
Abstract
Background:
Pregnant women who are placed on hospitalized bed rest experience increased antepartum-related distress. We sought to examine the efficacy of a single session music or recreation therapy intervention to reduce antepartum-related distress among women with high-risk pregnancies experiencing extended antepartum hospitalizations.
Methods:
In a randomized, single-blinded study, participants (n = 80) received 1 hour of music or recreation therapy or were placed in an attention-control group. Antepartum-related distress was measured by the Antepartum Bedrest Emotional Impact Inventory, which was administered before and after the intervention and at a follow-up period between 48 and 72 hours.
Results:
Significant associations were found between the delivery of music and recreation therapy and the reduction of antepartum-related distress in women hospitalized with high-risk pregnancies. These statistically significant reductions in distress persisted over a period of up to 48–72 hours.
Conclusions:
Single session music and recreation therapy interventions effectively alleviate antepartum-related distress among high-risk women experiencing antepartum hospitalization and should be considered as valuable additions to any comprehensive antepartum program.
Introduction
Recent advances in reproductive technologies (e.g., infertility treatments, more intensive pregnancy surveillance) have increased the likelihood of more viable pregnancies but also have increased the frequency of women being hospitalized for pregnancy complications before delivery. Such complications include preeclampsia, preterm labor, poor fetal growth, and placenta previa. Separated from her usual supportive network, the hospitalized antepartum patient with a high-risk condition must, at once, manage the emotional, physical, and social changes unique to pregnancy and attempt to cope with the emotional stress of her complication, compounded by the stress of hospitalization. By themselves, these and other high-risk conditions exacerbate normal anxiety about maternal health and the health of the fetus. 1 –3 Antepartum hospitalization has also been associated with increased levels of psychosocial distress, including anxiety, depression, stress, boredom, loneliness, feelings of loss of control, and powerlessness. 4 –10 Many studies have reported a positive relation between antepartum-related distress and increased nausea and vomiting, prolonged sick leave, more obstetrician visits, 11 increased planned cesarean deliveries and epidural analgesia during labor, 11,12 and adverse events in pregnancy and labor/delivery (e.g., spontaneous preterm delivery, fetal growth restriction, preeclampsia, and hypertension). 13 –17 Moreover, the severity of antepartum-related distress increases as the length of the hospitalization increases. 4,18 Despite these connections between antepartum-related distress and negative pregnancy outcomes, there is a paucity of research in the prevention and treatment of antepartum-related distress derived from the hospitalization experience.
One cost-effective stress reduction intervention that has been used frequently in hospital settings, 19 –22 including for women during pregnancy 23,24 and delivery, 25,26 is music therapy. Music therapy during pregnancy has been shown to slow respiratory rates, decrease stress and pain responses, 13,27 and improve relaxation responses. 28 Cassileth et al. 20 define music therapy as the controlled use of music to effect clinical change, and there is a wide variety of music therapy techniques designed to meet the needs of each patient. Based on a review of the Journal of Music Therapy, Music Therapy Perspectives, and Music Therapy from 1950 to the present, there appears to be only one published research study exploring the therapeutic effects of music therapy on hospitalized antepartum patients. Winslow 6 reported on a very small, qualitative case series of three hospitalized antepartum women with high levels of anxiety. Based on therapist observation, the author concluded that music therapy was used successfully to decrease anxiety. The effects of music therapy on patient populations other than antepartum women have been the subjects of considerable research.
A paucity of pregnancy-related experience also exists about the alternative intervention of recreational therapy. The American Therapeutic Recreation Association (ATRA) and the United States Department of Labor define recreation therapy as the utilization of leisure activities to foster autonomy across several areas of functioning, including emotional, physical, cognitive, and social domains. 29 As with music therapy, the literature on recreation therapy interventions in other populations (e.g., physical medicine, mental health disabilities, geriatric and pediatric populations) documents improvement in psychosocial health, including decreased depression, decreases in stress-related symptoms, decreased anxiety, a decreased sense of boredom and isolation, and an increased ability to cope with stressors related to hospitalization. 30,31
The purpose of this study was to examine the efficacy of a single session music or recreation therapy intervention in alleviating antepartum-related distress experienced by women with high-risk pregnancies on extended hospital bed rest. Based on previous research, we hypothesized that music and recreation therapy would be an effective intervention for reducing antepartum-related distress.
Materials and Methods
Participants and setting
This study took place at a large, Midwestern, suburban teaching hospital with a regional Perinatal Center with 26 private rooms on the antepartum unit. Before data collection, our research protocol was submitted to the Internal Review Board for review and approval. Participants were 61 pregnant women hospitalized with various high-risk obstetric health issues, including preterm labor, premature rupture of membranes, preeclampsia, and multiple gestations. Participants were all over the age of 18, between 24 and 38 weeks of gestation, who had not been hospitalized previously during this pregnancy, who were proficient in reading and writing English, whose length of hospital stay was unpredictable, and who had been hospitalized for at least 3 or 7 days. Originally, participants were eligible for the study only after they had been hospitalized for at least 7 days; at midstudy, however, we received IRB approval to decrease required hospitalization days to 3, as many more patients were being discharged to home bed rest after a few days based on stricter insurance protocols. Participants who were diagnosed with serious mental illness, who were vision or hearing impaired, or whose cognitive skills were so limited as to render consent meaningless were also excluded from the study.
Procedures
Once informed consent was obtained, participants were randomly assigned by the research coordinator (using a Random Numbers Statistical Table and opaque envelopes containing group membership) to an intervention condition (either a music or recreation therapy) or waitlist control condition. Because of this randomization protocol, there is a 2:1 ratio of control/music or recreation therapy participants. The participants were blinded to condition. We used an attention-control group to enable us to distinguish between decreased levels of distress caused by the interventions and those that might result from the nonspecific, supportive attention of the therapists. Moreover, this design allowed us to offer music and recreation therapy to the control group participants within a week from the date of consent. We believed it would be unethical to restrict potentially therapeutic interventions from patients during their entire hospitalization.
Participants in the experimental group received a visit in their hospital room from a board-certified music or recreation therapist within 24–48 hours. Variability in the intervention was minimized by attempting to keep the therapists constant. There were two music therapists and two recreation therapists; over the course of the 3-year study, some therapists left the program and were replaced by new ones. Therapists read from a standardized script, which briefly reviewed the nature of the study and provided directions for completing a self-report distress measure.
The distress measure was administered at three separate points: at a baseline meeting (Time 1), immediately after the intervention (or 1 hour after the baseline meeting for participants in the control group situation) (Time 2), and 48–72 hours after the intervention (Time 3). After participants completed the first assessment, the therapist read from a standardized script, describing music or recreation therapy, its potential benefits, and the available interventions. Participants then participated in a 1-hour music or recreation therapy intervention of their choice. Music therapists offered a range of interventions for patients, all within the current standards of care of these therapies. Specific interventions used for meeting the needs of antepartum patients included music-facilitated relaxation, active music listening, song writing, music for bonding, and clinical improvization. Of the music therapy options, the majority (>90%) of participants chose to participate in a music-focused relaxation intervention, in which live, improvised, nonvocal music (using either a harp or acoustic guitar) was paired with imagery and progressive muscle relaxation/breathing techniques of the participant's choice. Recreation therapy interventions offered included adaptive leisure activities, creative arts, community resource education, and leisure awareness activities. The majority (>90%) of participants receiving recreation therapy chose to participate in a creative arts intervention, in which the participant completed an independent craft project, for example, t-shirt painting or needlework. Table 1 lists the available music and recreation therapy interventions. At Time 3, the therapist requested the participant to complete some open-ended questions about positive/negative occurrences that had taken place since the therapist had last seen the participant. After the participant had completed this form, the therapist administered the third and final distress assessment.
In the attention-control group, participants received a visit from the same music or recreation therapist within 24–48 hours. The therapists read from the same standardized script, which very briefly reviewed the nature of the study and provided the directions for completing the assessment tool. Participants then completed the self-report measure. When the therapist returned 45 minutes later, participants completed the second assessment, and the therapist informed the participant that she would return in a few days to complete one final form. If asked, the therapist informed the participant that there was a waitlist for receiving intervention. Finally, the therapist returned at Time 3 for completion of an Intervening Variables Form. After the participant had completed this form, the therapist administered the third and final distress measure.
Measures
Sociodemographic and clinical forms
Demographic and clinical data were collected for each participant, including marital status, educational history, diagnosis on admission, length of hospitalization, and receipt of steroids and tocolytics. Information about these criteria was obtained from electronic patient records, nursing staff, and patient self-report.
Antepartum-related distress
Participants completed the Antepartum Bedrest Emotional Impact Inventory (ABEII). The ABEII is a brief assessment tool developed by the study authors to measure bed rest-related psychosocial distress, which includes items dealing with anxiety, loneliness/isolation, boredom, depression, stress, and loss of control (see item stems in the Appendix). Both research and clinical practice suggest that high-risk women who are hospitalized during their pregnancies experience increased levels of these symptoms. 4,32 However, no single self-report tool exists to measure these variables among antepartum women. The ABEII consists of 18 items that are summed to create a total antepartum distress score (higher score equals increased distress). The authors reviewed several related distress measures that have been used with hospitalized antepartum patients to generate a list of concepts and potential items: the Antepartum Hospital Stressors Inventory, 18 Hospital Anxiety and Depression Scale (HADS), 33 Perceived Stress Scale, 34 State-Trait Anxiety Inventory for Adults (STAI), 35 and the Edinburgh Postnatal Depression Scale. 36 From these scales, only 2 items were used in their entirity (“I get sudden feelings of panic” from the HADS and “I feel inadequate” from the STAI), with the remaining 16 items being written (using extensive clinical experience with antepartum women on bed rest, verbal reports from antepartum nurses, and a review of current literature) and modifying items from the scales mentioned to reflect specific circumstances of antepartum patients (see the Appendix for item stems of the ABEII). Next, we piloted and debriefed the items with a small group of hospitalized antepartum patients (n = 6), who first completed the ABEII and were then interviewed about its clarity, understandability, and relevance to their experience. Patients were also asked to make suggestions for changes, additional items, or deletion of items, which were incorporated in subsequent revisions. A final pool of items was reviewed for face and content validity by a panel of experts, consisting of instrument development specialists, mental health professionals, and nurses who were actively involved in the care of hospitalized high-risk antepartum patients, and also by women who had been high-risk antepartum patients. This was followed by additional modifications until a final item pool was agreed on. We estimated that the ABEII takes roughly 3–5 minutes to complete.
Data analysis
We used SPSS version 17.0 (SPSS, Inc., Chicago, IL) for all data analyses. After estimating internal consistency (Cronbach's alpha) and test-retest reliability coefficients on ABEII scores, we compared completers with those who were enrolled but dropped out either before or after the first assessment (using chi-square and independent samples t tests) to evaluate potential group differences on sociodemographic and clinical variables and baseline ABEII scores. Using the same statistical tests, we examined the success of random assignment by comparing treatment and control conditions on sociodemographic and clinical characteristics and baseline ABEII scores. Statistically significant variables were used as covariates in the model. We evaluated within-group change over time using paired t tests. Prior to testing the model, we also evaluated whether to include the following theoretically postulated covariates: total positive events during hospitalization (e.g., family member visits or phone calls, good news from M.D., news about discharge), total negative events during hospitalization (e.g., bleeding, postponed discharge, preterm labor, pain, contractions, postponed delivery), and use of tocolytics. Factorial repeated measures analysis of covariance (ANCOVA) was used to examine the effects of covariates in the model. We calculated Cohen's d effect size coefficients (M 1 − M 2 /σpooled) to estimate the relative magnitude of group differences. In the medical literature, effect sizes of 0.2–0.5 are considered minimally important in the measurement of health-related quality of life. 37 –39 Based on Cohen's recommendations, 40 we used the following guidelines to interpret effect size estimates: 0.01–0.14 = negligible; 0.15–0.44 = small; 0.45–0.79 = medium; ≥0.80 = large. This study was powered at 80% to detect a moderately large effect size (d = 0. 65) with an alpha ≤0.05.
Results
Sample characteristics
Table 2 lists characteristics of the participants. A majority of participants were Caucasian (59%), with a mean age of 31 years (range 18–43). Roughly 35% reported at least some college or more, and over half reported being employed (56%). The majority endorsed being married (83%) and being placed on partial bed rest (78%). The average length of hospitalization was 9.4 days (SD 4.4).
SD, standard deviation; ABEII, Antepartum Bedrest Emotional Impact Inventory.
Preliminary reliability and concurrent validity of ABEII
The Cronbach's alpha coefficient for the baseline ABEII was 0.90 and the r test-retest reliability coefficients (Pearson's r) ranged between 0.72 and 0.78, p < 0.01. Small, positive associations (r's = 0.31 and 0.36, p < 0.01) were found between the ABEII and gravida (total number of pregnancies in one's lifetime) and para (total number of births in one's lifetime), respectively.
Enrollment and random assignment
During 2003–2005, we identified eligible patients through chart review and nursing report. We enrolled a total of 136 patients (Fig. 1); once enrolled, however, 56 patients were unable to complete the study, and only 14 patients who dropped out finished the baseline ABEII assessment. The primary reasons for dropout once enrolled were delivery of one's baby (n = 24) and being discharged (n = 25). One person independently withdrew, and 6 patients left the study for unknown reasons. In the end, 80 subjects finished the study and provided complete data across all three time points. Conditions were distributed as follows: music therapy group (n = 19), recreation therapy group (n = 19), and control group (n = 42) (Fig. 1).
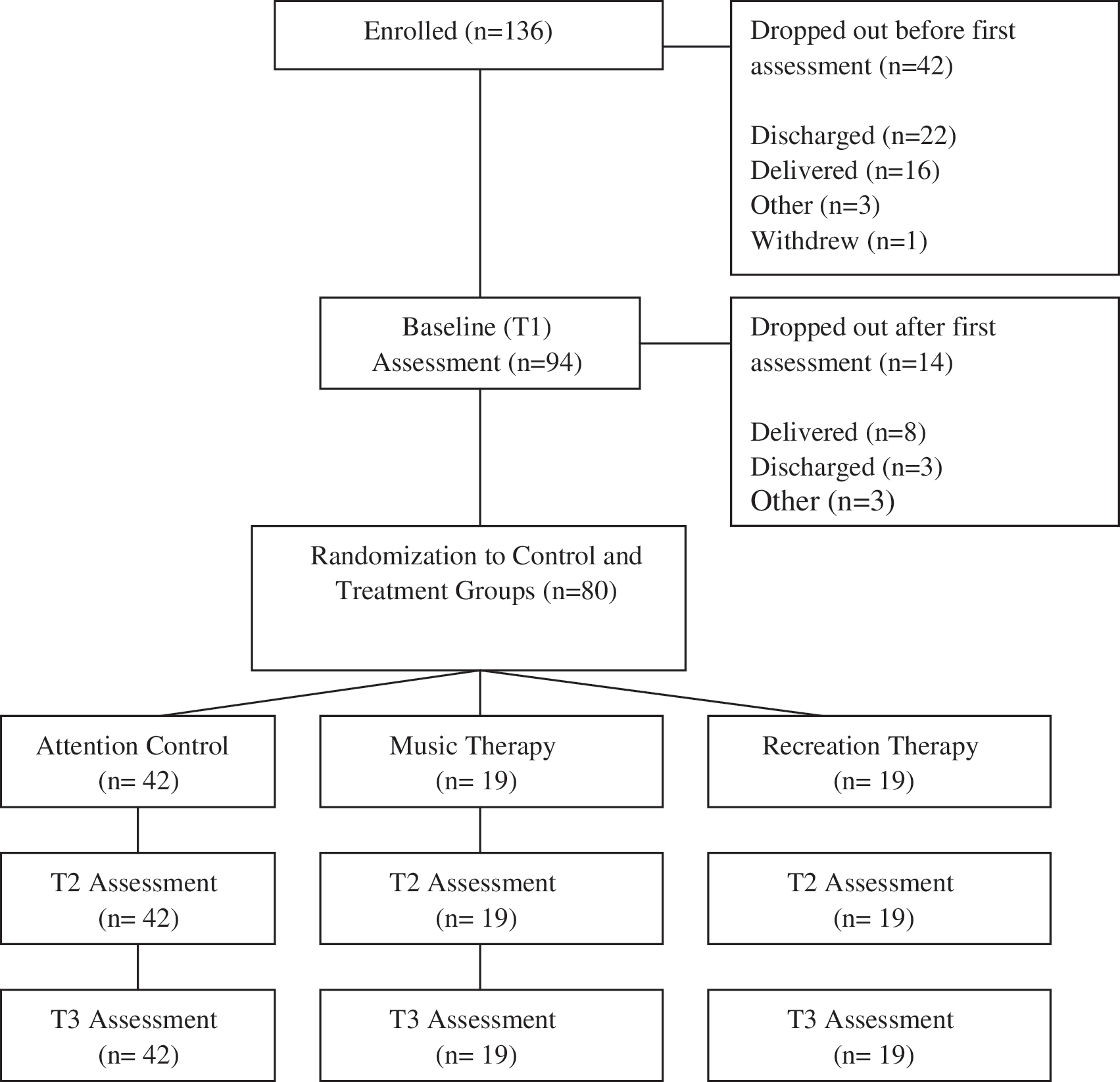
Participant flow.
Study completers were not statistically significantly different from those who dropped out for whom we had baseline data (n = 14) on medical and demographic variables, such as admission diagnosis (chi-square (2, n = 94) = 1.2, p = 0.56), age (t[92] = 0.25, p = 0.81), ethnicity (chi-square (4, n = 95) = 5.9, p = 0.21), or education (chi-square (5, n = 95) = 6.4, p = 0.26). We did detect a statistically significant mean difference (t [92] = −2.5, p = 0.02) on baseline ABEII total scores between completers (M = 36.8, SD 11.4) and those who dropped out (M = 44.9, SD 10.7), suggesting that those who dropped out experienced higher levels of distress than those who remained in the study. This finding may be attributable to the fact that 88% of these patients either delivered or were discharged from the hospital shortly after being enrolled, two events that could certainly contribute to heightened emotionality. Alternatively, this may reflect a general pattern in clinical research whereby more highly distressed people prematurely terminate from studies more frequently than those with comparatively less distress. 41,42 There were no statistically significant differences between experimental and control conditions on sociodemographic and clinical characteristics and baseline ABEII scores, except for type of birth (primiparous vs. multiparous, p = 0.03) (Table 2). Because of this significant group difference, we included type of birth as a covariate in the model. There were no statistically significant group differences between total good events, total bad events, or use of tocolytics; therefore, none of these variables was held constant in the model.
Impact of interventions on antepartum distress
Using paired t tests, statistically significant mean differences were observed immediately after the music and recreation therapy interventions (p = 0.00 and 0.02, respectively) but not in the control condition (p = 0.45). A contrary trend was observed for the music therapy group between the second and third assessments (e.g., immediately after the intervention and 48–72 hours later) whereby distress scores increased by approximately 5 points (p = 0.02) but nevertheless remained lower than baseline scores. Recreation therapy and control group scores remained relatively stable (Fig. 2). When examining changes across the entire study period (e.g., between baseline and 48–72 hours), this negative trend was largely attenuated for the music therapy group score, which decreased by approximately 5 points compared with baseline observations (p = 0.01). Similarly, the recreation therapy group score also decreased by approximately 5 points from baseline (p = 0.04). The control group reported a roughly 2-point decrease during this same period, which again was not statistically significant (p > 0.05). Figure 2 provides a comparison of mean changes for the ABEII scores by groups over time.

Antepartum Bedrest Emotional Impact Inventory (ABEII) mean changes across assessments.
Compared with the control group (d = 0.03), the music therapy group leveraged a large effect on decreasing distress on the ABEII total score between Time 1 and Time 2 (d = 0.87), whereas the recreation therapy group achieved a medium effect (d = 0.49). This was followed by a small increase in distress scores between Time 2 and Time 3 for the music condition (d = −0.38), with relatively stable scores for the recreation (d = 0.02) and control groups (d = 0.16). Finally, small to medium-sized overall decreases in distress were observed for music and recreation between Time 1 and Time 3 (music d = 0.44; recreation d = 0.49). Although the music condition evidenced a larger effect size initially compared with recreation or control conditions, this group demonstrated a small increase in distress between Time 2 and Time 3, whereas the other conditions remained relatively stable. In the end, both music and recreation therapy groups achieved roughly similar mean changes and effect sizes across the entire study period that were superior to the control condition in terms of total distress reduction. After covarying out the effect of type of birth, ABEII distress scores demonstrated the same patterns of significance and magnitude across assessments.
Discussion
This study prospectively examined the efficacy of brief music and recreation therapy interventions to reduce antepartum distress among women with high-risk pregnancies experiencing extended antepartum hospitalization. Results suggest that after controlling for type of birth, participants who were provided a single session of music or recreation therapy experienced significantly less antepartum distress compared with control participants. Interestingly, distress scores from music group participants increased slightly between 1 hour postintervention and 48–72 hours later, whereas recreation and control group scores remained relatively stable. It is important to note, however, that none of these score increases ever surpassed baseline levels. During this period, we speculate that the calming and possibly distracting effects of the music intervention gradually began to lessen, characterized by increases in negative affect. It is also possible that music group participants' ABEII reports were influenced by demand characteristics of the study, a common phenomenon following a pretest–experimental procedure–immediate posttest design. 43 Nevertheless, small to medium statistically significant differences (in favor of the music and recreation groups) were observed in total distress when examining changes across the entire study period.
The strengths of this study include the randomized control design and evaluation over three time points. The follow-up assessments between 48 and 72 hours provide new information about the potential longer-term (beyond immediate) impact of music and recreation therapy interventions on a hospitalized antepartum population. We believe this study is the first to systematically examine the therapeutic effects of music and recreation therapy on a relatively large sample of hospitalized antepartum patients. Although these interventions have been the subject of recent research, previous studies have investigated the effects of these interventions on other populations or have been limited to exploratory studies using very small samples. This study expands on earlier, limited findings that music and recreation therapy can be effective methods for reducing antepartum distress. 6
This study is not without limitations. Although we provided a rationale for why we believed a new antepartum distress measure was necessary for this study (and took appropriate steps to develop it within recommended instrument development guidelines), at this point the ABEII has not been sufficiently validated. In this study, preliminary reliability and concurrent validity associations with clinical variables showed potential for this scale, but additional testing is needed with larger samples and the inclusion of outside measures of the same or similar constructs. Second, selection bias may have occurred, given that the patients who consented to participate in this study were possibly more motivated and resource seeking than patients declining consent. Thus, participants may have been more likely than the general population of hospitalized antepartum women to benefit from music and recreation therapy. We feel confident, however, that selection bias was minimal because of our high response rate. Additionally, participants in the music and recreation therapy groups naturally had increased contact with the therapist. It is possible that the decreased levels of distress resulted, in part, from additional, nonspecific, empathic attention rather than from the actual music or recreation therapy interventions. We attempted to minimize this potential confounding variable by using an attention-control group. Given the 2:1 randomization scheme of the control/treatment conditions, it is possible that this unequal proportion may have influenced group assignment equity to some extent. Finally, because not all participants received exactly the same intervention (roughly 90% from each condition selected the same type of intervention), it is not possible to understand specific mechanisms of action outside of knowing more globally that music and recreation therapy demonstrated preliminary effectiveness at decreasing antepartum-related distress.
Conclusions
This study showed that music and recreation therapies have demonstrated preliminary acceptability and effectiveness in decreasing antepartum-related distress among this population. Given that highly distressed participants may have declined interest or dropped out, these interventions may be most feasible for expectant mothers who are mildly to moderately distressed. Future research in this area may be aided by repeated implementation of these interventions and conducting follow-up studies at longer intervals to investigate the potential intensity and longevity of positive effects. In addition to further refining and validating the ABEII scale, collection of additional physiological measures of distress (e.g., salivary cortisol, blood pressure, heart and respiration rates) would also help elucidate potential mechanisms of action. To further explore the potential confounding effects of personal care and attention, future research may consider comparing a brief face-to-face music therapy intervention with a recorded CD or DVD of the same intervention.
Given the rising number of high-risk pregnant women being placed on hospital bed rest and the association between antepartum distress and adverse pregnancy events, treatment of antepartum distress is important and should not be ignored. These findings suggest that a finite and safe intervention can significantly decrease patients' distress at this critical time. We assert that similar antepartum units would do well to initiate and support music and recreation therapy programs in the context of providing comprehensive medical and psychosocial care to high-risk pregnant women.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.