
Abstract
Objective:
The aim of this research was to analyze gabapentin's effect on Pittsburgh Sleep Quality Index (PSQI) scores in menopausal women.
Methods:
Secondary analysis of data from a cohort of menopausal women participating in a randomized, double-blind, placebo-controlled trial of gabapentin 300 mg three times daily (TID) for hot flashes. The outcomes of interest were PSQI global and factor scores at weeks 4 and 12.
Results:
Subjects randomized to gabapentin demonstrated improvement in the sleep quality factor score, compared to placebo-treated subjects, at 4 and 12 weeks (p < 0.03). There was also gabapentin-associated improvement in the global PSQI score (p = 0.004) and the sleep efficiency factor score (p = 0.05) at 4 weeks. There was no significant effect of gabapentin on the daily disturbance factor score.
Conclusions:
Gabapentin may improve sleep quality in menopausal women with hot flashes. These results warrant further prospective investigation, with an emphasis on measuring subjective sleep quality and maintenance.
Introduction
Nearly two million women in the United States enter menopause every year. This life transition can be uncomfortable and disruptive to sleep. Approximately 40% of menopausal women experience sleep disruption, often in the form of difficulty with sleep initiation and frequent nighttime awakenings. 1,2 A recent review on sleep in women identified at least four causes of sleep disruption during menopause: sleep disordered breathing, mood disturbances, primary menopausal insomnia, and hot flashes. 3 Menopausal insomnia has been difficult to characterize with polysomnography. Many studies draw different and sometimes contradictory conclusions about the impact of menopause on sleep architecture; however, perimenopausal and menopausal women often have the subjective experience of disturbed sleep. 4,5,6
Traditionally, treatment for menopausal symptoms, including hot flashes, has relied on hormone replacement therapy (HRT). Results of the Women's Health Initiative, however, have demonstrated increased risk of breast cancer and cardiovascular complications in post-menopausal women using HRT. 7 Recently developed hypnotic agents have shown promise in treating perimenopausal insomnia; however, questions remain about the safety of long-term benzodiazepine agonist use. 8,9 Some antidepressants have also shown promise in controlling hot flashes, but responses are variable. 10
Gabapentin, a neurotherapeutic agent with several proposed molecular mechanisms, originally gained U.S. Food and Drug Administration (FDA) approval as an anticonvulsant. Many randomized trials have demonstrated its utility in other neurologic and psychiatric conditions, including chronic neuropathic pain. 11,12 More recently, the efficacy of this medication in relieving the number and severity of daily hot flashes in menopausal women was demonstrated in two double-blind, placebo controlled studies. 13,14 The mechanism of this action remains speculative. One of these trials measured sleep quality using the Pittsburgh Sleep Quality Index (PSQI) global score. 13,15 Despite gabapentin's ability to reduce hot flashes, this placebo-controlled trial did not demonstrate sustained improvement in PSQI scores. Since sleep disturbance is multi-factorial, however, the PSQI global score may not have reflected the complete impact of gabapentin on sleep.
Using recently developed PSQI factor scores, the purpose of this present study was to re-examine PSQI data from this placebo-controlled trial of gabapentin to explore gabapentin's effect on sleep in menopausal women. 13,16
Methods
Data for this investigation were taken from a previously published randomized, double-blind, placebo-controlled trial of gabapentin in 59 postmenopausal women who experienced 7–20 daily hot flashes. 13 The University of Rochester Research Subjects Review Board approved this study, and all participants provided written informed consent at the screening visit. In the double-blind phase of this study, subjects were treated with gabapentin or matching placebo and followed for 12 weeks; they then entered an open-label treatment phase. Subjects were randomized to receive either gabapentin, escalating to 300 mg three times daily (TID), or matching placebo TID during these 12 weeks.
The primary outcome variable in the trial was the percent change in hot flash frequency from baseline to week 12. Secondary outcome measures included changes in the PSQI global score. In this trial, PSQI data were collected at weeks 4 and 12. At week 4, there was a suggestion of a benefit of gabapentin on the PSQI global score (p = 0.01), but this benefit appeared to wane at week 12 (p = 0.09). Although the analysis of the primary outcome variable was performed according to the intention-to-treat principle and included all randomized subjects, the analyses of the secondary outcome variables (including the PSQI) excluded subjects who had missing data at the visit being analyzed. 13
The PSQI is a well-validated questionnaire that broadly measures sleep quality. It is commonly used in both research and clinical practice. The PSQI has 19 items that are translated into seven components, which are then combined to yield a composite, global score. 15
A recently published study validated a three-factor scoring model for the PSQI. 16 The authors performed exploratory and confirmatory factor analyses on the PSQI using data obtained from a sample of community-dwelling older adults with and without depression. They identified three factors that they characterized as sleep efficiency, perceived sleep quality, and daily disturbances. The components and factors of the PSQI are provided in Figure 1.
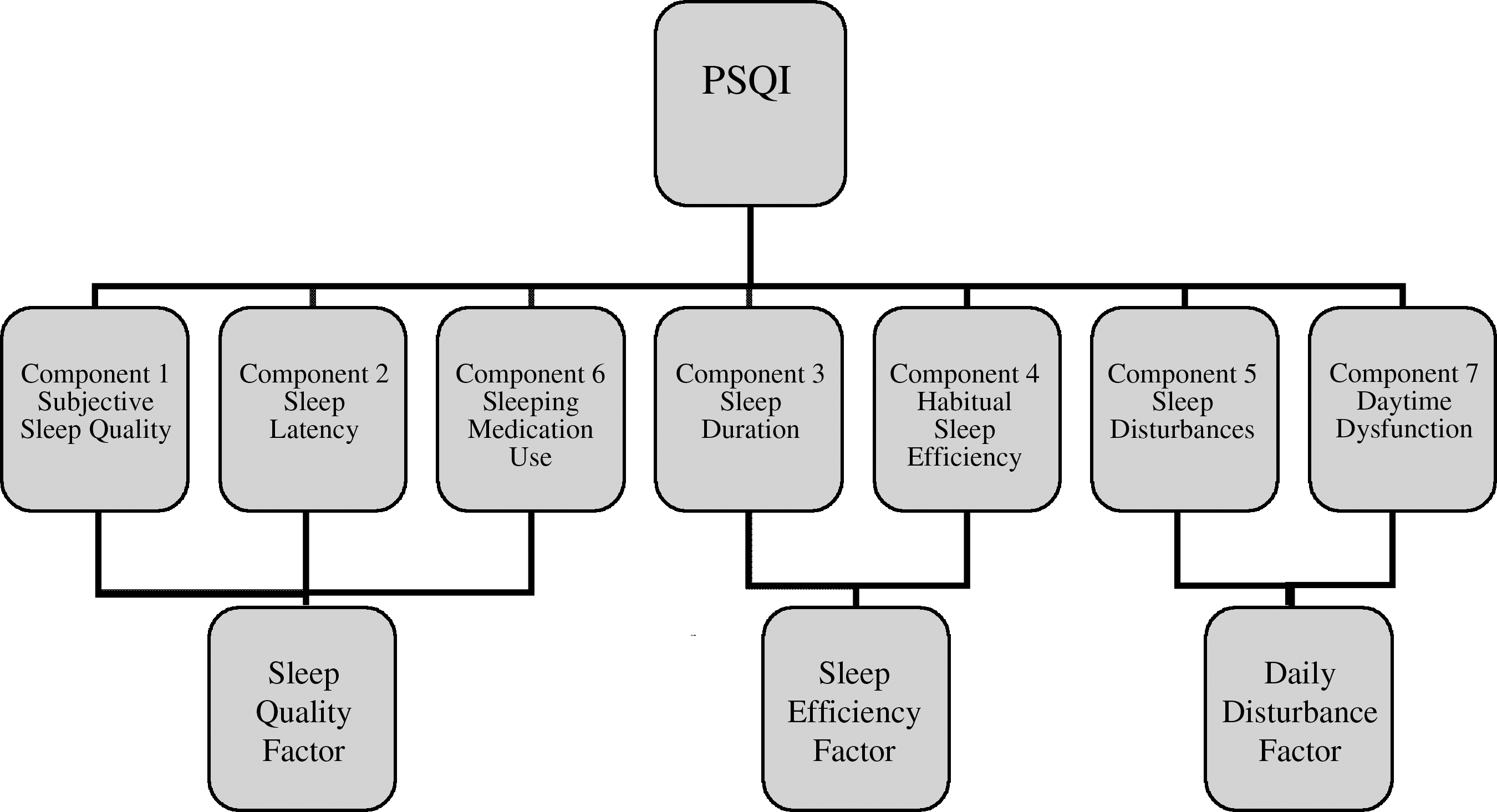
Pittsburgh Sleep Quality Index (PSQI) and its factors. (Adapted from Cole. 16 )
Statistical analysis
The PSQI global and factor scores were analyzed using a repeated-measures analysis of variance (ANOVA) model that included terms for treatment group (gabapentin, placebo), week (categorical), and the interaction between treatment group and week. This allowed estimation of the treatment effects (gabapentin–placebo) separately for each week, along with associated 95% confidence intervals. All available data from all randomized subjects were included in these analyses in accordance with the intention-to-treat principle, with maximum likelihood used to estimate the model parameters of interest in the setting of missing data. 17,18 An unstructured covariance matrix was assumed for model fitting. 19 These analyses were performed in SAS® (version 9.1) using the MIXED procedure.
Results
Baseline characteristics of the study participants are given in Table 1. The groups were generally comparable, particularly with regard to age, hot flash frequency and severity, and PSQI scores.
Values are mean (standard deviation) unless otherwise indicated. Daily hot flash composite score was calculated by summing the hot flash severity scores (subjectively rated on a 1–7 scale) and dividing by the number of days for which completed diaries were received.
PSQI, Pittsburgh Sleep Quality Index; SF-36, Short Form-36 Health Survey.
PSQI data were available at week 4 for 24–27 subjects (depending on the PSQI factor score) in the gabapentin group and 26–27 subjects in the placebo group. At week 12, PSQI data were available for 22–24 subjects in the gabapentin group and 25–26 subjects in the placebo group.
The estimated mean changes from baseline to weeks 4 and 12 in PSQI global and factor scores are presented by treatment group in Figure 2. Treatment effects (gabapentin–placebo) are summarized in Table 2. The mean improvement on the PSQI global score at week 4 was greater for the gabapentin group than for the placebo group (−3.37 vs. −0.81, p = 0.004). A similar pattern was seen at week 12, but the group difference was not statistically significant (−2.78 vs. −1.16, p = 0.07). The global improvement was reflected in the sleep quality and sleep efficiency factors. The mean improvement in the PSQI sleep quality factor was greater in the gabapentin group than in the placebo group at both week 4 (−1.50 vs. −0.33, p = 0.03) and week 12 (−1.27 vs. −0.28, p = 0.03). The mean improvement in the PSQI sleep efficiency factor was significantly greater in the gabapentin group than in the placebo group only at week 4 (−1.03 vs. −0.15, p = 0.05). No effects of treatment were apparent on the PSQI daily disturbances factor score.

Mean changes from baseline to weeks 4 and 12 in gabapentin versus placebo groups for global Pittsburgh Sleep Quality Index (PSQI) and factor scores. *p < 0.05, **p < 0.01.
CI, confidence interval.
Somnolence (20.0%), dizziness (13.3%), and rash with or without peripheral edema (6.7%) were the most common adverse events in the gabapentin group in the original trial. Onset of menses was more common in the placebo group (10.3%) than in the gabapentin group (6.7%). Fifty percent of subjects in the gabapentin group reported at least one adverse event, compared with 27.6% of subjects in the placebo group. Four subjects (13.3%) in the gabapentin group withdrew from the study (one each because of dizziness, rash, heart palpitations, and peripheral edema). One subject (3.4%) in the placebo group withdrew because of diarrhea. One subject in the gabapentin group temporarily decreased the dosage because of dizziness, and another did so due to sleepiness. 13
Discussion
This study demonstrates that gabapentin dosed at 300 mg TID may result in sustained improvement in sleep quality in menopausal women with hot flashes. Gabapentin was associated with improvements in the global PSQI score after 4 weeks of treatment; these effects tended to persist after 12 weeks of treatment. The improvements were reflected mainly in the PSQI sleep quality factor score. A short-term (4-week) effect on the sleep efficiency factor score was also noted. The results of this secondary analysis provide preliminary evidence that gabapentin may be an effective treatment option to improve sleep quality in menopausal women. Although other agents have been proven beneficial in treating menopausal insomnia, this analysis suggests benefit of this non-hormonal, non-hypnotic medication. 8,20 Sustained benefit of gabapentin on sleep quality in menopausal women has not been previously described.
The influence of menopause on sleep, particularly in the form of insomnia, has been well documented. 21,22 Subjective complaints of insomnia are common in this population, though consensus has not been reached on alterations in polysomnographic characteristics. 4,5,6,23
The study on which this secondary analysis was based demonstrated a significant improvement in daily hot flashes with the use of gabapentin. 13 It examined sleep quality in a prospective manner using the PSQI global score as a secondary outcome measure. Using a different method of statistical analysis (Wilcoxon rank sum test excluding subjects with missing data), the original study did demonstrate an improvement in the PSQI global score 4 weeks after initiating three times daily dosing of gabapentin, but not at the predetermined 12-week endpoint. These findings were confirmed in the current analysis. The PSQI has been well validated, but yields a composite score subject to a host of non-insomnia sleep paraphenomena like snoring, dyspnea, and nightmares. 15 The current analysis examined the PSQI and its three factor scores, and demonstrated a sustained gabapentin-associated improvement in the sleep quality factor, as well as suggestions of benefit on the sleep efficiency factor.
Independent from its beneficial effect on hot flashes, gabapentin's influence on sleep in normal, healthy individuals and in patients with epilepsy has also been demonstrated. 24,25 In general, polysomnographic recordings have demonstrated sleep “stabilization” with decreased light sleep and increased slow wave sleep and REM sleep. Gabapentin has not yet been demonstrated to improve variables that objectively reflect insomnia, such as sleep latency, wake after sleep onset (WASO) time, or early morning awakenings. Despite the lack of objective data, one known side effect of gabapentin is drowsiness. 26
In addition to its effects on hot flashes and sleep architecture, gabapentin has been demonstrated to have beneficial effects on some sleep conditions. For instance, gabapentin has demonstrated efficacy in treating restless legs syndrome (RLS), a condition that has been described in menopause. 27,28,29 The subjects in this trial were not screened for RLS, and it is possible that some of the subjects had improvement in sleep quality because of a corresponding improvement in RLS.
Based on these observations, gabapentin's impact on the sleep quality factor in menopausal women may reflect multiple mechanisms: improvement in hot flashes, “stabilization” of sleep architecture, or perhaps decreased sleep latency. It is also possible that gabapentin improved this factor by addressing unrecognized sleep pathology, such as RLS. The components that comprise the sleep quality factor (subjective sleep quality, sleep latency, sleeping medication use) do not shed sufficient insight to judge which of these potential mechanisms is most responsible for the effect.
In terms of molecular effects, not all of gabapentin's mechanisms have been identified. The compound binds to the α2δ subunit of the voltage-gated calcium channel and inhibits neuronal calcium currents in vitro. 30,31 It has been speculated that through a related mechanism, gabapentin might ultimately mitigate hypothalamic tachykinin activity in menopausal women, reducing hot flashes. 13 In relationship to sleep, it has been postulated that gabapentin may promote slow wave sleep by upregulating GABA in the central nervous system or through a serotonergic mechanism. 24 Again, since the mechanism through which gabapentin improves sleep quality is unknown, the molecular actions of the compound responsible for this effect are equally speculative.
Outside of the sleep quality factor, the other two PSQI factors (sleep efficiency and daily disturbances) appear less influenced by the proposed mechanisms, a conjecture that is supported by the absence of gabapentin-associated sustained improvement in these scores. Although the sleep efficiency score showed statistically significant improvement at week 4 of treatment, the improvement was not sustained at week 12. This factor is heavily weighted by subjective estimation of total sleep time, and it may be that gabapentin has relatively little impact on the perceived total amount of sleep. This may be unlike benzodiazepine agonists, which may yield some of their benefit on sleep through an amnestic effect. Components of the daily disturbances factor include questions regarding daytime “enthusiasm,” maintaining alertness, and breathing disturbances, among others. These questions do address common disruptors of menopausal sleep (including depression and sleep disordered breathing); however, gabapentin has little or no proven value in the treatment of these conditions. It is, therefore, not surprising that this factor remained unaffected by gabapentin treatment.
The PSQI includes a single question that specifically addresses nighttime arousals from feeling “too hot,” and this response makes up an exceedingly small portion of total PSQI score. Within the factor analysis, this question is included in the daily disturbance factor. Research tools that evaluate sleep quality and sleep maintenance (specifically, tools that measure vasomotor and sympathetic arousals) would be useful in measuring gabapentin's beneficial effect on menopausal sleep.
Limitations to this study include the fact that the PSQI was a secondary outcome variable in the original trial so the apparent improvement in sleep quality with this agent requires replication in a separate study. Second, there are considerations in regard to recruitment and baseline characteristics in the study. Women in the trial were recruited and enrolled based on the presence of hot flashes, and sleep disturbances were not required for enrollment. In addition, more subjects in the control group were taking raloxifen and fewer were taking antidepressants than those in the gabapentin group, and these agents might also affect hot flashes and sleep. Even with these considerations, however, both groups had similar baseline PSQI profiles. Third, the PSQI factor scores have been validated in a sample not limited to menopausal women, and the validation may not generalize to our population. 16 Notably, however, the validation was performed in a similarly-aged population. Lastly, the clinical trial on which our analysis is based examined TID dosing of gabapentin. In terms of examining sleep effects, every hour of sleep (Quaque Hora Somni [QHS]) dosing of gabapentin may be more appropriate.
Conclusions
In summary, this study provides evidence that gabapentin subjectively improves sleep quality in menopausal women with hot flashes. These results warrant prospective investigation, with an emphasis on measuring subjective sleep quality and maintenance, and with objective measurements of vasomotor sleep disruptions.
Footnotes
Disclosure Statement
Michael Yurcheshen states no conflicts of interest.
Thomas Guttuso is listed as the inventor of U.S. Patent 6,310,098, which is owned by the University of Rochester, covering the use of gabapentin and related compounds for treating hotflashes. The patent has been licensed to three companies.
Robert Holloway serves as a consultant for Milliman Guideline, reviewing neurology guidelines ($2000–4000 yearly). He is a chair for the Data Safety and Monitoring Board, National Institutes of Health ($400–600 year).
Michael P. McDermott receives 15% Salary Support from Medivation, Inc. for biostatistics work for Huntington's Disease research, and 20% Salary support from Boehringer Ingelheim Pharmaceuticals, Inc. for biostatistics work for Parkinson's Disease research.
Michael Perlis is the principal investigator (PI) in an investigator-initiated grant from Sanofi-Aventis Pharmaceuticals, studying long-term pharmacotherapy. He is also PI in an investigator-initiated grant from Cephalon Pharmaceuticals studying combined effects of cognitive behavioral therapy and alertness promoting agents. He is the site PI for several multisite trials with Sanofi, Aventis, Sanofi-Aventis, and Vanda. He has speaking Engagements with Sanofi-Aventis. He participates in directorships and management with Internet Didactic Services, and receives salary and distributions from the same. He has also consulted for Scientific Software Tools for compensation.
Acknowledgments
We thank Flavia B. Consens, M.D., Donald W. Greenblatt, M.D., and Joseph E. Modrak, M.D., for their input on manuscript submission.