
Abstract
Aims:
This study aimed to assess the rates of detection, treatment, and referral of maternal depression and anxiety by obstetrical providers during pregnancy and at 6 weeks postpartum.
Methods:
A convenience sample of women receiving obstetrical care at a large urban teaching hospital (n = 491) was screened for depression and anxiety during the third trimester of pregnancy and again at 6 weeks postpartum using the Edinburgh Postnatal Depression Scale and the anxiety portions of the Patient Health Questionnaire. Participants were also asked if they thought they needed help for depression, anxiety, or stress at the two time points. Obstetrical providers were blind to screening results. Two months postdelivery, each woman's obstetrical electronic medical record (EMR) was reviewed for documentation of psychiatric symptoms, diagnoses, psychiatric treatment, and mental health referrals at the two time points. Data were analyzed using descriptive statistics.
Results:
Twenty-three percent of participants screened positive for an anxiety disorder or high levels of depressive symptoms or both prenatally, and 17% screened positive at 6 weeks postpartum. The majority of women who screened positive were not identified by their providers during pregnancy or postpartum. Only 15% of positively screened participants had evidence of any mental health treatment in their EMR during pregnancy, with equally low rates of referral to mental health or social services. In the postpartum period, only 25% of positively screened postpartum women received treatment, and an additional 2.5% were referred. A low proportion of women who reported they felt a need for help with depression, anxiety, or stress prenatally or postpartum received treatment or referral.
Conclusions:
These findings indicate that detection, treatment, and referral of perinatal depression by obstetrical providers are seriously lacking and need to be addressed.
Introduction
For many women, the perinatal period represents a time of increased vulnerability to psychiatric illness. A substantial number of women experience their first onset of mood or anxiety disorders during pregnancy or within the first few months after giving birth, and those with a history of psychiatric disorder are at increased risk for a recurrence or relapse of symptoms. 1,2 Perinatal psychiatric distress negatively affects women's personal well-being and quality of life and, if left undetected and untreated, may negatively affect fetal and infant development. 3 –7 Nevertheless, detection and treatment rates for perinatal depression and anxiety are alarmingly low. 8 –12
Perinatal depression
Perinatal depression is considered the most common complication of childbirth. 13 Antenatal depression has a reported prevalence of 7%–20% 1,14 –18 and, if left untreated, can lead to a chronic or recurring depressive course throughout the woman's life. 1,19 Untreated antenatal depression has been associated with prolonged use of sick leave, 21,22 maternal functional impairment, 22 inadequate prenatal care, 23 and substance abuse, 24 all of which can affect birth outcomes. Several obstetrical complications and adverse birth outcomes have been associated with untreated prenatal depression, including preeclampsia, neonatal growth retardation, preterm deliveries, low birth weight in babies, spontaneous early labor, admission to neonatal intensive care units, spontaneous abortion, and fetal death. 3,5 Prenatal depression has been linked to less favorable child outcomes. 6 Moreover, depression during pregnancy is the greatest risk factor for postpartum depression. 25,26
Postpartum depression affects approximately 13% of new mothers, 27 with rates as high as 38.2% among lower socioeconomic status (SES) first-time mothers. 28 Postpartum depressed mothers are less likely than nondepressed mothers to achieve prepregnancy functional status in such areas as personal care, social interaction, household care, and occupational activities. 29 The negative impact of postpartum depression on the early mother-infant relationship and on the child's social, emotional, and behavioral development is well-documented and includes attachment insecurity, behavioral and social difficulties, impaired emotional development, impaired cognitive development, and long-term behavioral problems. 4,30 –36
Perinatal anxiety
The presence of anxiety disorders during the perinatal period has been much less studied 37 ; however, recent findings indicate that symptoms of anxiety are common during pregnancy and the postpartum period 38 –40 and that depression and anxiety are frequent comorbidities. 41 Maternal symptoms of anxiety during pregnancy have been associated with adverse fetal and developmental consequences in some 37,42 –44 but not all studies. 45,46 A strong link between anxiety during pregnancy and later postpartum anxiety and depression has been demonstrated. 47 –49
Identification and treatment of perinatal depression and anxiety
In the United States, many women consider their obstetrical/gynecological care provider to be their primary care provider during their childbearing years. 50 Obstetrical/gynecological care providers are often the first, most consistent, and sometimes the only healthcare provider for women, 51 especially during their reproductive years, and pregnant and postpartum women generally have frequent contact with them by way of prenatal visits, hospital delivery, and postpartum follow-up. Primary care providers, including obstetrical providers, have an increasing role in early detection and treatment of psychiatric disorders. 52 However, the overlap between common somatic complaints of pregnancy, such as fatigue or appetite changes, with symptoms of depression or anxiety can make identification of perinatal anxiety or depressive disorders more difficult. 53,54 Routine screening for psychiatric disorders during pregnancy is reported to be uncommon. 55,56
Because of the clear evidence of the negative effects of untreated perinatal depression and anxiety on women and infants, it is important that at-risk women are not only identified but also treated. Fortunately, effective pharmacological and nonpharmacological treatments exist for perinatal depression and anxiety, 57 –62 although there are treatment dilemmas, especially in regard to pharmacological treatment during pregnancy or lactation. 63 Research has shown that women who discontinue antidepressant medication during pregnancy have a much greater likelihood of relapse than those who continue medication, 2,64 emphasizing the importance of close monitoring of such women.
A small number of studies have documented that a substantial proportion of women treated in obstetrics have unrecognized and untreated psychiatric disorders. 9 –12 Marcus et al. 10 used the CES-D 65 to screen for depression in 3472 pregnant women in obstetrical clinics and found 20% of the women screened positive for depression, yet only 14% of the depressed women self-reported receiving any treatment for depression. Spitzer et al. 11 screened 3000 obstetrical/gynecological patients using the PRIME-MD 66 and then used provider reports to determine who was identified by providers as having a psychiatric disorder. They found that only 35% of the women who screened as having a psychiatric disorder were identified by providers. Two other studies used medical record review to assess provider recognition of psychiatric problems and subsequent treatment. Kelly et al. 9 used the PRIME-MD with 186 ethnically diverse, pregnant women. Forty-three percent of women who screened as positive for a psychiatric disorder or substance abuse in their sample had documentation of psychiatric symptoms in their medical record, 18% had a documented psychiatric diagnosis, and 23% had documentation of psychiatric treatment. Another study found even lower rates of identification and treatment. Smith et al. 12 used the Patient Health Questionnaire (PHQ) 67 to screen for depression, panic disorder, and posttraumatic stress disorder (PTSD) in 387 pregnant women in public sector obstetrical clinics. Only 2% of the women who screened positive for depression were identified or referred to treatment, only 1 woman (11%) who was positive for panic disorder was identified and referred, and none of the women (n = 10) who were positive for PTSD were identified.
These previous studies have focused on pregnant women or a mix of obstetrical/gynecological clinic patients, but no study could be found that assessed obstetrical provider detection and treatment of postpartum depression or anxiety. Two studies used medical records to assess provider detection and treatment but with very different results, and no study compared screening with the Edinburgh Postnatal Depression Scale (EPDS),
68
the most commonly used perinatal depression screening tool, with provider spontaneous detection of depression. The current study was designed to address these gaps in knowledge. The purpose of this study was to examine the processes of care for women who screened positive for anxiety or depressive symptoms during pregnancy or postpartum. The specific aims were: To assess the rates of detection, treatment, and referral of maternal depression or anxiety or both by obstetrical providers during pregnancy and at 6 weeks postpartum. To determine the frequencies with which women self-reported that they thought they needed help with depression, anxiety, or stress at the two time points and the treatment or referrals received.
Materials and Methods
Design and setting
This article presents findings related to the identification, treatment, and referral of women with perinatal depression or anxiety by obstetrical providers derived from a larger longitudinal, descriptive study using both quantitative and qualitative methods to examine depression and anxiety across the perinatal period. Recruitment sites were two hospital-affiliated obstetrical clinics that serve an ethnically and socioeconomically diverse population of pregnant women and postpartum women. Care at the sites is provided by one faculty practice consisting of obstetricians, midwives, nurses, and social workers. All documentation of provider care occurred within the electronic medical record (EMR) that is used throughout the perinatal process. All participants delivered their infants at the same level III teaching hospital in Boston, Massachusetts. Medical record review took place using the EMR.
Sample
A convenience sample of women who met the following criteria was recruited for the study: (1) in the third trimester of pregnancy (>28 weeks gestation), (2) able to read or speak English or Spanish, and (3) ≥18 years of age. Third-trimester assessment was chosen, as previous research has shown pregnancy depression rates to be highest later in pregnancy. 1 It also allowed for assessment of participants' retrospective felt need for help during all three trimesters. Pregnant minors were excluded because of difficulty obtaining required parental consent in a timely and cost-effective manner. To limit potentially confounding factors, women were to be excluded from the study if they had a previous or current major psychiatric diagnosis of schizophrenia or other psychotic disorder, as patients with these disorders would likely already be identified and in treatment prior to pregnancy. None of the women screened for this study, however, met these exclusion criteria.
Study enrollment was conducted from June 2006 through February 2007. A total of 659 women were given information about the study and invited to participate; 525 agreed to participate and were enrolled into the study (80%). Sixteen women did not complete the prenatal questionnaire and were dropped from the study. Another 18 women either moved or did not deliver at the study hospital, or their medical records were not available and, thus, were not included in the final study sample. The resulting prenatal sample included 491 women. Sixty-one percent of the participants (n = 299) completed the 6-week postpartum questionnaire. Chi-square tests of independence and t tests were performed to determine any group differences between participants who completed the 6-week postpartum questionnaires and those who did not. The percentage of participants who completed the 6-week postpartum questionnaire did not differ by parity, chi-square (1, n = 491) = 3.17, p = 0.075, or by proportion of positive screens for depression and anxiety, chi-square (1, n = 490) = 3.06, p > 0.080. They did differ, however, by race, education, and income.
A greater proportion of white participants completed the 6-weeks postpartum questionnaire compared with Latinas and others, chi-square (2, n = 489) = 19.51, p < 0.001. A greater proportion of women who had more than a high school education completed the postpartum questionnaire compared with participants with a high school education or less, chi-square (1, n = 485) = 10.50, p < 0.001, and a greater proportion of women with household incomes of ≥$60,000 completed the postpartum questionnaire compared with women with household incomes of <$60,000, chi-square (1, n = 467) = 35.59, p < 0.001. Participants who completed the 6-week postpartum questionnaire were older (mean = 32.5 years, SD = 5.2) than those who did not complete the postpartum questionnaire (mean = 30 years, SD = 5.3), t(489) = 4.96, p = 0.001). The demographic characteristics of the prenatal and postpartum samples are shown in Table 1.
Mean age for prenatal sample 31.6, range 18–45, SD = 5.35.
Mean age for 6-weeks postpartum sample 32.5, range 18–45, SD = 5.18.
Procedures
All study procedures were approved by the Institutional Review Board of a large academic medical center in Boston where the participants were recruited before initiation of the study. Patients attending prenatal clinics on days when research staff were present were invited to participate in the study. Study staff included graduate nursing students and bilingual Spanish-speaking research assistants (RAs) for the recruitment site with a predominantly Spanish-speaking population. Obstetrical care providers were told that a study of moods during pregnancy was being conducted at their clinic but were blind to screening results.
An RA trained in the administration of the study consent form and questionnaires approached eligible women in the clinic waiting room prior to the women's prenatal appointment. The RA described the study, answered questions, and obtained written informed consent from each woman before administering the prenatal questionnaire. Participants completed the questionnaire in the clinic waiting room or in an empty clinic examination room either before or after a prenatal visit. The questionnaire was self-administered, but the option to have the RA assist with completing the questionnaire was offered in an effort to include women for whom language or literacy level may benefit from such assistance. Some participants opted to take the questionnaire home to complete and return it in a stamped envelope provided. All participants received a $5 gift card after completion of the prenatal questionnaire.
A postpartum questionnaire was mailed to all participants at 6 weeks postpartum, along with a stamped addressed envelope for return of the questionnaire. Reminder phone calls were made to women if a questionnaire was not returned within 2 weeks of mailing.
Two months after delivery, each participant's obstetrical EMR for the period of the index pregnancy through 6 weeks postdelivery was systematically reviewed using an investigator-developed Medical Records Data Collection Tool. Three graduate nursing students assisted in the record review. After receiving training in the record review procedures, reviewers were evaluated and achieved at least 95% interrater reliability for ability to agree on collected data before proceeding to review charts independently. In addition, 5% of charts were randomly selected after completion of the first 100 reviews and checked for accuracy of data collected, and, again, at least 95% reliability was attained. All prenatal, delivery, and postpartum notes, problem lists, summaries, and referral notes for the index pregnancy were reviewed, including notes by obstetricians, nurse midwives, nurses, social workers, and others involved in care. Records were reviewed for documentation of psychiatric symptoms, psychiatric diagnoses, psychiatric treatments, and referrals to psychiatric or social services.
Instruments
A prenatal questionnaire developed by the researcher and administered during the third trimester of pregnancy was used to collect data about demographics (age, marital status, employment status, educational attainment, race/ethnicity, immigrant status), past and current mental health symptoms, past or current psychotropic use, and other potential risk factors for depression and anxiety. The study questionnaire also contained the EPDS 68 and the anxiety sections of the PHQ. 67
The EPDS 68 was used to assess level of depressive symptoms. The EPDS is a 10-item self-rating scale developed to detect depression in postpartum women in community samples. The EPDS has been well validated for use in prenatal and postpartum populations 1 and has a validated Spanish version, 69 which was used for Spanish-speaking participants in this study. The scale focuses on cognitive and affective features of depression rather than somatic symptoms, which may confound detection during pregnancy or the postpartum period. The scale has had satisfactory reliability and has adequate sensitivity and specificity when compared with a psychiatric diagnosis of major depression. As recommended by the authors, a cutoff score of 9/10 for minor depression and a cutoff score of 12/13 for major depression were used, and women scoring ≥10 were considered depressed in this study.
The anxiety portions of the PHQ 67 were used to screen participants for anxiety disorders. The PHQ is a self-administered version of the PRIME-MD 66 and has been validated for use in primary care settings 67 and with obstetrical/gynecological patients. 11 Positive findings on the PHQ correspond to specific diagnoses in the Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV). 70 Only the questions pertaining to anxiety (“panic syndrome” and “other anxiety syndrome”) were used in this study. A validated Spanish version was used for Spanish-speaking participants. 71
A postpartum questionnaire was administered via mail at 6 weeks postpartum to collect data about postpartum stressors, use of psychotropic medication, or other mental health treatments since the birth of the baby. The questionnaire included the EPDS and the anxiety sections of the PHQ.
A Medical Records Data Collection Tool developed by the researcher was used to facilitate extraction of data from participants' medical records at 6 weeks postpartum. Data extracted included any documentation of the following for the index pregnancy and postpartum period: (1) psychiatric symptoms (e.g., tearful, sad, poor sleep), (2) psychiatric diagnoses (e.g., depression, anxiety), (3) psychiatric treatments (medication or psychotherapy or both), and (4) referrals to psychiatric or social services and noted outcome of the referral (accessed, declined, or not known). In addition, documentation of past psychiatric diagnoses and treatments, obstetrical history (number of pregnancies, number of spontaneous and elective abortions, maternal or fetal health problems), and pregnancy outcome variables (Apgar scores, gestational age at delivery, type of delivery, birth weight, perinatal complications, and level of neonatal care) for the index pregnancy were abstracted. These findings will be presented elsewhere.
Data analysis
All data were entered into the computer program SPSS version 15 (SPSS, Inc., Chicago, IL), which was used for data management and statistical analyses, and data were checked for accuracy. We determined the prevalence of positive depression and anxiety screens at each time point, followed by the frequencies of documented psychiatric symptoms or diagnoses, mental health treatments, and referrals. McNemar tests were used to determine if there was a significant difference between the proportions of women scoring as positive on the various measures prenatally and postpartum among the participants who completed questionnaires at both times. Means and SDs were calculated for prenatal and postpartum EPDS scores. The frequencies with which women self-reported that they thought they needed help with depression, anxiety, or stress at the two time points were calculated.
Results
Prenatal results
A total of 113 women (23%) screened positive for an anxiety disorder or for depressive symptoms during the third trimester of pregnancy. Table 2 presents the prevalences of depression (both major and minor) and anxiety disorders at the two times. At the prenatal assessment, 109 participants (22%) screened in the depression range on the EPDS, 13.4% in the minor depression range (EPDS 10/12) and 8.6% in the major depression range (EPDS 13+). The mean prenatal EPDS score was 6.28 (SD 4.77). Of the 109 women who were positive for depression (10+ on EPDS) prenatally, 12 (11%) were also positive for panic disorder, and 8 (7.3%) were positive for other anxiety disorder. In all, 17 women (15.6%) had an anxiety disorder comorbid with their depression. In addition, 2 women were positive for panic disorder without depression, and 2 other women were positive for other anxiety disorder without depression at the prenatal assessment (1% of total prenatal sample).
EPDS, Edinburgh Postpartum Depression Scale.
Of the women who screened positive for anxiety or depressive symptoms prenatally, only 46 (41%) had any documentation of psychiatric symptoms or diagnoses by providers in the medical record. Only 17 (37%) of those had documented mental health treatment (psychotropic medication or therapy or both) during pregnancy, and an additional 20 (43%) had a documented mental health or social services referral. Of these, half accessed the referral, and half declined the referral. Nine women (20%) who had documented psychiatric symptoms or diagnoses in the medical record had no documentation of treatment or referral. Of all the women who were identified as depressed or anxious during screening, only 17 (15%) had documented mental health treatment (medication or therapy or both) during pregnancy, and an additional 20 (18%) had a documented mental health or social services referral. Thus, only 37 (33%) of the women who screened as depressed or anxious during pregnancy received any treatment or referral, and two thirds (67%) of the women who screened positive received no psychiatric treatment or referral. In addition, another 9% were referred for help but declined the referral. In all, 76% of the women who scored in the depressed range on the EPDS or screened positive for an anxiety disorder during the third trimester of pregnancy received no mental health services. Figure 1 shows the findings for documented symptoms or diagnoses, treatment, and referral for depression or anxiety during pregnancy.
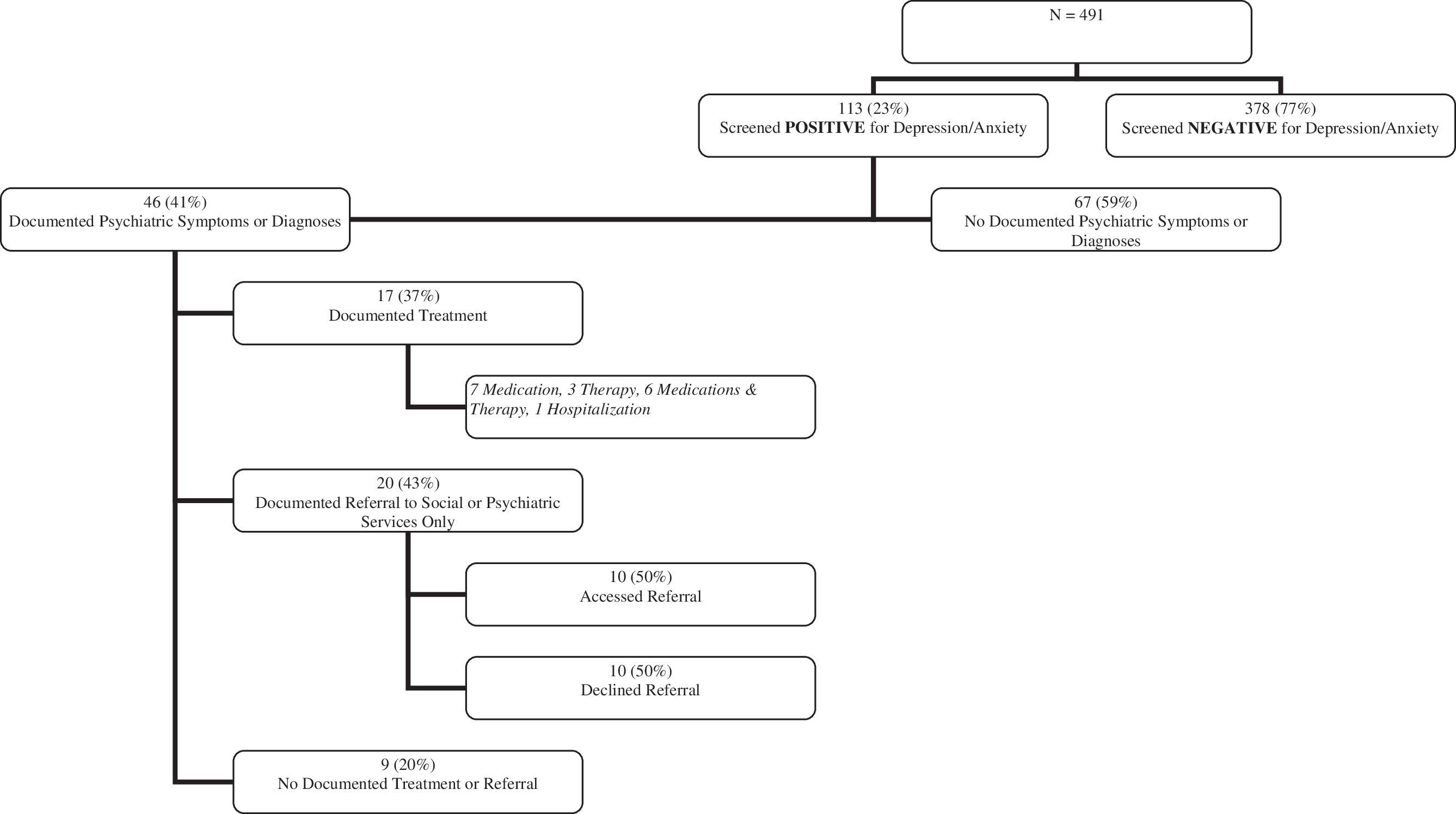
Documented detection, treatment, and referral of depression/anxiety during pregnancy by providers.
Postpartum results
At 6 weeks postpartum, 61% of participants (n = 299) completed the postpartum questionnaire. Of these, 51 women (17%) screened positive for anxiety or depressive symptoms (Table 2). Forty-eight participants (16.1%) screened in the depressed range on the EPDS at 6 weeks postpartum, 26 (9%) in the minor depression range (EPDS 10/12) and 21 (7%) in the major depression range (EPDS 13+). The mean postpartum EPDS score was 5.5 (SD 4.23). Of the 48 women who were positive for depression (10+) at 6 weeks postpartum, 2 (4.2%) were also positive for panic disorder, and 5 (10.4%) were positive for other anxiety disorder. In all, 7 women (14.6%) who scored >10 on the postpartum EPDS had a comorbid anxiety disorder. In addition, 2 women of the postpartum sample were positive for panic disorder without depression, and 2 other women were positive for other anxiety disorder without depression at the postpartum assessment, with 3 women (1%) screening as positive for an anxiety disorder without depression at 6 weeks postpartum.
Of the 51 women who screened positive for anxiety or depressive symptoms at 6 weeks postpartum, only 15 (29.4%) had any documentation of psychiatric symptoms or diagnoses by providers in the medical record. Thirteen (87%) of those had documented postpartum mental health treatment (psychotropic medication or therapy), and 1 additional woman (6.7%) had a documented mental health or social services referral, although there was no record of whether this woman accessed or declined the referral. Only 1 woman (6.7%) who had documented postpartum psychiatric symptoms or diagnoses in the medical record had no documentation of treatment or referral. Of the women who screened positive for depression or anxiety at 6 weeks postpartum, only 13 (25.5%) had documented postpartum mental health treatment (medication or therapy or both), and an additional 1 woman (2%) had a documented mental health or social services referral. Thus, only 14 (27.5%) of the women the study screening identified as depressed or anxious at 6 weeks postpartum received any treatment or referral, and 37 (72.5%) of the women identified by researchers as depressed or anxious during the postpartum period received no psychiatric treatment or referral. Figure 2 shows the findings for documented symptoms or diagnoses, treatment, and referral for postpartum depression or anxiety.
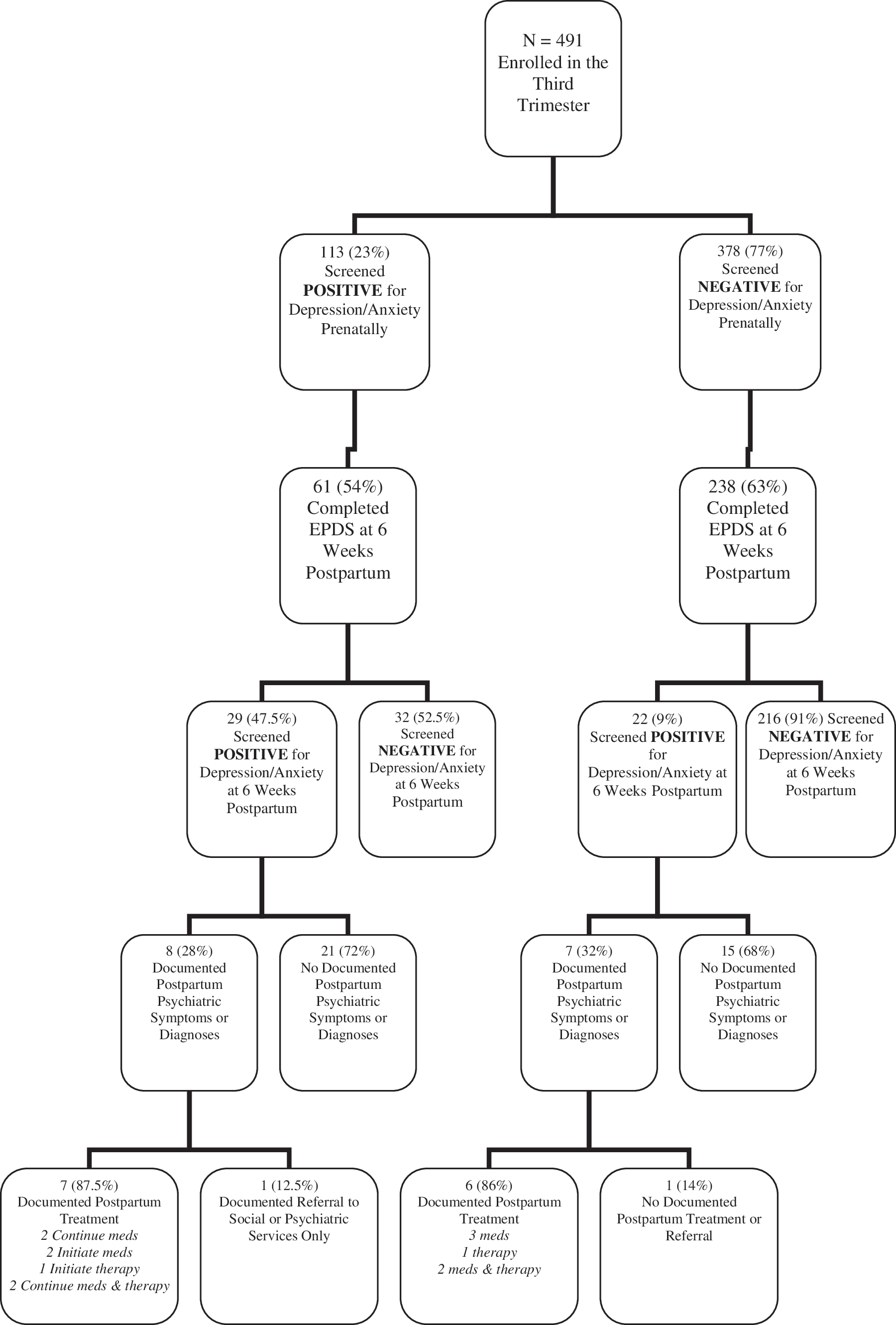
Documented detection, treatment, and referral of depression/anxiety during the postpartum period. EPDS, Edinburgh Postpartum Depression Scale.
Comparison of prenatal and postpartum sample and results
Among the women who completed questionnaires at both time points (n = 299), 19.4% had significant symptoms of depression (EPDS > 9) prenatally, and 16% had significant symptoms postpartum. However, these percentages were not significantly different from each other based on the results of the McNemar test of dependent samples (p = 0.203). Similarly, there were no significant difference between the proportion of women who scored in the probable clinical depression range (13+) on the EPDS prenatally and postpartum (p = 0.690), between the proportion of women who screened positive for panic syndrome prenatally and postpartum (p = 0.227), or between the proportion of women with other anxiety syndrome prenatally and postpartum (p = 0.774). Mean total EPDS scores were significantly higher prenatally (mean 6.04, SD 4.66) than at 6 weeks postpartum (mean 5.5, SD 4.23), t(299) = 2.35, p = 0.019).
Participants felt need for help
On the prenatal questionnaire, 121 women (25%) responded Yes to the question: Have you thought you've needed help with depression, anxiety, or stress during this pregnancy? On the postpartum questionnaire, 42 women (14%) responded Yes to the question: Have you thought you've needed help with depression, anxiety, or stress since the birth of your baby? Of the participants who screened positive for depression or anxiety prenatally, 64 (57%) reported they thought they needed help with depression, anxiety, or stress during pregnancy. Of the women who screened positive on the postpartum questionnaire, 27 (53%) reported they thought they needed help with depression, anxiety, or stress since the birth of the baby. Conversely, only about half of the women (53%, n = 64) who said they needed help during pregnancy screened as positive for depression or anxiety. The other half (47%) felt a need for help but did not screen positive for depression or anxiety. Of the women who both felt they needed help and screened positive for anxiety or depression during pregnancy, 30% received treatment, 36% were referred for mental health or social services (half accessed the referral and half declined), and 34% received no treatment or referral.
In the postpartum period, 27 women (64%) who said they needed help since the birth of their baby screened as depressed or anxious. In all, 50 of the 121 women (41%) who felt they needed help for depression, anxiety, or stress during the pregnancy received help (i.e., received either treatment or a referral that was accessed). At the postpartum assessment, 13 of the 42 women (31%) who felt they needed help received it. Of the women who both felt they needed help and screened positive for anxiety or depression at 6 weeks postpartum, 37% received treatment, 8% were referred for mental health or social services, and 55% received no treatment or referral. Figures 3 and 4 outline the findings regarding screening results and documented treatment and referral according to participants' responses to the questions of whether they thought they needed help for depression, anxiety, or stress at the prenatal and postpartum time points.
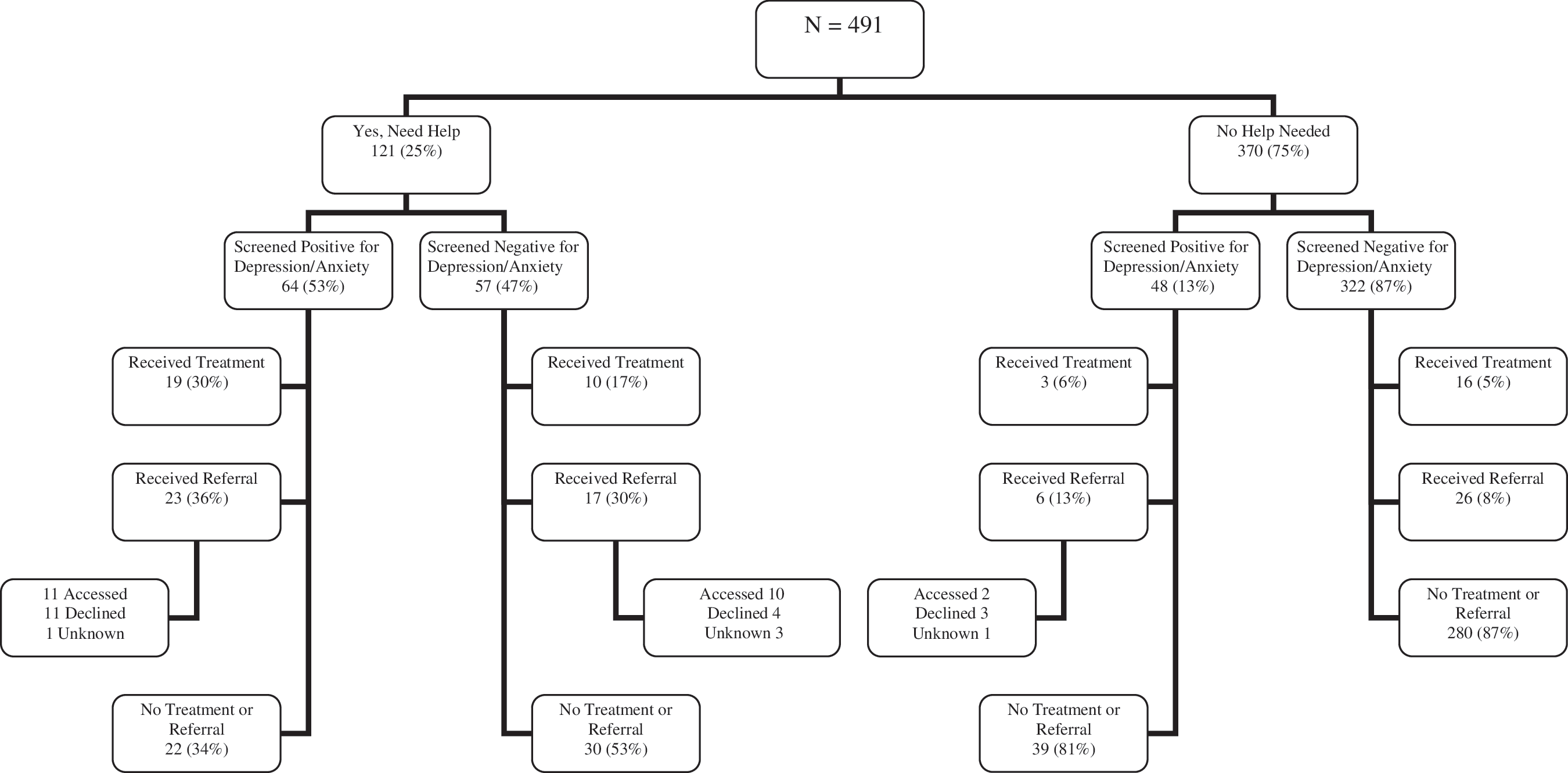
Screening results and documented treatment and referral according to participants' self-identified need for help with depression, anxiety, or stress during pregnancy.
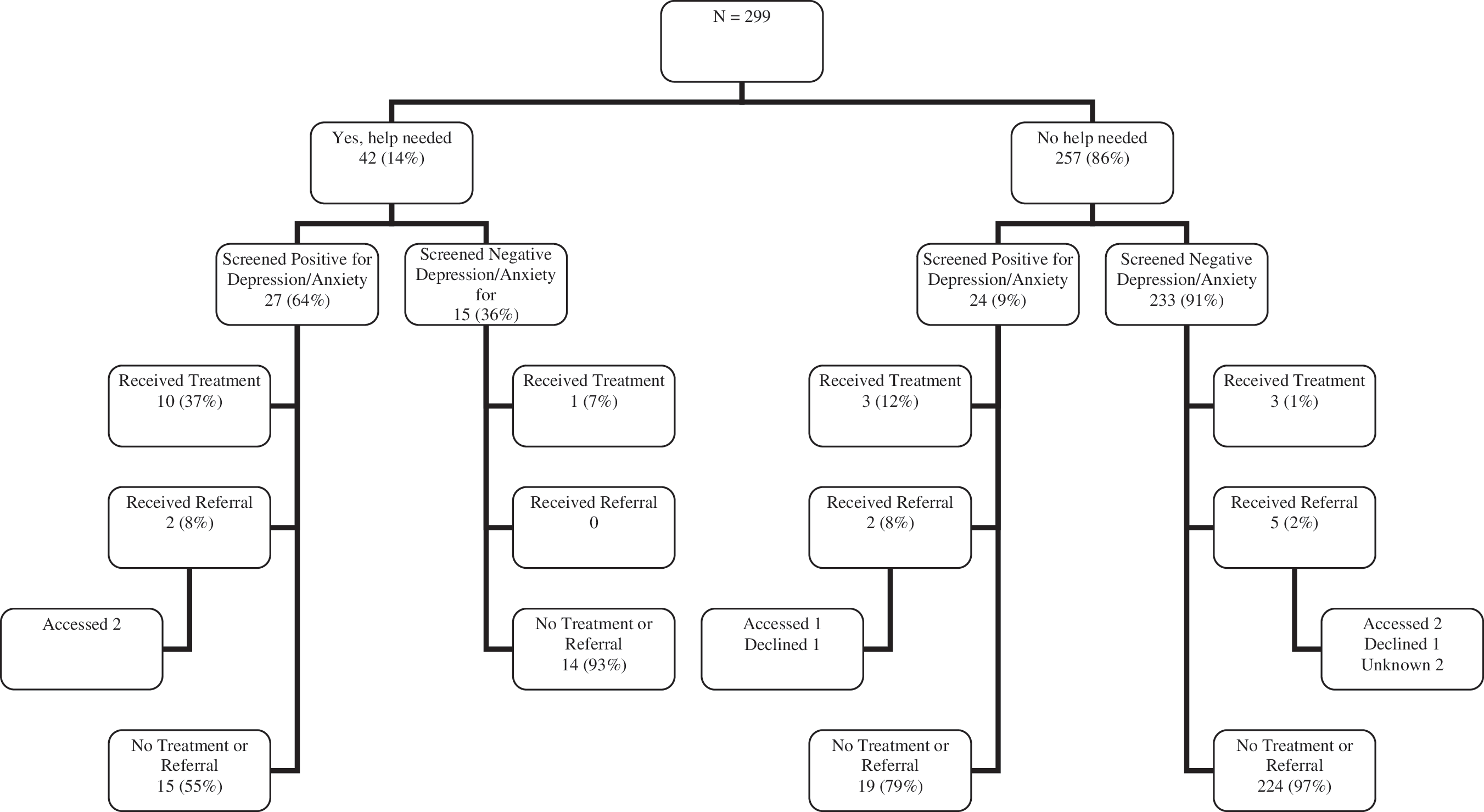
Screening results and documented treatment and referral according to participants' self-identified need for help with depression, anxiety, or stress during the postpartum period.
Discussion
To our knowledge, this is the first study to use medical records to investigate obstetrical provider identification of psychiatric symptoms, treatment, and referral at two separate periods across the perinatal period (both prenatally and postpartum) of women identified with depression or anxiety using validated screening instruments. Previous studies have used medical record examination in conjunction with screening at a single time point, whereas the approach used in this study allowed for a more comprehensive view of women's symptoms of depression and anxiety over time and the detection by obstetrical providers over the period in which obstetrical care was provided.
Findings from this study show that depression and anxiety among perinatal women in obstetrical care are quite prevalent and are largely undetected and untreated by providers. These findings echo previous reports showing that in the absence of systematic screening, most perinatal mood disorders are not detected by obstetrical providers. The importance of screening for psychiatric disorders during the perinatal period is beginning to receive more attention 72,73 and has been identified as a critical public health issue. 74 Findings about the discrepancy between the number of women identified with depression and anxiety using screening instruments and the number of women identified by clinicians without a screening tool highlight the usefulness of screening tools, such as the EPDS and the PHQ, in identifying women who may require psychiatric treatment and the importance of structured screening for case identification. Researchers have demonstrated that the use of structured assessment and screening in postpartum care settings led to increased rates of detection of postpartum depression compared with the use of unstructured clinical interviews. 75,76 The same is likely to be true for prenatal settings. Routine screening for postpartum depression is recommended, 13 and federal legislation is currently under consideration in the United States that would make screening for postpartum mood disorders mandatory. 77 Studies have reported that screening for depression and anxiety prenatally and postpartum is feasible and acceptable to women. 10,78 –80
The study findings have implications for determining the optimal time for screening. Only a small percentage (9%) of women who screened negative for depression/anxiety prenatally screened positive at 6 weeks postpartum. On the other hand, almost half of the women who screened positive postpartum had screened positive prenatally. This finding is in line with previous studies that have identified depression/anxiety during pregnancy as one of the greatest predictors of postpartum depression. 25,27 Early identification and effective management of prenatal depression and anxiety would have the greatest overall impact and minimize negative effects for mother and baby. Prenatal screening in obstetrics can identify women who may be at risk for adverse pregnancy outcomes, enabling appropriate treatment and monitoring. In addition to identifying women who may meet diagnostic criteria for these disorders, identification of women with elevated symptoms of depression or anxiety allows providers to monitor closely for change in status that may increase the risk for adverse outcomes. 78 Screening for depression and anxiety symptoms during pregnancy can also identify women at high risk for postpartum depression, as many women who develop postpartum depression have symptoms during pregnancy.
The frequent comorbidity between depression and anxiety found in this study highlights the need to include screening for anxiety disorders along with depression screening. Previous research has shown that comorbidity during pregnancy vs. depression or an anxiety disorder alone is uniquely associated with elevated cortisol and pregnancy-related distress 81 and that, in women with postpartum depression, comorbid anxiety symptoms were associated with a poorer prognosis. 82 The proportion of women in our study who screened positive for an anxiety disorder using the PHQ was comparable to those in other studies 9,12,83 but lower than the findings in some other perinatal studies. 38,84 These varied findings may reflect the lack of standardized instruments specific to measuring anxiety in pregnancy and postpartum, as there are currently no brief screening instruments designed specifically to assess anxiety symptoms among pregnant or postpartum women. 37,85 The participants' responses to individual items on the PHQ anxiety subscales showed that a high proportion of women endorsed significant symptoms of anxiety both prenatally and postpartum but without meeting diagnostic criteria for anxiety disorders. The PHQ provides a dichotomous positive or negative evaluation for the anxiety disorders it measures but does not give a measure of symptom level or severity. It may have been more useful to measure symptom levels of anxiety, as this would also have provided an indication of subclinical levels of anxiety and, therefore, would identify women for whom continued monitoring may be indicated.
The proportion of women who reported they felt a need for help with depression, anxiety, or stress was similar to the proportion of women who screened positive for depression or anxiety at the same times (25% reported a needed for help prenatally, and 23% were positive for depression or anxiety; 14% reported a need for help during the postpartum, and 17% were positive for depression or anxiety). This would suggest that many depressed or anxious women were aware of the need for help and wanted it. A closer look, however, revealed that not all women who screened positive felt a need for help: 13% of pregnant women and 9% of postpartum women who screened positive for depression/anxiety did not report feeling a need for help with depression, anxiety, or stress. This suggests a few possibilities. Many depressed/anxious women may not recognize a need for help, either because they are accustomed to feeling poorly, they believe that the symptoms they are experiencing are a normal or expected part of pregnancy or early motherhood, or they recognize that something is wrong but think they can manage without help. On the other hand, there were many women who screened negative for depression/anxiety but who reported feeling a need for help (47% prenatally, 36% postpartum), suggesting that there are even more women who are feeling the need for and wanting some kind of help for depression, anxiety, or stress who are not being identified by screening instruments or by providers and are, thus, not getting help. The need for mental health services may be far higher than we think. In this study, of the women who reported feeling a need for help, only 41% of prenatal women received help, and only 31% of postpartum women received help.
An essential next step in managing perinatal depression/anxiety will be to move from screening to improved rates of treatment and, ultimately, improved outcomes for affected women. An important finding in this study is that when providers detected symptoms of depression or anxiety in their patients, treatment or referral most often followed. Eighty percent of women identified by providers as having psychiatric symptoms during pregnancy had documentation of treatment or referral, and all of the women identified as symptomatic during the postpartum period had documented treatment or referral. This suggests that providers are doing well with treatment or referral once depression or anxiety is detected. In this study, the problem was not so much in ensuring that women identified as symptomatic received treatment or referral to psychiatric or social services but rather that women were not identified in the first place. This finding adds further weight to the argument for systematic screening.
Engagement in treatment is important, as untreated perinatal depression/anxiety can have negative effects on both mother and child. In this study, only 50% of the women who received a referral accessed it, suggesting that more work needs to be done to increase rates of treatment engagement as well as to ensure follow-up of women who decline or are unable to access referrals. In a recent report from the larger study of which this report was a part, women identified lack of time, stigma, and child care issues as the greatest perceived barriers to obtaining mental healthcare for perinatal depression/anxiety. 86 Understanding what prevents women from seeking or obtaining mental health help can be used to improve access to mental health treatment and support for childbearing women. Once depression is identified, collaborative care or care management programs have been shown to greatly improve outcomes in general primary care patients with depression or anxiety. 87 Perinatal depression care management has been shown to be feasible, 50 and systematic screening and provider notification of depression results have shown modest increases in depression treatment uptake. 74 Programs or pathways to manage care of perinatal women identified as depressed or anxious need to be developed and tested as the next step in improving healthcare quality and women's mental and emotional well-being.
Limitations
The study sample was predominantly well educated, partnered, and of high SES, which limits the generalizability of the findings. Although the initial agreement rate was relatively high, systematic bias in participation may be present and is a limitation of the study. In addition, only 60% of participants completed the 6-week postpartum questionnaire, and the completers differed from noncompleters in race, income, education level, and age, which may have biased the results and may further limit the generalizability of these findings. Insurance information was not collected, thus presenting a limitation in terms of understanding any impact that this may have had on referral and treatment rates. The EPDS and the PHQ are screening instruments and do not give a clinical diagnosis but only the likelihood of a psychiatric disorder. A structured diagnostic interview to ascertain depression and anxiety disorder diagnoses would have strengthened the study. Evaluation of treatment of psychiatric disorders during pregnancy reflects any overall treatment, whether treatment began before pregnancy or during pregnancy and whether initiated by the obstetrical provider, by another provider, or by the participant herself. Delineating when treatment began would further describe care patterns.
Identification, treatment, and referral rates may be underestimated, as they reflect only what was noted in the EMR. Specifically, psychiatric provider notes are not included in the EMR, and, therefore, some psychiatric service use data may be missing; however, documentation of referral and treatment would likely be indicated in the obstetrical provider notes or social worker notes, which are included in the EMR. On the other hand, rates may be overestimated, as wide latitude was given for identification (even notation of one symptom) and whether recorded treatment actually took place was not verified. In addition, even though some women received treatment, we do not know if the treatment was effective. Although a measurement of treatment outcome could be inferred from persistence or remittance of symptoms, the study did not assess adequacy or effectiveness of treatment received by participants.
Conclusions
The majority of women who screened positive for an anxiety disorder or high levels of depressive symptoms were not identified by their providers during pregnancy or postpartum. Only 15% of positively screened participants had evidence of any mental health treatment in their EMR during pregnancy, with equally low rates of referral to mental health or social services. In the postpartum period, only 25% of positively screened postpartum women received treatment, and an additional 2.5% were referred. A low proportion of women who reported they felt a need for help with depression, anxiety, or stress prenatally or postpartum received treatment or referral. These findings indicate that obstetrical providers' detection of perinatal depression and anxiety is seriously lacking, resulting in low rates of treatment or referral. This problem must be addressed in order to provide the care that childbearing women need and want.
Footnotes
Acknowledgments
This study was supported by a Sharon Davies Memorial Research Award from the Freedom from Fear Foundation (J.H.G.) and from an MGH Institute of Health Professions Faculty Research Fellowship (J.H.G.). We would like to acknowledge the following MGH Institute of Health Professions graduate nursing students who assisted with data collection: Jessica Gould, Alison Bates, Maeve Dargush, Isis Lucia, Neena Philip, Kerry Decker, Tricia Keogh, and Anita Pandofe-Ruchman.
Disclosure Statement
The authors have no conflicts of interest to report.