
Abstract
Objectives:
Data on risk factors for major antenatal depression among African American women are scant. In this study, we seek to determine the prevalence and risk factors for major antenatal depression among low-income African American women receiving prenatal services through the Central Hillsborough Healthy Start (CHHS).
Methods:
Women were screened using the Edinburgh Postnatal Depression Scale (EPDS) with a cutoff of ≥13 as positive for risk of major antenatal depression. In total, 546 African American women were included in the analysis. We used logistic regression to identify risk factors for major antenatal depression.
Results:
The prevalence of depressive symptomatology consistent with major antenatal depression was 25%. Maternal age was identified as the main risk factor for major antenatal depression. The association between maternal age and risk for major antenatal depression was biphasic, with a linear trend component lasting until age 30, at which point the slope changed markedly tracing a more pronounced likelihood for major depression with advancing age. Women aged ≥30 were about 5 times as likely to suffer from symptoms of major antenatal depression as teen mothers (OR = 4.62, 95% CI 2.23-9.95).
Conclusions:
The risk for major antenatal depression increases about 5-fold among low-income African American women from age 30 as compared to teen mothers. The results are consistent with the weathering effect resulting from years of cumulative stress burden due to socioeconomic marginalization and discrimination. Older African American mothers may benefit from routine antenatal depression screening for early diagnosis and intervention.
Introduction
Depression is the most common mental health problem identified during pregnancy and following delivery. 1,2 In light of increasing racial disparities in birth outcomes and infant mortality, understanding the risk factors associated with maternal health issues, such as antenatal and postpartum depression, among disadvantaged African American women becomes crucial in the fight to improve the health of black women and their infants. Currently, research on antenatal depression among African American women is scarce. Most research addresses postpartum depression; however, there is increasing evidence that antenatal depression impacts maternal health and birth outcome. Accordingly, we undertook this study to identify risk factors for antenatal depression among African American women. In the general population, the prevalence rates for both antenatal and postpartum depression vary considerably, ranging between 10% and 52%. 1,3,4 The prevalence of pregnancy-related depression in disadvantaged populations has been consistently higher, however, with rates of antenatal depression as high as 41.7% reported for low-income women. 4 –6
Risk factors for antenatal and postpartum depression include young age, poverty, lack of education, history of depression, history of miscarriage or abortion, anxiety, low self-esteem, lack of social support, stressful life events, and history of abuse. 7 There is also evidence that women diagnosed with postpartum depression in their fist pregnancy are 50% more likely to develop the disorder in subsequent pregnancies or to develop depression that is unrelated to pregnancy. 8
African American and Hispanic women have the highest rates of antenatal and postpartum depression. 3,5 –11 Single marital status and low income have been reported as being predominant risk factors for postpartum depression among African American women. 6 Disadvantaged populations have been found to be more vulnerable to depression, as they have less control over their surroundings, are more likely to suffer stressful life events, 5,6 have less access to financial and emotional resources, and are more likely to have experienced discrimination. 11
Stress is a significant contributing factor to the onset of postpartum depression in African American women. 4,9 Mothers are often depressed because of medical conditions following delivery, including hypertension, infection, and recovery from surgery. 9 Loneliness and abandonment, as well as such external factors as financial difficulties, employment concerns, lack of social support, lack of support from a partner, and sibling care, may contribute additional stress, which culminates in fatigue associated with the accumulation of stressful circumstances. 4,9 Both antenatal and postpartum depression have been associated with an increased likelihood of developmental problems in infants of afflicted mothers. There is evidence that these infants are more likely to show signs of depression and stress and exhibit changes in brain activity that mimic the mother's prenatal depressive state. 12
The CDC estimates that as many as 50% of postpartum depression cases go undiagnosed. 3 Identifying pregnancy-related depression early is critically important in preventing postpartum depression and in improving birth outcome. In this study, we seek to identify factors associated with the risk for major antenatal depression among a low-income population of African American women.
Materials and Methods
The Central Hillsborough Healthy Start Project (CHHS) is one of the community-based programs in the State of Florida funded by the federal government through the Maternal and Child Health Bureau's Healthy Start Initiative. Implemented by the Lawton and Rhea Chiles Center for Healthy Mothers and Babies, the CHHS project functions as a community/university partnership to narrow racial disparities in maternal and infant health outcomes in urban Tampa neighborhoods (Florida), where the black infant mortality and morbidity rates are more than double those among whites (unpublished data from the Florida Department of Health). In these neighborhoods, most of the births are to mothers who are black, many of whom are young, unmarried, undereducated, and Medicaid eligible. 13 Prenatal and postnatal risk reduction services are provided by the project within the local perinatal healthcare system framework, the Hillsborough CHHS Program, and its overarching state system, the Florida Healthy Start Program. In collaboration with the Florida Department of Health and the Healthy Start Coalition of Hillsborough County, local and state efforts are integrated in a complementary manner. Unique to Florida, all pregnant women and newborn infants are offered risk screens to identify those who would benefit most from risk reduction services. Mothers who voluntarily accept the screen and express interest in services are referred to local Healthy Start Programs. In Hillsborough County, women living in select East Tampa ZIP codes (33602, 33603, 33605, and 33610) who need services are referred to the CHHS Program for those services.
Data collection
Data were collected through services provided by the CHHS program during the period 2002–2007. Florida's universal screening of pregnant women and infants was used to identify women at risk of poor outcomes. 14 Florida's universal screening of pregnant women and infants includes a series of questions that focus on medical, environmental, and psychosocial factors that identify a patient as at risk. The score is determined by summing the contributing items, each worth 1 point, except for race, which contributes 2 points. The following 15 variables comprise the components of the screening score: black race, maternal age <18 or >39, unmarried, less than high school education, low maternal weight (<110 pounds), problems keeping appointments, moving ≥3 times in the past year, feeling unsafe, going to bed hungry, tobacco use in the past 2 months, use of drug or alcohol in the past 2 months, unwanted pregnancy, current maternal illness, seeking prenatal care in the second trimester, and history of poor outcomes or no previous pregnancy experience. Women who scored ≥4 were considered at risk for adverse birth outcomes, which has been demonstrated previously. 15
Women were administered the Edinburgh Postnatal Depression Scale (EPDS) during prenatal visits. Measurements were conducted at different times during pregnancy, and the aggregate sum of EPDS scores from participating mothers was used to determine the prevalence of depressive symptomatology consistent with risk for antenatal depression. We believe that this is a better approach to capturing prevalence than administering the EPDS at a single point in time. The EPDS is a screening tool used to identify women at risk for antenatal and postpartum depression. It is usually administered at the 6–8-week postpartum examination, with a recommended readministration of the test after 2 weeks. The EPDS instrument has been validated for antenatal administration. 16 The EPDS has been validated and used cross-culturally throughout the world and has been administered numerous times to black women in the United States and England. 17 –20 The scale can only be used to indicate how the mother felt during the previous 7 days and is not intended to detect anxiety, phobias, or personality disorders. 21 Questions evaluate symptoms of depression, such as the inability to laugh, the inability to look forward to things with enjoyment, self-blame, anxiety and excessive worry, fear and panic, difficulty sleeping because of sadness, crying, and self-harm. 22 The maximum possible score is 30, with a cutoff point of 12/13 indicating that the mother is potentially suffering from major depression and a cutoff point of 9/10 indicating possible minor depression. 23 According to Cox et al., 21 the cutoff point of 12/13 results in a sensitivity of 86% and a specificity of 78%. A total of 724 women were administered the EPDS instrument prenatally. Of these women, 75.4% (n = 546) were African American. We restricted our analysis to African American women because of a paucity of numbers for the other racial/ethnic groups in the sample. The study is cross-sectional in design, as we did not follow participants over time.
Statistical analyses
We applied chi-square tests to determine differences in sociodemographic characteristics between mothers with EPDS scores compatible with risk of major depression vs. those with lower scores. We used chi-square tests for linear trend to assess dose-response. In order to determine predictors for risk of major depression, we constructed logistic regression models that contained the following covariates: maternal age (categorized as <20, 20–24, 25–29, and ≥30), body mass index (BMI) (<30 vs. ≥30), marital status (single vs. married), education (high school graduate vs. nongraduate), prenatal screening score (<4 vs. ≥4), and smoking (smoker vs. nonsmoker). Teens (<20) were used as a reference group to compare the risk of antenatal depression with maternal age. Variables were chosen based on previous research indicating their potential to impact depression during pregnancy. 24 –26
Because the analyses depicted a strong association between maternal age and risk for major antenatal depression, we constructed a receiver operator characteristics (ROC) curve to assess the predictive ability of maternal age in categorizing a woman in the study sample as being at risk for major antenatal depression. We performed this procedure using values generated from the adjusted logistic regression model with simultaneous computation of the area under the curve, the measure of accuracy. Similarly, we computed adjusted probabilities for major antenatal depression across maternal age and plotted the values to assess the trajectory of risk for major antenatal depression during pregnancy.
All tests of hypothesis were two-tailed, with a type 1 error rate fixed at 5%, and SAS version 9.1 (SAS Institute, Cary, NC) was used to perform all analyses. This study was approved by the Office of the Institutional Review Board at the University of South Florida.
Results
Of the 546 women in the study, 137 had EPDS scores consistent with risk for major depression (25.0%). Table 1 presents a summary of the results of crude frequency comparisons between women at risk for major depression vs. those not at risk with respect to selected sociodemographic characteristics. There were significant differences between women with risk of major antenatal depression vs. those not at risk with respect to maternal age. The risk for major antenatal depression correlated positively with maternal age in a dose-effect fashion (p for trend <0.01). However, the prevalence of marital status, education, BMI, prenatal screening score, and smoking during pregnancy did not differ between the two maternal groups.
The mean EPDS scores steadily increased by age group, with women <20 years having a mean EPDS score of 7.5, those aged 20–24 having a mean score of 7.7, those aged 25–29 having a mean score of 9.9, and women ≥30 having a mean score of 11.1. The mean EPDS score for the entire study sample was 8.4.
Table 2 shows the results of the logistic regression analysis used to generate the odds ratios (ORs) for maternal age and other risk factors associated with antenatal depression. Model I includes screening score in the analysis, whereas model II does not. Prenatal screening score and maternal age were significantly associated with elevated risk for major antenatal depression in model I. The strongest association was with maternal age, which demonstrated a monotonic increase in risk for major antenatal depression in a dose-effect pattern (p for trend <0.01). The association observed for maternal age was not impacted by the inclusion/exclusion of screening score in the analysis. As compared with teenagers, the risk for major antenatal depression was more than doubled among women aged 25–29 years (OR = 2.25, 95% CI 1.19-4.27) and almost quintupled by the time African American women reached the age of 30 and beyond (OR = 4.62, 95% CI 2.23-9.55). Results of further analysis using adjusted probabilities to assess this dose-response relationship are illustrated in Figure 1. The observed trend between maternal age and possible antenatal depression appeared to be biphasic, with age 30 being a critical point in time when the risk of antenatal depression became more pronounced and maintained a much greater level of risk there and beyond.
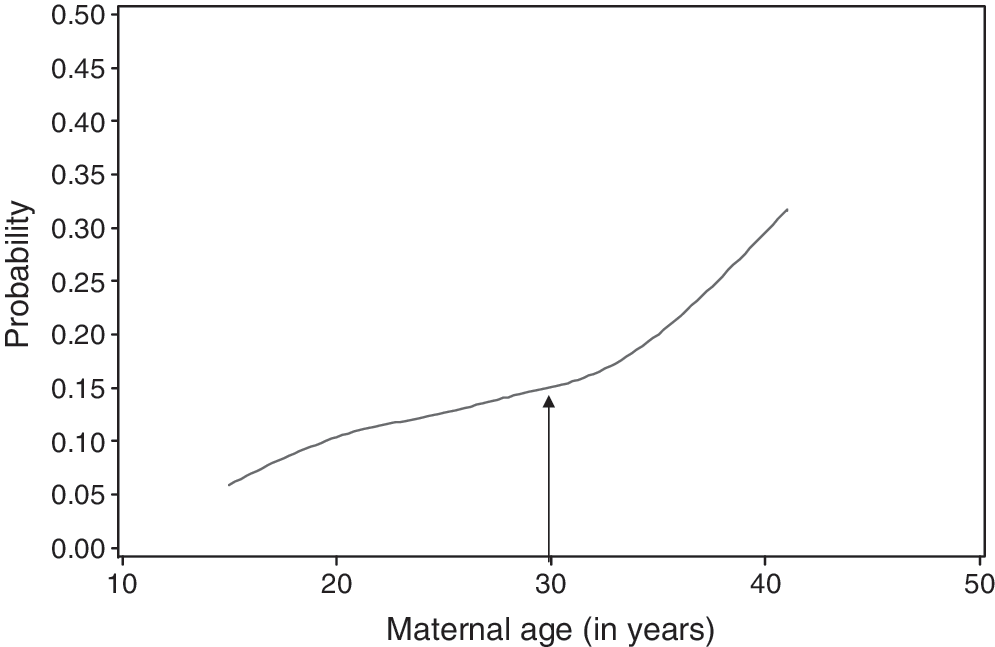
The probability of risk for antenatal depression across maternal age.
p for trend for age.
OR, odds ratio. Adjusted ORs were obtained by controlling for the confounding effects of the following characteristics: BMI, smoking, marital status, education, prenatal screening score and age; CI, confidence interval.
The ROC curve in Figure 2 highlights the predictive ability of age in determining a woman's risk of developing major antenatal depression. An accuracy rate of 60.4% was established, indicating that maternal age is a fairly good predictor of risk for major antenatal depression.
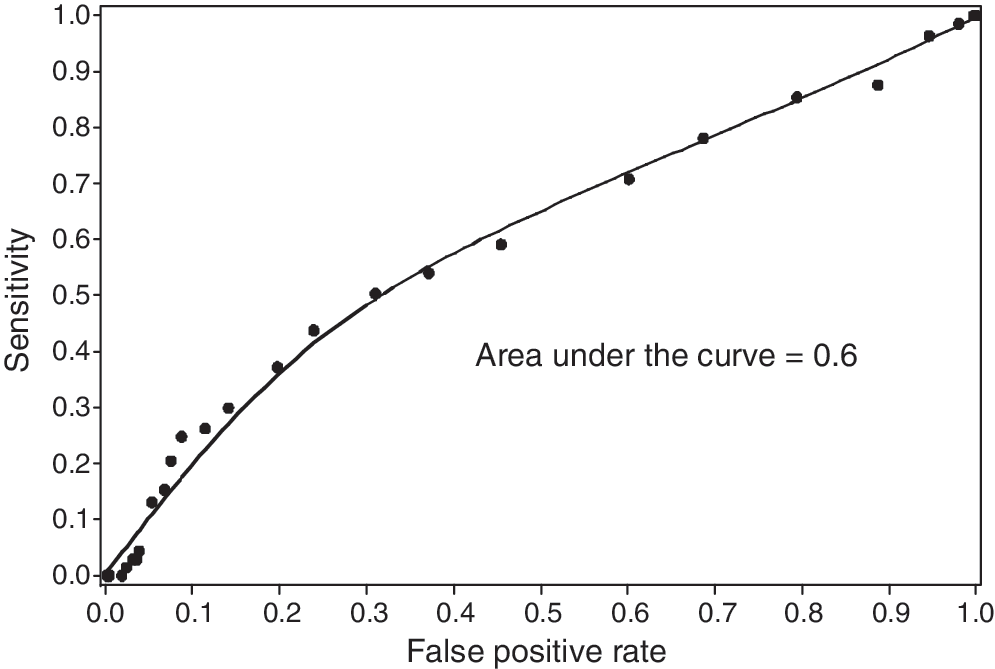
ROC for maternal age as a predictor of major antenatal depression.
Discussion
We found up to 25% of women in this study to be at risk for major antenatal depression. This result is consistent with previous research on antenatal depression in women of low socioeconomic status. 4 –6,10,27 However, as only women at risk for major depression were of interest or counted as cases (and this implies that minor and moderate depression were noncases), the actual prevalence of depressive symptomatology in the study population must be much higher.
Our study contributes important new insights into the relationship between maternal age and depression. Our findings indicate that African American women's risk for depression increases with age. There is a distinct biphasic dose-response relationship that notably increases in the 30s. A shocking 47.5% of women in the 30 and older age group experienced depressive symptomatology consistent with major antenatal depression. Older women were about 5 times more likely to be at risk for major antenatal depression compared with teen mothers. Previous research has reported teenage mothers as being a high-risk group for depression, 7 and to our knowledge, there is no known documented research indicating that older women are at a greater risk for antenatal depression. However, our findings are consistent with the weathering effect hypothesis, which posits that the long-term cumulative exposure to stressors adversely affects the mental and physical well-being of African American women. 4,28 –36 The Life Course Model also provides a rationale for the observed effect by postulating that experiences accumulated from birth and throughout the life span significantly alter the trajectory for health and well-being. 37 Women in this study came from disadvantaged backgrounds and had limited financial resources. Approximately 45% did not graduate from high school, and close to 91% were single throughout their pregnancy.
The weathering effect theory and Life Course Model suggest that exposure to repeated negative life events with age might explain why older African American women are more susceptible to poor mental health, in this case, antenatal depression. There is evidence that chronic stress caused by poverty and perceived discrimination causes higher rates of respiratory illness, hypertension, chronic illness, anxiety, depression, and psychosis. 28,33 Among African Americans, the odds of experiencing an adverse health event that limits work ability increase by 158% with each decade of life. 28 Research has shown that after the age of 26, African Americans are 24% more likely than Caucasians to suffer a health-related event. 28 By age 35, African Americans experience health conditions that are on average more commonly diagnosed in 55-year-old Caucasians, 29,31 and by age 46, African American women have the highest probability of health-related work limitations compared to any other group. 28
Most studies have reported a positive association among perceived discrimination, psychological distress, and a diagnosis of major depression. 28,31 –36 It has been found that 12% of African American women who had experienced a negative life event in the previous year and lived in high-stress neighborhoods went on to suffer a major depressive episode compared with 2% of women who had experienced a negative life event and lived in low-stress environments. 38 High rates of homicide in disadvantaged areas result in many women grieving the loss of a loved one. 4,31 They may be caring for a parent with a chronic illness or may be suffering ill health themselves. According to one study, being a caregiver, experiencing parenting strain, and not being married are most strongly associated with depressive symptoms. 39 In general, African American women in their 30s may have more children and are less likely to have financial support from their parents than women in their teens and 20s. 40,41 Older women may be raising preteen or teenage children without the presence of a father figure, which may act as an additional source of psychological stress. 40,42 Women who lack partners suffer greater financial hardships and struggle with the reality of raising additional children by themselves. 40 Given this premise, we hypothesize that the accumulated psychological stress from financial burdens, poor living conditions, poor health, negative life events, and perceived discrimination built up over the years cause the increased risk of major antenatal depression with age among disadvantaged African American women. Further research is needed to determine the cause of the observed effect, however, as many factors were not directly measured in this analysis. For example, African American women may not receive adequate healthcare or may have less access to positive social support. We recommend evaluating these measures in future research.
Study limitations include selection bias, which might have impacted the study results if unidentified differences (in addition to those adjusted for in the study) existed between younger and older women participating in the Healthy Start Program. Other limitations of the study include the fact that the EPDS is only a screening tool and cannot be used to diagnose antenatal or postpartum depression. As well, the EPDS can only measure depressive symptoms within the past week, which may miss the severity of depressive symptomatology at another point during pregnancy. Because of the variable sensitivity and specificity of the instrument, there is always the chance of obtaining false negatives or false positives, leading to misclassification bias that should reasonably be random across age groups. Consequently, the reported results in this study could have underestimated the observed association between maternal age and major antenatal depression. A history of depression is also an important risk factor for antenatal and postpartum depression and was not evaluated in this study. 1 Additional information about the course of depressive symptomatology over time could not be obtained because this was a cross-sectional study. Further research needs to be conducted to identify and confirm the factors responsible for the observed trend in maternal age and major depression in African American women. We recommend conducting a prospective cohort study to verify that lifelong stress and discrimination impacts maternal depression during pregnancy in older African American mothers.
Conclusions
As African American women age, they face an accumulation of adverse life events from poverty and discrimination that have a profound impact on mental well-being. Symptoms consistent with the weathering effect become apparent during pregnancy, as African American women aged ≥25 become significantly at higher risk of developing major antenatal depression compared with younger women. This finding has important implications for public health and social policies. Healthcare providers need to be aware of the increased risk of pregnancy-related depression in older African American women in order to better provide effective prenatal screenings and eventual optimal management for this population.
Footnotes
Acknowledgments
This work was supported in part by project H49MC00090 from the Maternal and Child Health Bureau (Title V, Social Security Act), Health Resources and Services Administration (HRSA), U.S. Department of Human and Health Services. The funding agency did not play any role in any aspect of the analyses.
Disclosure Statement
The authors have no conflicts of interest to report.