
Abstract
Interest in preconceptional healthcare was advanced by release of the recommendations of the Centers for Disease Control and Prevention (CDC) and its Select Panel on Preconception Care in 2006. With increasing interest, apprehension surfaced from healthcare professionals, women, and the public at large. The most common themes of concerns are that an emphasis on preconception care is pronatalist, unnecessary, exclusive of men, framed too narrowly, doomed to failure because of competing clinical demands and influences, and involves a vocabulary that is meaningless to the public. This article explores the themes and argues that none of them are fatal to moving forward with a preconception agenda—rather, they should stimulate thoughtful response, careful framing, and vigilance for unintended consequences related to restructuring the basic perinatal prevention paradigm from a prenatal care approach to a women's wellness model.
Introduction
More than 20
The importance of this reorientation is underscored by the recognition that in obstetrics, most of our patients' outcomes or their determinants are already present before we welcome a woman to her first prenatal visit. Examples include intendedness of the conception, the interpregnancy interval, maternal age, conception through ovulation stimulation or assisted reproductive technology, abnormal placentation, prepregnancy chronic disease control, fetal anomalies due to abnormal organogenesis, and timing of entry into prenatal care. Once prenatal care begins, it is not possible to change whether the pregnancy was intended, the length of the interpregnancy interval, the mother's age, her exposures during the critical periods of organogenesis, or any of the other factors related to increased risk for poor pregnancy outcomes. Prenatal care is, for the most part, a program of surveillance; in contrast, preconceptional health promotion offers an avenue for the primary prevention of many poor pregnancy outcomes.
Efforts to change the prevention paradigm to one that acknowledges and addresses the importance of a woman's health and habits before and during the earliest weeks of pregnancy are not new, 10 but progress in altering the nation's approach to the prevention of reproductive casualties has been slow. 7,11 National attention toward the importance of the preconception period was significantly advanced when the Centers for Disease Control and Prevention (CDC) convened a Select Panel on Preconception Care in 2005. Subsequently in 2006, a definition of preconception healthcare was put forward by the group: “Preconception care is a set of interventions that aim to identify and modify biomedical behavioral and social risks to a woman's health or pregnancy outcome through prevention and management. … Preconceptional care is more than a single visit to a health care provider and less than all well-woman care.4p4
The CDC and its Select Panel also formulated four goals for preconception health
4
: Improve the knowledge, attitudes and behaviors of men and women related to preconceptional health. Assure that all women of childbearing age in the United States receive preconception care services (i.e., evidence-based risk screening, health promotion and interventions) that will enable them to enter pregnancy in optimal health. Reduce risks indicated by a previous adverse pregnancy outcome through interventions during the interconceptional period that can prevent or minimize health problems for a mother and her future children. Reduce the disparities in adverse pregnancy outcomes.
After the release of the CDC and Select Panel report, national work groups were established, state task forces were formed, local, state, and national meetings were convened, and hundreds of talks were given to educate providers and the public about the importance of the preconception period. With increasing energies to change the perinatal prevention paradigm to emphasize a woman's health before pregnancy, recurrent themes of concern surfaced from healthcare professionals, women, and the public at large. The most common themes are: Preconception health is being structured as a clinical initiative, but there are many other equally or more important influences. Preconception health is pronatalist, as it assumes future childbearing and has the potential to frame women as vessels for growing healthy offspring. Women are already getting the care that they need, which makes this initiative unnecessary. Because women do not plan their pregnancies, preconceptional healthcare is unlikely to have a positive impact on outcomes. Men are important to reproduction—why are they excluded from this initiative? The word “preconception” is meaningless to the public. “I (we) already have too much to do, so this initiative is doomed for failure.”
Each of these themes has the potential to undermine enthusiasm for broadening the perinatal prevention paradigm to one that begins with women's health before pregnancy and to derail related opportunities for primary prevention. On the other hand, careful examination of the detractors may result in strengthened momentum and a broadening of the platform for changing the nation's approach to preventing reproductive casualties. The rest of this article explores the themes and argues that none of them are fatal to moving forward with a preconception agenda.
Theme 1: Preconception Health Is Being Structured as a Clinical Initiative, but There Are Many Other Equally or More Important Influences
Although the scientific foundations for addressing the preconceptional health status of women come from the clinical arena, the new paradigm cannot and should not expect clinical encounters alone to make a significant difference in the health status of women of reproductive age. Nothing inherent in the CDC and Select Panel preconception health initiative suggests that only clinical activities are of value. Recognizing the need for broad involvement, the CDC included 23 national organizations representing consumer, nonprofit, government, and clinician interests in formulating the national recommendations. The resulting document acknowledges in its title, Recommendations to Improve Preconception Health and Health Care, that although clinical care is important, it does not and cannot stand alone. 4 The specific recommendations put forth by the CDC and Select Panel 4 are targeted to consumers and the public at large, the public health arena, financial systems and payers, researchers, and clinicians. The recommendations, separated into focus areas, are shown in Figure 1.

Summary of Centers for Disease Control and Prevention/Select Panel's recommendations to improve preconception health and healthcare by focus.
To be successful, the responsibility for achieving higher levels of wellness cannot rest with clinicians alone. Figure 2 illustrates the complexity and interrelatedness of influences on women's health status and highlights that health is a function of the interplay between an individual and her various environmental exposures, interpersonal networks, and institutional influences. 12 This inclusive consideration of influences on health status is identified as the ecological framework; in 2002, the framework gained traction when the Institute of Medicine released a report supporting that the health of populations and individuals is shaped by a wide range of factors in the social, economic, natural, built, and political environments that interact in complex ways with each other and with individual traits, such as race, sex, and genetics. 13
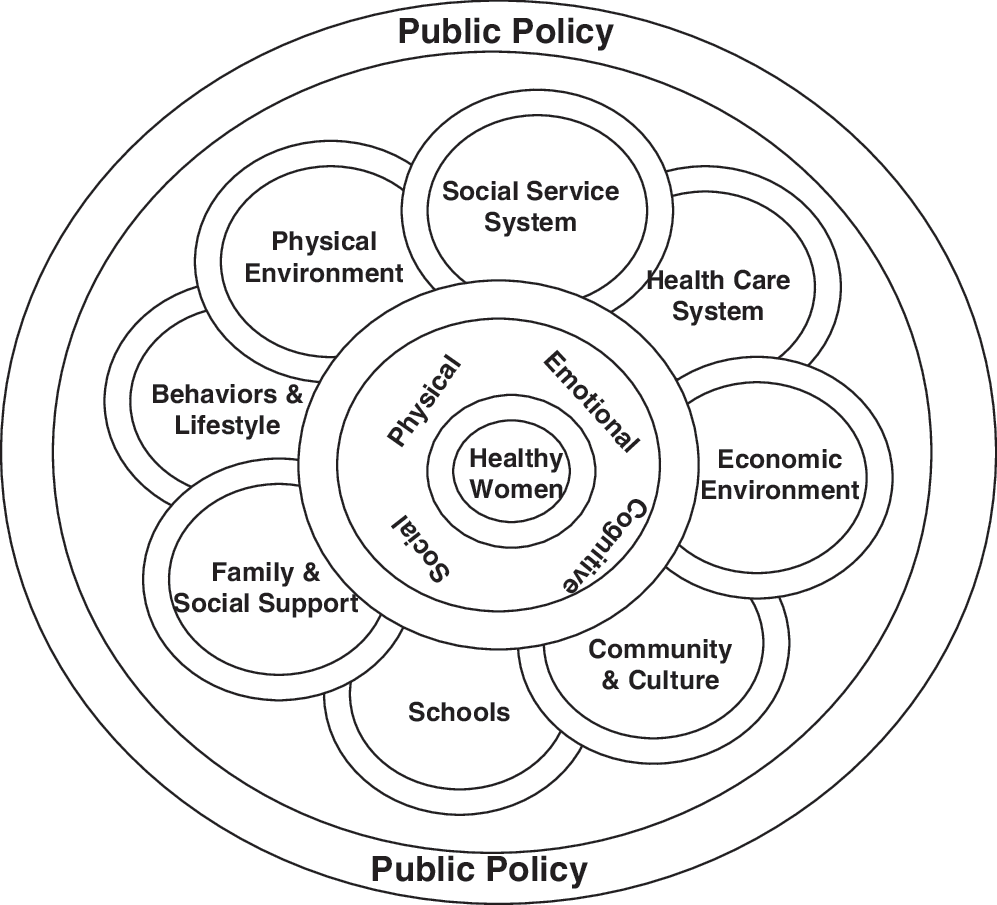
Influences on women's health. Adapted from Delaware Children's Health Chartbook, 2005, with permission of The Nemours Foundation, Division of Health and Prevention Services.
Recognizing the limitations of clinical care suggests some relief from total responsibility for those primarily engaged in clinical activities as well as partnerships that need to be not only forged but embraced if higher levels of health are to be achieved. The influence of the clinician should not be lost in the complexity of the influences on health behaviors and health status, however. Studies report that provider recommendations are critical to the adoption of health promoting behaviors 14,15 and such health protecting behaviors as smoking cessation. 16 Thus, success in promoting health for a specific individual is dependent on an intersection of clinical guidance and support, individual motivation, and social and environmental context.
Theme 2: Preconception Health Is Pronatalist and Has the Potential to Frame Women as Nothing More than Vessels for Growing Healthy Offspring
Preconception health is not a pronatalist initiative but, rather, a women's health agenda. There is little that could be recommended in routine preconceptional counseling that would not benefit the general health of all women of reproductive age, irrespective of eventual conceptions. 8,11 Attention to health education and disease prevention activities is frequently concentrated in prenatal care. This concentration diminishes the value of the woman's own health and too often results in missed opportunities for prevention. By emphasizing the promotion of women's wellness at every encounter, the potential to impact the health and well-being of women themselves exists; through this potential, higher levels of preconceptional wellness for more women who conceive will be achieved, and their risks for poor pregnancy outcomes will be reduced. 8
Major determinants of poor health status in women are also important risk factors for poor pregnancy outcomes. For instance, tobacco has been identified as the largest preventable cause of death and disability in this country 17 ; tobacco use in pregnancy increases the risk of low birth weight, prematurity, and placental abnormalities. 18 Using evidence-based tobacco cessation interventions with each woman who smokes 19 irrespective of childbearing desires is appropriate for her own health; should she become pregnant, the benefits are expanded. Similarly, obesity is known to be associated with the development of many chronic diseases and numerous disabilities; pregnancies occurring in obese women are at increased risk for numerous complications. 20 To prevent or positively impact obesity in women, irrespective of conception plans, is likely to impact the woman's health for a lifetime; should she become pregnant, the benefits are again expanded. Assessing and addressing a woman's alcohol and other drug use, intake of specific nutrients, use of multivitamins, physical activity, and immunization status have the potential to improve a woman's health status and risks for future disease, which is, in and of itself, an important outcome.
Theme 3: Women Are Already Getting the Care They Need, so This Initiative Is Unnecessary
Although it is true that women are participating in clinical encounters, it does not necessarily follow that they are receiving preventive care or health promotion counseling. National data estimating ambulatory medical care use find that women aged 15–44 average 3.8 medical visits each year. 21
Clear expectations about the content of preventive care exist. For instance, the American College of Obstetricians and Gynecologists (ACOG) recommends that all women from age 13 onward receive a dietary/nutrition assessment and have their body mass index (BMI) computed. ACOG also recommends that periodic assessments include review of tobacco, alcohol, and other drug use, evaluation for domestic and dating violence, assessment of calcium intake, discussion and assessment for sexually transmitted diseases (STDs), and prevention of unwanted and unintended pregnancies, including the use of emergency contraception. 22
Despite recommendations, evaluation of the care women receive suggests that opportunities for promoting preventive health practices among women are largely missed. In 2005, the Kaiser Family Foundation reported on its survey of 2766 women aged ≥18. The survey found that just over half of the of the women (55%) had talked to a doctor or nurse in the previous 3 years about diet, exercise, or nutrition; <50% had talked about calcium intake (43%), smoking (33%), and alcohol use (20%). Only 31% of women between the ages of 18 and 44 had talked with a provider about their sexual history in the preceding 3 years; discussions of related topics, such as sexually transmitted infections (STIs) (28%) and HIV/AIDS (31%), were even more rare. Emergency contraception was included in the content of care for 14% of the women, and domestic and dating violence was addressed for 12%. 23
Other studies echo missed opportunities. Five hundred middle-class, educated women between the ages of 18 and 45 were enrolled between 2004 and 2005 in a study to assess women's interests, knowledge, and experiences regarding preconceptional health promotion. 24 Nearly all the women (98.6%) recognized the value of optimizing health prior to conception, but only 39% recalled their clinician ever addressing the topic. Two thirds of the women expressed interest in receiving preconception health education, and the majority desired that the information be delivered by their primary care provider, including obstetricians/gynecologists (95.3%). In another study, the experiences of 1325 diverse women of childbearing potential who participated in a cross-sectional random-digit telephone survey in Central Pennsylvania were explored. 25 Only half of the women at risk for conception reported receiving counseling about pregnancy planning or contraception in the prior year; one third of the women did not receive any routine physical examination or screening services (pelvic examination, breast examination, Pap smear, and blood pressure measurement) during the preceding 12 months, and 57% of the sample reported receiving no health counseling or counseling about the following topics: tobacco use, dietary intake, physical activity, alcohol and other drug use, safety and violence concerns, STI, or stress and stress management.
It is possible to assume that women in the various studies simply do not recall the content of their encounters. However, the findings of a chart audit of the content of care included during routine gynecology visits support the lack of attention to many important health promotion topics, such as nutritional status (81% of records contained no documentation of this), and disease prevention topics, such as medical history (85% of records did not include documentation of the woman's prior medical profile). 26
As early as 1990, Jack and Culpepper 27 recommended that preconceptional care be made available to all women and their partners as an integrated part of primary care and that it also become a routine component of all initial and annual family planning visits. To date, there is no evidence that women are routinely receiving the care they need to promote their own health or the health of any future conceptions should they become pregnant.
Theme 4: An Emphasis on Preconceptional Healthcare Will Have No Impact Because Women Do Not Plan Their Pregnancies
An important outcome of preconceptional health promotion activities would be reduction of the nation's unintendedness rate. In the latest National Survey of Family Growth, 49% of pregnancies were identified by woman as unintended (either unwanted or mistimed). 28 Of these pregnancies, 44% ended with birth; 42% ended in abortions, and 14% ended with fetal losses. 28 Unintended pregnancies occur because of lack of contraception, imperfect use of contraception, and contraceptive failure. The latter two causes are significant because nearly one half of all unintended pregnancies occur in women who used some method of contraception in the month they conceived. 28
All healthcare visits before pregnancy offer an opportunity to educate about the advantages of intended conceptions and to provide health promotion education to all women, irrespective of their declaration of intent to conceive in the near or distant future. Cognizant that nearly 50% of pregnancies in this country are unintended, the CDC and Select Panel recommend that each woman, man, and couple be encouraged to have a reproductive life plan. 4 The concept of a reproductive life plan is an attempt to formalize patient-centered contraceptive care: listening to and talking with patients about their reproductive goals, helping them understand their pregnancy risks, matching contraceptive choices to personal goals, and helping them access and effectively use their chosen method. 29,30 In 2006, ACOG recommended that discussion of reproductive health plans be a routine component of care for all women aged 19–39. 23 Model reproductive life plans have been put forth, 30 but they have not yet been evaluated for effectiveness. 8 Numerous benefits have been postulated that include increased efficiencies in meeting women's reproductive healthcare needs. 30
Focusing on the 50% of pregnancies that are uninintended begs the question about the other half of conceptions. Intentions about the subsequent conception do not imply either proactive planning or adequate knowledge to make informed decisions about personal health, behaviors, or exposures. Work is needed to understand the intertwined but likely distinct concepts of intendedness, which represents an attitude, and planned pregnancy, which suggests proactive behaviors. While waiting for a body of research that adequately explains these concepts, creative strategies to reach all women and men with information about the importance of the earliest weeks of pregnancy are needed so that those who do intend to become pregnant are aware of beneficial behaviors.
Theme 5: Why Aren't Men a Part of the Preconception Agenda?
Although this agenda, like prenatal care, focuses on women, it opens the door much wider than the traditional prenatal approach to acknowledge and address the health needs of men. As demonstrated by the first goal, the CDC Work Group and Select Panel were deliberately inclusive of both men and women. 4
The benefits of targeting men are fundamental and growing. At least six potential advantages have been identified
31
: Engaging men in the preconception health promotion agenda is critical to addressing the unintendedness rates in this country. As sperm DNA can be damaged in many ways, assessing and addressing a man's health and exposures prior to attempted pregnancy may improve the likelihood of conception and healthy pregnancy outcomes. Preconception care encourages the screening and treatment of STIs in the male, thereby impacting the preconceptional health status of the female. Educating men about the importance of a woman's health status prior to pregnancy may result in greater support of good health practices in the partner, such as smoking cessation and healthy nutrition. Introducing the importance of deliberately deciding before a conception if and when one would like to become a father or father to additional children may impact future involvement in pregnancy and childrearing. As with women, a clinical orientation toward the importance of men's prepregnancy decisions and health status may result in higher levels of wellness for all men of reproductive potential irrespective of eventual conceptions.
No consensus exists on how to effectively reach men with preconception information and interventions. 31 In addition, numerous barriers exist, including access and use of preventive services by men, reimbursement structures, and training of healthcare providers. Nonetheless, the preconception agenda provides a platform of inclusion rather than exclusion of men. It invites a much more fundamental recognition of the importance of men in the health and well-being of the next generation.
Theme 6: The Word “Preconception” Is Meaningless
Many have suggested that because the word “preconception” is meaningless to the majority, the concept can have no traction. Preconception is a clinical term, literally meaning “before conception.” There is no reason to assume or hope that the word “preconception” or its meaning currently resonates with the public; there is also no reason to recommend abandonment of a service because the clinical vocabulary is not understood by the targeted population. Many if not most terms in the clinical lexicon are not understood by the public. For example, terms associated with cervical cancer screening, such as dysplasia and ACUS, are not readily understood by women who have been tested or who have abnormal findings. However, we do not choose to stop providing cervical cancer screening because women do not understand either the test or its potential findings. Rather, we listen to and learn from the public about how to label and discuss clinical concepts so that we can translate them to be both accessible and meaningful.
A specific word is less important than how a concept is understood and interpreted. Research from focus groups presented to the Select Panel on Preconception Care provided the following insights about framing the preconception concept 32 : women do not want to be framed as a vessel whose purpose is to someday have a healthy child, the motivational message of engaging in health promoting behaviors “just in case you could become pregnant” is not compelling, and women want nonpregnancy-related reasons for performing health promoting behaviors.
We do not currently understand the best verbiage for promoting a woman's health for her own short-term and long-term needs and for the health of any pregnancies and offspring she may have. This deficit in our understanding does not suggest that we throw the concepts and goals away; rather, it suggests that we work with our patients and with researchers to find a meaningful language for communicating with women, men, and communities about the intergenerational value of high levels of wellness for all women. The discovered language may also prove useful in mobilizing public opinion leaders, policymakers, and third party payers to consider the advantages of the health of today's citizenry for the health of tomorrow's citizens. The best vocabulary is unlikely to be universal—what resonates with and motivates members of one group or community may not have equal resonance with another population. The many target populations identified by the CDC and Select Panel, 4 including male and female patients, the public at large, researchers, clinicians, and financial gatekeepers, will need to inform the architects of outreach efforts, attitudinal and behavioral strategies, and clinical and community interventions about how to articulate the meaning and purposes of the new prevention emphasis if it is to achieve its potential.
Theme 7: “I (We) Already Have Too Much to Do”
The final theme is a powerful detractor and one that nearly all clinicians express. Current workloads and poor reimbursement make the suggestion of even one more clinical activity overwhelming.
Our current approach to the healthcare of women is built on healthcare silos, such as contraceptive services, obstetrical services, well woman care, specialty services, and chronic disease care. In women's health, fragmentation often is divided between reproductive and nonreproductive functions, which has the potential to miss important considerations in the total health of the woman and to cause unnecessary risks for women, their future pregnancies, and their future children. 33 For instance, women with preexisting diabetes mellitus are more likely to have healthy pregnancies and offspring if they conceive after tight control of their blood sugar has been achieved. 34,35 However, studies demonstrate that women do not receive contraceptive guidance from their endocrinologists, and they do not receive disease control advice from the providers who provide contraceptive care. 36 The result is that women and fetuses are placed at risk despite medical encounters. Care provided to women with diabetes provides a well-documented example of fragmentation, and innumerable other examples exist, particularly the prescription of potentially teratogenic drugs to women at risk for pregnancy.
Although the CDC and its Select Panel on Preconception Care put forward goals and specific recommendations for impacting the routine provision of preconception care, they were unable to add minutes to the day or change the demand for clinical productivity imposed by today's payers. This reality suggests that altering what we already do to “work smarter, not harder” is the only option currently available for incorporating the preconception agenda into the care we provide. What is not needed for the majority of women is further fragmentation of our healthcare delivery system through creation of a new service or silo called the preconception visit. Such an approach would prove expensive and would likely miss the majority of women who become pregnant each year. A special preconception visit is, indeed, appropriate for women with complex medical and reproductive risks, but there is nothing to recommend this strategy as the access point to important health promotion information for the majority of women and couples. 30 For most women, what is needed is a conscious determination to provide preventive services to “every woman, every time,” a concept first proposed by the California Preconception Initiative. 37 The simple imperative is designed to take advantage of all healthcare encounters to stress prevention opportunities throughout the life span and to address conception and contraception needs and choices at every encounter. This involves all medical specialties, not only those directly involved in reproductive health.
Ideas to move the imperative forward are being tested across the nation. They involve activities outside the examining room, such as social marketing, community outreach and education, and the development of educational pamphlets and posters that highlight and motivate women to be deliberate about choices that put them at risk for an unintended pregnancy. Many educational tools are already available from the March of Dimes Foundation at
To help clinicians anchor themselves in what the evidence says about the clinical content of preconception activities, the Clinical Committee of the CDC's Select Panel for Preconceptional Health systematically reviewed all of the available evidence in a 2008 supplement to the American Journal of Obstetrics and Gynecology.
38
The 17 articles are available on line at
Conclusions
It is rare in our complex healthcare system that the opportunity to redefine a basic construct of health comes along. In the next few years, exciting opportunities to further advance the preconceptional health and healthcare initiative through clinical, public health, and public policy activities will surface. As the nation moves forward, energy must be directed at creating a strong, comprehensive, and accessible framework 39 that avoids categorical silos, that maximizes continuity, 33 and that rewards primary care and preventive services. 7,40
We are certainly not there yet. Clinicians are essential to moving the initiative forward through advocacy for public policy and payer changes, by supporting social marketing messages, and by integrating relevant preventive care into their routines. An activity as simple as recommending a multivitamin with folic acid to every woman from menarche through menopause has the potential to make a difference for women, for the pregnancies they may conceive, and for the children they may have. 8 As two proponents of preconceptional health have succinctly noted, if you see women of reproductive age, it is not a question of whether you are providing preconceptional care but, rather, a question of what kind of preconceptional care you are providing. 41
Indeed, there are themes of concerns, as there should be: alterations to paradigms require close examination. However, none of the themes represent fatal flaws within the initiative. Rather, they stimulate thoughtful response, careful framing, and vigilance for unintended consequences. The changes necessary to restructure a paradigm from a fetalcentric prenatal approach to one that has the potential to impact multiple generations can come neither quickly nor easily, but this should not dissuade us from tackling the status quo, which has proven unequal to impacting positively the preventive care needs of both women and the children in our futures.
Footnotes
Acknowledgments
I thank Irwin R. Merkatz, M.D., Peter Bernstein, M.D., and Karla Damas, PhD, organizers of the Autumn in New York Symposium, for the opportunity to participate.
Disclosure Statement
The author has no conflicts of interest to report.