
Abstract
Rapid eye movement (REM) sleep behavior disorder (RBD) is a treatable parasomnia involving dream-enacting behaviors that is considered to be a male-predominant disorder. However, it is speculated that underrecognition of RBD among female patients in part contributes to the male predominance, probably because women have less aggressive and violent RBD behaviors. We conducted a literature review focused primarily on women with RBD, in which the age of onset of RBD, types of nocturnal behaviors, presence of dream enactment, polysomnographic findings, clinical course, treatment response, male/female ratio, comorbid diagnoses, and medications were tabulated and discussed. RBD was found to primarily affect middle-aged and older women and those with a broad range of neurological disorders. As the link between RBD and neurodegenerative disorders, such as Parkinson's disease, becomes increasingly apparent, including the delayed emergence of parkinsonism in patients initially diagnosed with idiopathic RBD, primary care and specialty physicians should be aware of RBD in women, its potential complications, its excellent response to clonazepam, and its association with neurological disorders and older age groups.
Introduction
Rapid eye movement (REM) sleep behavior disorder (RBD) is a treatable parasomnia often associated with parkinsonism, which is characterized by the release of abnormal behaviors accompanying the loss of the customary generalized muscle paralysis during REM sleep (REM-atonia). 1 RBD clinically manifests as increased muscle tone during REM sleep that is often accompanied by dream-enacting behaviors that can cause injury and sleep disruption, as the dreamer is attending to the dream environment with eyes closed rather than attending to the actual bedroom environment. Both the affected person and the bed partner are at considerable risk for sleep injury and sleep disruption caused by RBD.
RBD can be symptomatic or idiopathic. When there is an associated neurological disorder, such as narcolepsy or a neurodegenerative disorder, the term “secondary” or “symptomatic” RBD is used. “Idiopathic” RBD (iRBD) is used in the absence of an associated neurological or other clinical disorder. A sleep laboratory study, polysomnography (PSG), is required to establish the diagnosis of RBD by detecting REM sleep without atonia (RSWA) (Fig. 1). However, the diagnosis of RBD also requires either a history of disruptive or violent behaviors during sleep or abnormal REM sleep behaviors documented by PSG. Subclinical RBD refers to the presence of RSWA (and some minor behaviors) without any clinical RBD.
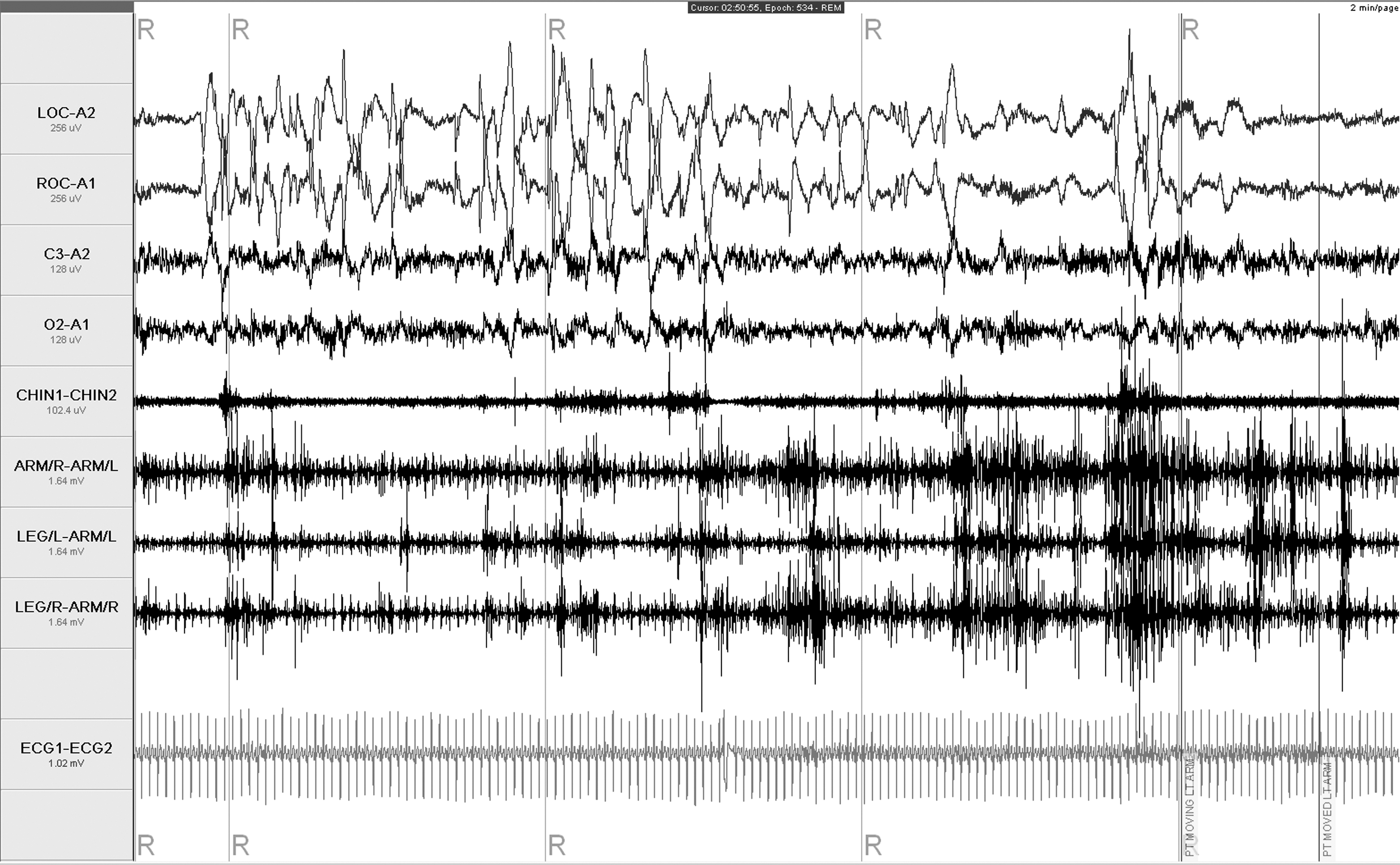
The PSG demonstrates increased muscle tone during REM sleep (RSWA). This female patient broke her cervical vertebra process by flying out of bed and hitting her head on he bathroom door while dreaming she was stepping over a low fence in her neighbor's garden.
Male predominance has been a hallmark of RBD, with the reported percentage of female RBD patients around 13%, 2 –4 Although pooled chronic RBD data by Schenck et al. 3 demonstrated 36.5% were women. Of 100 consecutive patients with injurious nocturnal behaviors, only 1 of 29 women had RBD vs. 35 of 71 male patients. 5 Could the male predominance be in part explained by the more aggressive and violent behaviors among male patients vs. female patients, leading male patients to preferentially seek medical attention? The first reported case series of RBD in 1986 described 4 men and 1 woman. 1 In the cases involving men, they or their spouses reported aggressive sleep behaviors, whereas the 1 woman reported sleep disruption. In patients with both Parkinson's disease (PD) and RBD, sleep-related injuries are associated more often with male patients. 6 Overall, there is little reported about the spectrum of RBD in women. We attempt to clarify this issue by reviewing the literature on RBD in women.
Materials and Methods
We reviewed PubMed for articles written in English and Spanish published between 1986 and 2009 with the key words “REM Sleep Behavior Disorder” and “females, women or woman,” as well as relevant articles found through references and abstracts from scientific meetings. Full articles were reviewed for relevance if the titles or abstracts described patients with symptoms suggestive of RBD. Articles were excluded if there was no mention of sex or clear breakdown by sex before or after any intervention. The remaining articles were further reviewed for age of onset, age of diagnosis, secondary diagnosis, medications, types of nocturnal behaviors, presence of dream enactment, PSG findings, treatment, clinical course, and male/female ratio.
Results
We included 126 articles in our review. Most articles either involved small case series or provided very little information about the female patients. Of the articles that contained the pertinent information, the mean age of onset of RBD in women was 48 ± 23 years (n = 113) and ranged from birth to 86 years. The mean age at diagnosis was 54 ± 20 years (n = 77). The etiologies of RBD in women are listed in Table 1. The onset of symptomatic RBD by decade of life had the following etiological associations: first decade: narcolepsy, midline cerebellar astrocytoma, Mobius syndrome, autism; second decade: narcolepsy in the PD; third decade: narcolepsy, multiple sclerosis (MS), spinocerebellar ataxia (SCA); fourth decade:narcolepsy, MS, SCA; fifth decade: narcolepsy, dementia with Lewy bodies (DLB), chronic autoimmune meningoencephalitis, PD, multiple system atrophy (MSA); sixth decade: narcolepsy, MSA, DLB, PD, MS; seventh decade: DLB, SCA, MSA, progressive supranuclear palsy (PSP), pure autonomic failure, acute inflammatory demyelinating polyneuropathy (AIDP), stroke, corticobasal degeneration (CBD); eighth and ninth decades: PD, DLB, MSA, CBD, stroke.
Clinical manifestations of RBD in women, as described in the literature, included nocturnal awakenings, yelling, talking, crying, groaning, laughing, head movement, pelvis movements, kicking, slapping, hitting, thrashing, waving arms, grimacing, jerking, gesturing, limb movements, arm movements, running movements of legs, sitting up, standing up on the bed, getting out of bed, jumping out of bed, falling out of bed, bruising, injury to self, injury to bed partner, attacking bed partner, and strangling the bed partner. Of 60 women with RBD where details on their behavior were provided, 36 (60%) were noted to have violent behaviors. The authors did not routinely comment on the presence of dream-enacting behaviors. In cases that did report on such behavior, however, 29 cases (87.8%) reported dream-enacting behavior, whereas only 4 cases (12.5%) specifically reported no dream-enacting behaviors. 28,37,79,80,85,87,96 REM without normal atonia was seen in all cases where PSG results were provided and ranged from increase in electromyographic (EMG) activity to complex behaviors in REM sleep.
Treatment used and responses to therapy were not frequently provided. Positive response was most notable with clonazepam, although case reports of improvement in women were noted with donepezil, carbidopa/levodopa, pramipexole, temazepam, fluvoxamine, paroxetine, yi-gan san, and adrenocorticortropic hormone (ACTH). 7,30,42,53,73,97 Therapy used included clonazepam, 8,9,14,15,37,40,42,55,80,81,87,88,92,94,98 –101 donepezil, 42 amitriptyline, 1 carbidopa/levodopa, 53 imipramine hydrochloride, 91 pemoline, 91 pramipexole, 7,69,102 melatonin, 92,98,103,104 carbamazepine, 98 sertraline, 98 IVIG, 40 and ACTH (MS). 86
When data on all cases that specified sex were pooled, the percentage of female RBD patients was 27% 2 –4,6 –71,73 –83,86 –94,96 –100,102 –133 ; MS patient with RBD had the highest percentage of female patients (Table 2). A large number of these studies were done at sleep centers, which adds significant referral biases. Although attempts were made to avoid duplication, it is very likely the same RBD patient may be represented more than once, given multiple articles from the same centers. When including only articles that looked at screened consecutive patients with PD for RBD based on a history or questionnaire, the percentage of women found to have RBD was 25%. 6,48,51,57,59,66 –68,131 However, when consecutive patients with PD were evaluated with PSGs, this percentage increased to 37.5% (Table 3). 54,58,64,70,131
REM sleep without atonia.
Similar findings were noted in other diseases that looked at consecutive patients. All 4 patients (1 woman) who had extrapyramidal symptoms with pure autonomic failure had RBD. 73 All men and women with MSA who underwent a PSG were found to have REM without atonia and gross movements during REM sleep. 74 Another study found 35 of 39 patients (13 women) with MSA had PSG findings of RBD. 72 Although they noted there was no statistically significant relationship between patient sex and RBD, they did not provide the details on the sex of the 35 patient with RBD. The ratio of women with narcolepsy and RBD was similar to that of men, 22 of 53 and 25 of 46, respectively. 32,33 However, only 25% of women with clinical RBD demonstrated RBD behaviors during video-PSG compared with 53% of men. 32 In a study of children with autism and sleep complaints, RBD was found in 2 of 2 girls and 3 of 9 boys. 94 Of patients with posterior cortical atrophy (PCA) and visual hallucinations, 5 of 7 females and 3 of 6 males had RBD. 43 When looking at RSWA, similar ratios between female and male patients were noted in Alzheimer's disease (AD), PD, PSP, and narcolepsy. 32,58,78
Tatman and Sind 105 specifically targeted differences between men and women. They reviewed 400 patients studied in the sleep center and found 8 patients with RBD, comprising 4 men, 3 women, and 1 transsexual (male by birth). In their abstract, they found that women had considerably higher arm EMG densities, whereas men had higher leg densities. In fact, 2 women had a previous PSG without arm EMG electrodes, and consequently, RBD was not diagnosed. Women also had more victim dreams, and their spouses reported no violent behaviors in their sleep. On the other hand, Wing et al. 4 also looked at gender differences among Chinese diagnosed with RBD at a sleep center and found no difference among behavioral symptoms or violence but did find that 82% were male and that females were minimally older.
Discussion
Clinicians treating females with neurological disorders at any age, including childhood, as well as clinicians treating older female patients should be aware that RBD can emerge in older age groups and in patients with a wide variety of neurological disorders, similar to what has been reported in men. Although a wide range of nocturnal behaviors has been described in women with RBD, there still is a deficiency in the literature of descriptions of these behaviors that to date has hindered a clear understanding of the differential expression of RBD across genders. Similar to men, women have had a robust positive response to clonazepam, which is the standard therapy of RBD. 8,9,14,15,42,55,87,88,98 Medications, especially antidepressants, can also exacerbate or cause RBD. It is unclear if antidepressants unmask underlying (i.e., subclinical) RBD or cause RBD. More research needs to be focused in this area.
It has been reported that RBD is considerably more common in men, 2 –4 Although in narcolepsy patients, the frequency of RBD is similar between men and women. 33 When consecutive patients with PD are all screened for RBD with PSG, the frequency of RBD among women is closer to that of men, that is, 38% vs. 57%. Compared with the clinical history, the frequency of RBD in women was only 25%. It appears that clinical history or questionnaires alone are not as sensitive in diagnosing RBD in women, which could lead to their being underdiagnosed with RBD. Although the sample sizes were small, in studies that screened for RBD in patients with a specific neurological disorder, the ratio of women with RBD was closer to that of men with RBD, specifically when using PSG together with a questionnaire. 6,8,32,33,43,51,54,57,72 –74,80,88,94,131 When including patients with RSWA, the ratio of women with RSWA and men with RSWA was even closer 58,78 ; the closer ratio among men and women with RSWA vs. RBD may suggest a different expression of the disease process. This would be supported by less aggressive and violent behaviors among women and higher arm EMG activity vs. leg activity during PSG. 67,105 However, more descriptive information is needed on the range of behaviors of RBD in women. Sex hormone alterations have been hypothesized to play a role in the predominance of male patients with RBD, but recent studies have failed to show any clear relationship. 134,135 Because the male/female ratio of PD is around 1.5 in western populations, estrogen has been hypothesized to be neuroprotective. However, there is no gender difference in Asian PD populations, which would be unusual if the male predominance of PD was related to estrogen. 136
The clinical significance of RSWA in the absence of clinical symptoms of RBD or of mild RBD in women who are not injuring themselves or bed partners remains uncertain. There is a strong association with RBD and neurodegenerative disorders, however, specifically synucleinopathies. 50,137 –141 Between 15% and 26% of patient with PD also have RBD (36% before and 63% after diagnosis of PD). 57,142 Idiopathic RBD (iRBD) may be one of the earliest signs, evident more than 20 years before a clinical diagnosis of parkinsonism can be made. 138 The 12-year risk of patients with iRBD developing a neurodegenerative disease has recently been estimated to be 52%. 50 Reduced cardiac 123 I-MIBG accumulation has been demonstrated in iRBD, PD, and DLB compared with normal controls, supporting a relationship between iRBD and α-synuclein neurodegenerative disorders. 137 SPECT brain imaging has also demonstrated similarities among patients not only with PD and iRBD but also with RSWA. 130 Although the clinical course of RSWA is unknown, there is growing evidence that RSWA may have the same clinical course as iRBD. 143 Therefore, the need for more systematic, descriptive RBD behaviors in women is of particular clinical importance, as a preponderance of men, aged ≥50 years, with idiopathic RBD will eventually develop a parkinsonian disorder. So the possibility remains that a comparable percentage of women with less vigorous behaviors in REM sleep (undetected RBD) will also develop a parkinsonian disorder.
Neuroprotective agents have historically been shown to be helpful in in vitro and animal studies but lack effectiveness in human clinical trials. 109,144,145 One possibility for the lack of effectiveness is the timing of initiation along the course of the disease. As neuroprotective agents become more efficacious, they will need to be administered at the first sign of the disease (e.g., idiopathic RBD or possibly RSWA). It would then be especially crucial to not underdiagnose RBD in women, especially taking into account that women on average have been diagnosed with RBD 10 years after the age of onset of symptoms. 80,81,94,99 –101
Physicians need to be aware of the victim vulnerability factors. Bed partners of patients with RBD are at increased risk for morbidity or mortality related to injuries occurring from an RBD episode. Women and children have been the victims of violent behaviors from their bed partner who suffers from RBD, such as choking, headlocks, and punching. 95 Educational resources are available that document the first-hand accounts of women who were accidentally victimized—physically, emotionally, and with repeated sleep disruption—by sleeping with husbands with aggressive and violent RBD. The beneficial response to therapy of RBD with clonazepam on the sleep and overall well-being for both bed partners is also discussed. 146,147 To date, not one case of marital separation or divorce as a result of RBD has been reported, which probably attests to stable marriages lasting decades before the onset of RBD and recognition by the spouse that the partner afflicted with RBD was acting completely out of character during sleep.
Conclusions
RBD does occur in women and is probably underrecognized. The findings presented from the literature search indicate the importance for primary care and specialty physicians to be aware of RBD, its potential for injury and sleep disruption, its excellent response to clonazepam, its association with neurological disorders and older age groups, and its particular risk as a herald for future parkinsonism. It is important for healthcare providers to recognize the symptoms of RBD in women, especially if there is an underlying neurological disorder. Primary care and specialty care providers for women with neurological disorders and of middle-aged and elderly women should routinely ask their patients and spouses about the presence of any sleep-related behaviors, particularly those associated with dream enactment and consider referral to an accredited sleep disorder center for evaluation of RBD. Screening questions for RBD are provided in Table 4. With the development of neuroprotective agents, it will become more urgent to not delay the diagnosis of RBD in women, given the possibility of an increased risk for future parkinsonism/dementia.
Disclosure Statement
There was no financial support or investigational use of medications associated with the contents of this article. Clonazepam therapy of RBD is an off-label use of this anticonvulsant medication.
The authors have no conflicts of interest to report.