupation did not require physical labor and they did not perform structured physical activity. These restrictive criteria for sample selection were intended to optimize the homogeneity and comparability of the results.
The increase in NO metabolites after maximal exercise is not a voluntary response. In relation to workload, the increase in nitrate concentration in the CFS group was more than 2.5-fold greater than in the control group. At rest there were no differences between the two groups, but after the maximal and supramaximal exercise, the CFS group values increased significantly compared with those of controls. The control group performed a much longer exercise with a higher oxygen uptake and cardiac output, but in spite of this, the NO metabolite levels were much lower than in the CFS group. The physical exercise test by itself, without metabolite analyses, yielded controversial results, but when NO metabolites after maximal effort were analyzed, the responses showed considerable differences.
A limitation of the present study is that the sample comprised exclusively Caucasian women, thus preventing us from making any comparisons with men or with other ethnic groups. Future research is required with larger samples to assess the influence of different comorbidities and to establish clinical subgroups within the known heterogeneity of CFS. With respect to the methods, evaluation of different forms of NOS may help to explain the pathophysiology of this process. Further studies are needed to examine possible differences in response to submaximal (rather than maximal and supramaximal) exercise in CFS patients.
In conclusion, this study showed important differences in the changes in NO metabolites (nitrates) after exercise in a group of CFS patients and a control group. The very much higher values in CFS patients give an objective tool in the diagnosis.
Footnotes
Acknowledgments
This study was funded partially by a grant from the Fundación Mútua Madrileña (07PRIV009).
Disclosure Statement
The authors have no conflicts of interest to report.