
Abstract
Objective:
To study the influence of socioeconomic variables, lifestyles, and sexual behaviors on the prevalence of high-risk human papillomavirus (HR-HPV) infection in female sex worker (FSW) according to their geographic origin in Alicante, Spain.
Methods:
This is a cross-sectional study of 549 FSW attending an AIDS information and prevention center from May 2003 to December 2004. Face-to-face interviews were carried out. HR-HPV was determined through Digene HR-HPV Test. Hybrid Capture II-positive samples (Digene Corp., Gaithersburg, MD) for PCR were directly sequenced. Data were analyzed using multiple logistic regression.
Results:
HR-HPV prevalence was 28% in Spaniards, 32% in Latin Americans, 32% in Eastern Europeans, 16% in sub-Saharan Africans, and 65% in North Africans (p = 0.04). Lower HR-HPV prevalence was associated with higher age, higher education, and higher body mass index (BMI) (p values for trend <0.05). In multivariate analyses, the effects of geographical origin, age, and education were maintained, together with time in sex work; women engaged for >1 year had a lower HR-HPV prevalence (OR 0.57, 95% CI 0.36-0.91) compared with those engaged <1 year. HR-HPV-16 was the most common type (n = 23, 24%), followed by HR-HPV-18 and HR-HPV-31, (n = 11, 11%), respectively.
Conclusions:
HR-HPV prevalence is very high in FSW and varies by geographic origin. Women of younger age and lower education level and those engaged in sex work for <1 year showed the highest prevalence, making them a priority group for cervical cancer prevention programs.
Introduction
Female sex workers (FSW) from western countries have a higher prevalence of high-risk human papillomavirus (HR-HPV) than women from the general population. 1 –8 Spain has one of the lowest HR-HPV prevalences worldwide, 1,9 but the few studies on HR-HPV infection among FSW show prevalence is high, similar to that published in other settings. 3,8 A very large proportion of the women who sell sex in Spain, similar to what has happened in the rest of the European Union, originate from developing countries, and many come from Central and South America, where HR-HPV prevalence and cervical cancer incidence are high. 2,10
The increased risk of HR-HPV observed in FSW has been attributed to a high number of sexual contacts with clients and to unsafe sex behavior with them, but the role of other factors, such as socioeconomic indicators, lifestyles, and sexual behavior with their private sexual partners, has seldom been studied. Kjaer et al. 6 found an association between HR-HPV prevalence and the number of private sex partners in a study of 188 Danish FSW. Other authors, mainly working in HIV epidemiology, have described how unsafe sex behavior is much more common with private partners than with clients. 11 –14
FSW, particularly migrants, are a group of women who are particularly vulnerable to HR-HPV infection and its consequences, but no in-depth studies have characterized their socioeconomic and working conditions, their commercial and noncommercial sexual behavior, and how these variables influence HR-HPV infection. In this article, we aim to answer these questions, and we hypothesize that prevalence and risk factors for HR-HPV may vary according to the geographic origin of the women. Our objective is to study the influence of socioeconomic variables, lifestyles, and sexual behaviors on the prevalence of HR-HPV infection in FSW according to their geographical origin.
Patients and Methods
A cross-sectional study of FSW attending a Centre for Information and Prevention of AIDS (CIPS) in Alicante, Spain, from May 2003 to December 2004 was carried out. The CIPS was created in the mid-1980s and is free of charge to all subjects irrespective of their nationality or legal status. From 1986, a specific outpatient clinic for commercial sex workers was set up to prevent, diagnose, and treat sexually transmitted infections (STIs). All FSW were invited to participate in the study, and the refusal rate was very low. Verbal informed consent was obtained from all the women. Ethics clearance for this study was obtained.
An ad hoc questionnaire of approximately 45 minutes duration was designed to collect information through a face-to-face interview conducted by a physician. The questionnaire included information on sociodemographic characteristics, reasons for attending the clinic, sexual practices in commercial and noncommercial contacts, time work in sex and social and work conditions, reproductive health, use of contraceptive methods in commercial and noncommercial contacts, and past history of STIs and hepatitis. An HIV test with informed consent was requested. Additional information about private partners was also collected (country of origin, use of intravenous drugs, and HIV status). Information about condom use was collected by asking the frequency of condom use in the last month through a Likert scale that ranged from 1 (never) to 5 (always). For the purpose of the analyses, this was classified in three categories: 1 (never users), 2/3 (occasional users), and 4/5 (frequent users). Frequency of condom accidents was asked as follows: Have you had a condom accident with a client within the last 3 months? If yes, how many? This was further classified as none, one, or more than one. The number of contacts with clients in the last year was calculated by multiplying the self-reported number of daily clients by the number of self-reported working days in the last year and classified in two groups according to the median value. The body mass index (BMI) was calculated with self-reported weight and height (BMI = kg/m2) and classified according to guidelines from the National Institutes of Health (NIH).
HR-HPV DNA detection and type assignation
Cervical samples were collected with a cervical brush and placed in 1 mL of Specimen Transport Medium (Digene Corporation Gaithersburg, MD), sent to the Retroviruses and Papillomavirus Laboratory of the National Centre for Microbiology in Madrid, and stored at −20°C until required for testing. HR-HPV infection was determined through the Digene HR-HPV Test, Hybrid Capture II, HC2 using the HR-HPV probe B cocktail, which identified types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68 in accordance with the manufacturer's instructions. All HC2-positive samples were typed by PCR and direct sequencing. DNA was extracted from cells recovered from a 200 μL aliquot of the residual HC2 denatured sample stored at −20°C (for 18–24 months). The quality of the DNA sample was tested with amplification of the β-actin gene. The samples successfully amplified were considered optimal for HPV typing. PCR amplification was carried out using MY09/MY11 general consensus primers. 15 Negative PCR samples were retested in a different PCR system (GP5+/GP6+) 16 in order to increase the positive rate of HPV type detection. The nucleotide sequences obtained were aligned with the reference sequences of different HR-HPV types from the Los Alamos sequence and GenBank database using the Clustal X program. HR-HPV type assignation was accomplished by phylogenetic analysis. (PHYLIP v3.5).
Statistical methods
Univariate analyses of demographic and clinical differences were conducted using appropriate methods. Trend score tests were used. Multiple logistic regression was used to study the relationship between HR-HPV infection and the explanatory variables. A significance level of <0.1 was chosen to select the variables entering the multivariate logistic regression model. Interaction terms between geographic origin and all variables entering the regression analyses were checked for. We used likelihood ratio tests and Wald tests to derive p values. A multiple logistic regression model was built incorporating all variables from univaried analyses. A backward approach was chosen, and the variables included in the final regression models were those that maximized the likelihood values. We tested for linear relationships between ordered categorical variables and the log odds of infection by HPV. The shape of the relationship was assessed by comparing the models, assuming lack of and presence of a linear relationship between the variable and the log odds of infection through likelihood ratio tests. Stata 10 was used to carry out the analyses (Stata Corp., College Station, TX).
Results
The study included 549 women whose characteristics by geographic origin are described in Table 1. The largest group of women, 303 (55%), originated from Latin America (LA), 91 (17%) were from Eastern Europe (EE), 87 (16%) were Spanish (Sp), and 51 (9%) were from sub-Saharan Africa (SSA). The women from EE and the SSA were the youngest and more likely to be single; those from NA and Sp were the oldest and more likely to be separated/divorced or widowed. The women from EE had a higher level of education—19 (21%) had been to university, whereas 9 (53%) and 14 (16%) of the women from NA and Sp, respectively, had no formal education. Higher prevalences of smoking were observed among Sp (64%), EE (71.4%), and NA (53%) compared with SSA (16%). Intravenous drug use was present only among Sp (9, 10%) and LA (3, 1%).
A lower proportion of women from SSA (31.4%) and EE (27.5%) had health cards (grants access to free universal care) compared with 56% of the LA and 53% of the NA. Median age of first sexual intercourse was around 16 years for all groups except for SSA (17.5 years). Nearly 90% of the women from SSA had a current regular partner, this proportion being around 60% for Sp, NA, and EE.
There were an important number (44%) of missing data on HIV infection. HIV prevalence was higher in Sp women, 8 (24.6%), and women from SSA, 4 (14%). Information on the HIV status of the current partner was available in 26% of the women; 20% of the current partners of the Sp FSW were HIV positive. The great majority of the women started to sell sex in Spain. Thirty (59%) and 15 (17%) of the SSA and the Sp, respectively, worked in the street. Half of the LA and EE and 65% of the NA worked in clubs. Median time work in sex was longer in Sp (11 years) and NA (8.5 years). The median number of daily contacts with clients was 5 for women from LA, 3 for NA, and 4 for the other geographic origins. Median number of yearly contacts with clients was 1056, and its interquartile range was 720–1500.
Over 90% of the women reported penetrative vaginal sex with either regular partners or clients in the last 10 sexual contacts, but whereas use of condom was high with clients, it was very low with regular partners (Fig. 1). Condom use with clients was lower among Sp compared with women from other countries, but condom use with regular partners was more frequent (31%) among Sp FSW and very uncommon in LA FSW (7%) (Fig. 1). Reported condom accidents in the last 3 months with clients were high, around 50% ranging, from 39% in SSA and EE to 63% in Sp (Table 1).
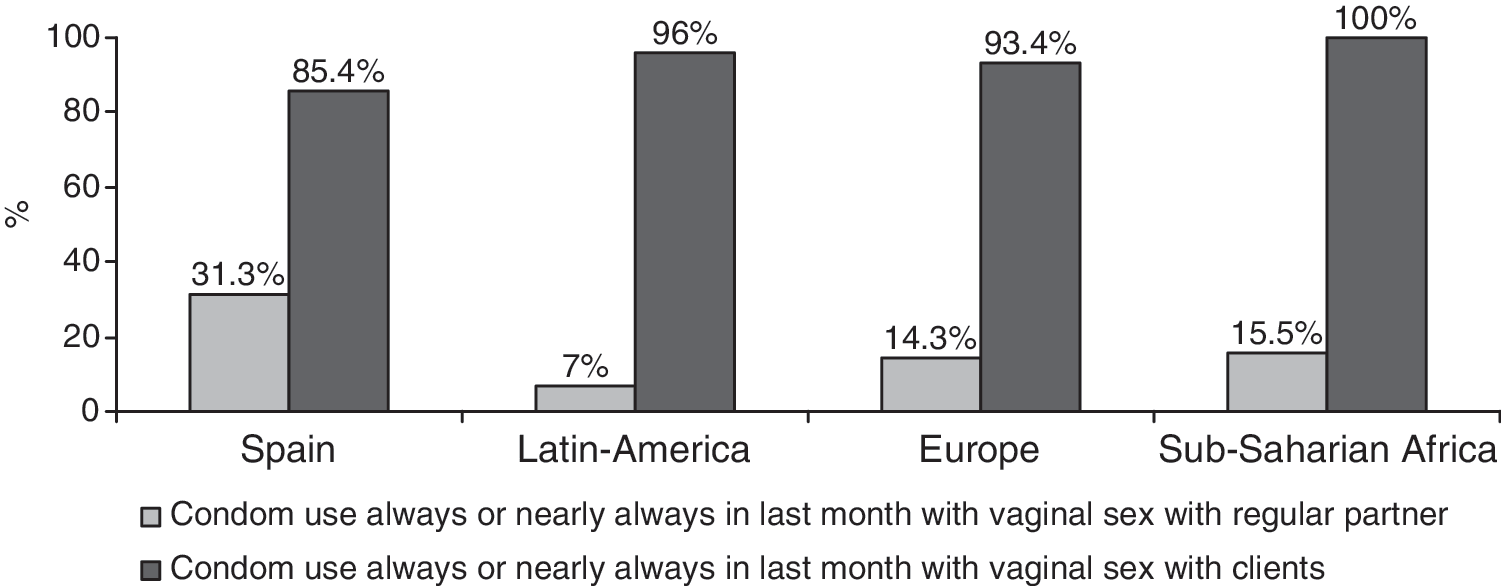
Frequency of condom use with regular partners and clients.
There were statistically significant differences (p = 0.004) in HR-HPV prevalence by geographic origin (Fig. 2). The highest HR-HPV prevalence was observed in FSW from NA (65%, 95% CI 38.32-85.79) and the lowest in women from SSA (16%, 95% CI 7.01-28.58). For the other three groups, HR-HPV prevalence was around 30% (Fig. 2). Lower HR-HPV prevalence was associated with higher age, higher education, and higher BMI (Table 2). The observed trends between overall HR-HPV prevalence and age, education, and BMI were statistically significant (p for trend 0.000, 0.026, and 0.013, respectively). The distribution of risk factors for HR-HPV varied by geographic origin (Table 2). HR-HPV prevalence in HIV-positive women from SSA was 75% compared with 8% among HIV-negative women (p < 0.05). For Sp women, HR-HPV prevalence was also higher in HIV-positive women (38%) compared with HIV-negative women (23%), although differences were not statistically significant (p = 0.2). Information on the HIV status of the regular partner was available from 25 Sp FSW; HR-HPV prevalence in those women whose partners were HIV infected was 80% compared with 10% in those with an uninfected HIV-positive partner (p < 0.05). Women who had engaged in commercial sex work for <1 year had a higher prevalence of HR-HPV (41%) than those who had been engaged in sex work for longer periods (27%). There were no differences in HR-HPV prevalence between women engaged in sex work for 1–2 years (28%), from 2–3 years (26%), and for >3 years (26%). There were no differences in HR-HPV prevalence according to condom use in the last month with neither the clients nor regular partners. For contacts with clients, HR-HPV prevalence was 36% in never users, 23% in occasional users, and 31% in frequent users. For regular partners, HR-HPV prevalence was 30% in never users, 27% in occasional users, and 30% in frequent users.

HR-HPV prevalence and 95% CI by geographic group.
p < 0.05; ** p < 0.10.
Multivariate analyses of the risk factors independently associated with HR-HPV infection are presented in Table 3. Age and educational level maintained the inverse associations with HR-HPV prevalence identified in univariate analyses. BMI lost its statistical significance (p = 0.11). However, the linearity tests for OR of the three variables, age, educational level, and BMI, were statistically significant. Women engaged in commercial sex work for >1 year had a lower HR-HPV prevalence (OR 0.57, 95% CI 0.36-0.91) compared with the reference group.
Stratifying by geographic origin in multivariate analyses yielded additional information in Sp women, as having an HIV-infected regular partner increased the odds of being HR-HPV infected (OR 14.13, 95% CI 1.3-150.6). Also, assuming the men with an unknown HIV status were HIV negative, the effect was maintained (OR 10, 95% CI 1.0-95.7). This effect was independent of the HIV status of the woman. In women from SSA, HIV-infected women were more likely than HIV-negative women to be HR-HPV-infected (OR 33, 95% CI 2.2-284.4). The number of yearly contacts with clients over 1057 increased the odds of HR-HPV in Sp women (OR 5.39, 95% CI 1.34-21.67), and reporting condom accidents with clients did so in LA women (OR 1.60, 95% CI 0.97-2.67).
A total of 169 samples were positive for HR-HPV, of which typing was possible in 97 (57.4%). In 12 samples (7.1%) HPV types were classified as nononcogenic or unclassified. Of the remaining 85 samples, HR-HPV-16 was the most common, accounting for 23 (24%), followed by HR-HPV-18 and HR-HPV-31, both of which accounted for 11 each (11%). The rest of the oncogenic HPV types accounted for 41 (42%) of the samples. The distribution of these proportions was similar across the different geographic origins, but numbers were low.
Discussion
The prevalence of HR-HPV infection in FSW is very high and varies according to the women's geographic origin. The highest prevalence was seen in women from North Africa (65%), the lowest in women from sub-Saharan Africa (16%). Women from Spain, Latin America, and Eastern Europe had intermediate values of HR-HPV prevalence, around 30%. In multivariate analyses, these differences by geographic origin were maintained. As well as the geographic origin differences, women of younger age, with a lower educational level, and those who had worked in commercial sex for <1 year had a higher HR-HPV prevalence.
Some of the risk factors for HR-HPV varied by geographic origin. Probably because of the small number of women and low HIV prevalence in women from geographic origins different from Spain and sub-Saharan Africa, HIV infection increased the odds of HR-HPV only in the women from sub-Saharan Africa. The HIV status of the women's noncommercial regular partner and the number of yearly contacts with clients increased the odds of HR-HPV only in the Spaniards. Latin American women reporting a higher number of condom accidents with clients had a higher HR-HPV prevalence compared with those who did not report any.
The high prevalence of HR-HPV observed in FSW is consistent with previous publications. 3 –8 Del Amo et al. 3 have reported that migrant FSW in Madrid had an HR-HPV prevalence of 39%, and it is noteworthy that FSW from sub-Saharan Africa also had the lowest prevalence, 29%, compared with 39% in Colombians, the largest group in that publication. The effect of age was consistent with the well-described pattern in that HR-HPV prevalence decreases with age. 17,18 This pattern has been largely attributed to acquired immunity in heavily exposed populations and to the immaturity of the cellular response in the cervix. 19 In women from the general population, a second peak around the menopause has been reported. 17 However, this pattern does not seem to be universal, and as described by Franceschi et al., 17 women who had been working as prostitutes for <1 year had a higher prevalence of HR-HPV than those who had been working for longer periods. For women who reported working as FSW for >1 year, there was no trend between time in sex work and HR-HPV prevalence. This effect was seen in women irrespective of their origin and may suggest an acquired immunity effect, similar to the one observed with age. We are not aware of this effect having been previously reported. However, interpreting time trends in cross-sectional studies has to be done with caution.
Having a very low BMI was associated with a higher odds of being HR-HPV positive, but it lost statistical significance in multivariate analyses. The association between BMI and HR-HPV infection is intriguing and has not been described before. Various explanations are plausible. Although the trend was maintained in analyses that adjusted for age and number of contacts with clients, the role of residual confounding secondary to client's preferences (youth and body shape) cannot be excluded. Another possibility is that nutritional deficiencies, such as folate deficiency, have been associated with HR-HPV persistence. 20 –23 Further studies are needed to confirm this finding. The effect of education on HR-HPV prevalence has been examined in women from the general population in different parts of the world. Some have found a protective effect of education, 24 –27 some have found no effect, and others, for example, Molano et al., 18 have reported an increased prevalence in women with a higher educational level. The effect of educational level in FSW has been less studied.
Being HIV positive increased by 33 times the odds of being infected by HR-HPV in women from sub-Saharan Africa, an effect that has been reported previously and has a biological basis. 28 –30 Immunodeficiency leads to higher persistence of HR-HPV in the cervix and increases the risk of intraepithelial lesions. Marais et al. 7 reported that 85% of the HIV-infected FSW from sub-Saharan Africa were HR-HPV positive compared with 42% among the HIV-negative women. The effect of the HIV status of the private sexual partner on the risk of HR-HPV infection of the Spanish women was remarkable, as it increased by 14 times the odds of the woman being HR-HPV infected. Caution has to be used in the potential misclassification here, as many women might not know about the HIV status of their partners and numbers were low. Although this effect has not been reported previously, it has various possible biological explanations: HPV prevalence could be higher in HIV-positive men, and immunodeficiency could lead to higher concentrations of HR-HPV on the epithelial surfaces. 31
A high number of contacts with clients was a risk factor for the Spaniards when using the median value as cutoff point; using other cutoff points showed similar effects for women from Latin America (data not shown). Juárez-Figueroa et al. 5 found an increased risk of HR-HPV associated with high number of contacts with clients. A very high proportion of FSW used condoms with clients, but the frequency of condom accidents was also very high, indicating an elevated number of high-risk exposures to HR-HPV. Condom accidents with clients was a risk factor for Latin American women but not for the other groups, where numbers were lower. As reported in previous studies looking at the risk of HIV infection, condom use with regular partners was very low. 11 Spanish FSW reported the highest use of condoms with their regular partners, but this was related to the high prevalence of HIV infection in these men. More information about the characteristics of the clients of these women would have been very interesting. Although we attempted to explore this by asking the women about the geographic origin of their clients, this was poorly answered. Qualitative research would be needed to address these aspects.
Although numbers were low when attempting to compare HR-HPV distribution, it is worth highlighting that HPV-16 was the most common type, followed by HPV-18 and HPV-31 in equal proportions. The few other studies that looked at HPV type distribution in FSW in Spain reported similar findings, 8,32 as have the few studies that have described HPV types in the general population. 1,9
Some of our analyses were clearly underpowered to estimate some associations after stratification by geographic area, and other analyses lack precision. Our sample size of FSW is, nevertheless, considerable. Some variables (number of contacts with clients, condom use) are prone to substantial misclassification, and some of the negative results could well be due to nondifferential misclassification. Also, for some variables, such as HIV infection or the HIV status of the partner, there was a high number of missing values, which makes interpretation less valid. Similar results were, nevertheless, maintained, assuming missing values were HIV negative.
In summary, FSW have a very high prevalence of HR-HPV, which varies by geographic origin. FSW have multiple risk factors for HR-HPV infection, some common and some specific to women from a given geographic region. These facts make these women a priority group for active follow-up and intervention within sexual health programs, particularly relevant to the migrant FSW who have not yet obtained their health cards. Regular cervical cancer screening is a must in this population. It is important to highlight the need to convey prevention messages to a personal sphere, that is, to their private partners as well as their clients, and to facilitate access to the health system for these women.
Footnotes
Acknowledgments
This study was supported by funds provided by the Generalitat Valenciana, Conselleria de Sanidad, DOGV and also by RIS, RD06/2006, and FIS 1055/07.
Disclosure Statement
The authors have no conflicts of interest to report.