
Abstract
Background:
The association between hormone therapy (HT) use and lung cancer risk is inconsistent in epidemiological studies. This meta-analysis was conducted to examine the association between HT and lung cancer risk.
Methods:
We searched MEDLINE (PubMed), EMBASE, and the Cochrane Library in April 2008. All articles searched were independently reviewed and selected by two evaluators according to predetermined inclusion and exclusion criteria.
Results:
We included a total of 11 studies (8 case-control studies and 3 prospective cohort studies), involving a total of 220,599 participants. When all studies were pooled, the odds ratio (OR) of HT use for lung cancer risk was 0.87 (95% confidence interval (CI) 0.74-1.02). In subgroup meta-analyses, there was no association among cohort studies (relative risk (RR) 1.01; 95% CI 0.74-1.38), while there was a significant association between HT use and lung cancer risk among case-control studies (OR 0.81; 95% CI 0.68-0.97) based on a random-effects model. No significant association between HT use and lung cancer risk was observed in most of the subgroup meta-analyses by methodological quality of study, type of HT use, duration of HT use, and histology of lung cancer, while significant protective effects were observed among former and never smokers except for current smokers. However, cumulative meta-analyses based on year of publication showed a distinct trend toward a protective effect of HT use on lung cancer risk in the recent studies.
Conclusions:
Overall, the findings of this meta-analysis do not support the hypothesis that there is a link between HT use and lung cancer risk. Our findings should be evaluated in further prospective cohort studies.
Introduction
Hormone Therapy (HT), which has been used to treat menopausal symptoms in perimenopausal or menopausal women, had also previously been prescribed to prevent cardiovascular disease in women without menopausal symptoms before the results of the Women's Health Initiative (WHI) were reported. However, the results from the WHI clinical trials indicated that the regimen of combined estrogen plus progestin among healthy postmenopausal women should not be initiated or continued for primary prevention of coronary heart disease (CHD). 1
Also recent epidemiologic studies and randomized controlled trials (RCTs) have reported that HT use could be a risk factor for some cancers or, conversely, a preventive factor for other cancers. According to a meta-analysis of 13 epidemiological studies, such as case-control studies and cohort studies, an odds ratio (OR) of postmenopausal estrogen therapy use was 1.16 (95% confidence interval (CI) 1.06 to 1.28) for breast cancer, and the OR for estrogen-progestin hormone therapy was 1.39 (95% CI 1.12 to 1.72). 2 Even though the evidence is limited, when combining 2 large RCTs (the Women's Health Initiative [WHI] and the Heart and Estrogen/Progestagen Replacement Study [HERS]), it was reported that the OR of HT for colorectal cancer was 0.64 (95% CI 0.45 to 0.92). 3
Furthermore, epidemiologic studies and RCTs have reported an association between HT use and risk of lung cancer in women; in most epidemiological studies, HT use was reported by using HT ever use vs. never or no use. However, those findings are contradictory. 1,4 –15 One case-control study found an increased risk, 4 4 studies reported no association 5,6,8,11 although the ORs of three of them 6,8,11 were below 1.0, and 3 studies suggested that HT use significantly decreased the risk of lung cancer in women, showing ORs in the range of 0.66 to 0.70. 7,9,10 Among 3 cohort studies, 12 –14 2 showed no association, 12,13 while a recent study reported that HT as currently used had a preventive effect on the risk of lung cancer, but did not as previously used. 14 Furthermore, 2 large randomized, placebo-controlled trials (HERS and WHI) have reported that there was no association between HT use and lung cancer risk. 1,15
To date, there is no meta-analysis published on this topic. The purpose of the current study was to examine, via a meta-analysis of epidemiological studies, the association between the use of HT and the risk of lung cancer in women.
Methods
Data sources and keywords
We searched MEDLINE (PubMed) (1968 to April 2008), EMBASE (1977 to April 2008), and the Cochrane Library (1953 to April 2008) by using selected common key words regarding HT and lung cancer in epidemiological studies such as case-control studies and cohort studies; these searches were performed by one of the authors (Dr. Myung, SK), and then confirmed by another author (Dr. Oh, SW). We also scanned the bibliographies of relevant articles in order to identify additional studies. As the keywords for the literature search, we selected “estrogen or progesterone replacement,” “hormone replacement therapy,” “postmenopausal hormone,” and “noncontraceptive hormones” for the exposure factors, and “lung cancer” and “pulmonary neoplasm” for the outcome factors.
Selection criteria
We included case-control and cohort studies reporting an association between HT use and lung cancer risk using ORs or relative risks (RRs). Only articles written in English were included in the current study. We excluded those studies that had no available data for outcome measures, the same population as another study (in this case, the first published or more comprehensive study was included in the analysis), data on mortality only, and those reporting standardized incidence ratios (SIR).
Selection of relevant studies
All studies retrieved from databases and bibliographies were independently evaluated by two authors of this paper (Dr. Oh, SW, and Dr. Myung, SK). When there were disagreements between evaluators concerning the selected studies, they discussed the matter and reached a consensus or consulted a third author (Dr, Ju, W). In cases where data were insufficient or were missing, we attempted to contact the authors of the articles in order to request the relevant data. Of the articles found in the three databases, duplicate articles and those that did not meet the selection criteria were excluded. We extracted the following data from the remaining studies: study name (first author, year of publication), journal name, country and design (project name), years enrolled, population characteristics and range of age, criteria of HT use (type of HT), OR or RR with 95% CI, and adjustment. Data abstraction was also done in duplicate, as was study selection.
Assessment of methodological quality
We assessed the methodological quality of included studies based on the Newcastle-Ottawa Scale (NOS) for quality of nonrandomized studies in meta-analyses. 16 Even though several quality assessment tools for observational studies such as NHS CRD, MOOSE, Downs and Black checklist, and the NOS are available, none has been fully validated. Among these tools, the NOS is quite comprehensive for assessing the quality of nonrandomized studies in meta-analyses. The NOS for nonrandomized studies, including case-control and cohort studies, consists of 8 items with three subscales: the selection of the study groups (4 items), the comparability of the groups (1 item), and the ascertainment of either the exposure or outcome of interest for case-control or cohort studies respectively (3 items). A “star” system of the NOS (range 0 to 9 stars) has been developed for the assessment: each study can be awarded a maximum of one star for each numbered item within the selection and exposure categories, while a maximum of two stars can be given for the comparability category.
In the current study, we considered a study awarded 6 or more stars as a high-quality study, since standard criteria have not been established, and the mean value for the 11 studies assessed was 5.7 stars.
Statistical analyses
We used adjusted data (adjusted OR or RR with 95% CI) for the meta-analysis whenever possible. We performed cumulative meta-analyses, in which the cumulative evidence at the time that each study was published is calculated. We also conducted subgroup analyses by the following: methodological quality of study; type of study design (case-controls studies and cohort studies; we classified a nested case-control study into a case-control study in the current study, in terms of the selection of cases and controls); type of HT (unopposed estrogen therapy, estrogen plus progesterone therapy, and unspecified HT); duration of HT use (short-term [< 5 years], mid-term [5–10 years], or long-term [> 10 years]); status of HT use (current users or former users); smoking status (current, former, or never smokers); and histology of lung cancer (adenocarcinoma, squamous cell carcinoma, or small cell carcinoma).
Heterogeneity in results across studies was assessed by using Higgins I2, which measures the percentage of total variation across studies. I2 is calculated as follows:
where Q is the Cochran's heterogeneity statistic and df is degrees of freedom. Negative values of I2 are set at zero, so that I2 exists between 0% (no observed heterogeneity) and 100% (maximal heterogeneity). 17 An I2 value greater than 50% represents substantial heterogeneity. We estimated a pooled OR or RR with 95% CI based on both fixed-effects and random-effects models. When substantial heterogeneity was not observed (i.e., if I2 ≤ 50%), the pooled estimate calculated based on the fixed-effects model was reported. When substantial heterogeneity was observed (i.e., if I2 > 50%), the pooled estimate calculated based on the random-effects model was reported.
We used the Woolf method (inverse variance method) for a fixed-effects analysis 18 and the DerSimonian and Laird method for a random-effects analysis. 19 Begg's funnel plot and Egger's test were used to identify publication bias. If there is publication bias, the funnel plot is asymmetrical or the p value is found to be less than 0.05 by Egger's test. We used the Stata SE version 10.0 software package (StataCorp, College Station, Texas) for all statistical analyses.
Results
Selection of studies
Our study included a total of 11 studies (8 case-control studies and 3 prospective cohort studies), involving a total of 220,599 participants, published between 1994 and 2008.
Figure 1 shows a flow diagram of the procedure used to identify the relevant studies. Searches of the three databases and the bibliographies of relevant articles yielded 392 articles. After the exclusion of duplicates (n = 45), we reviewed all the remaining screened articles (n = 347). Out of 347 articles, 330 were excluded because they did not meet the selection criteria. After the full text of the remaining 17 articles were reviewed, 11 articles were included in the final analysis. The main reasons for exclusion of studies during the final review were as follows (n = 6): insufficient data (n = 2), an identical cohort with another updated study (n = 1), data on mortality only (n = 1), or using standardized incidence ratios (SIR) (n = 2).
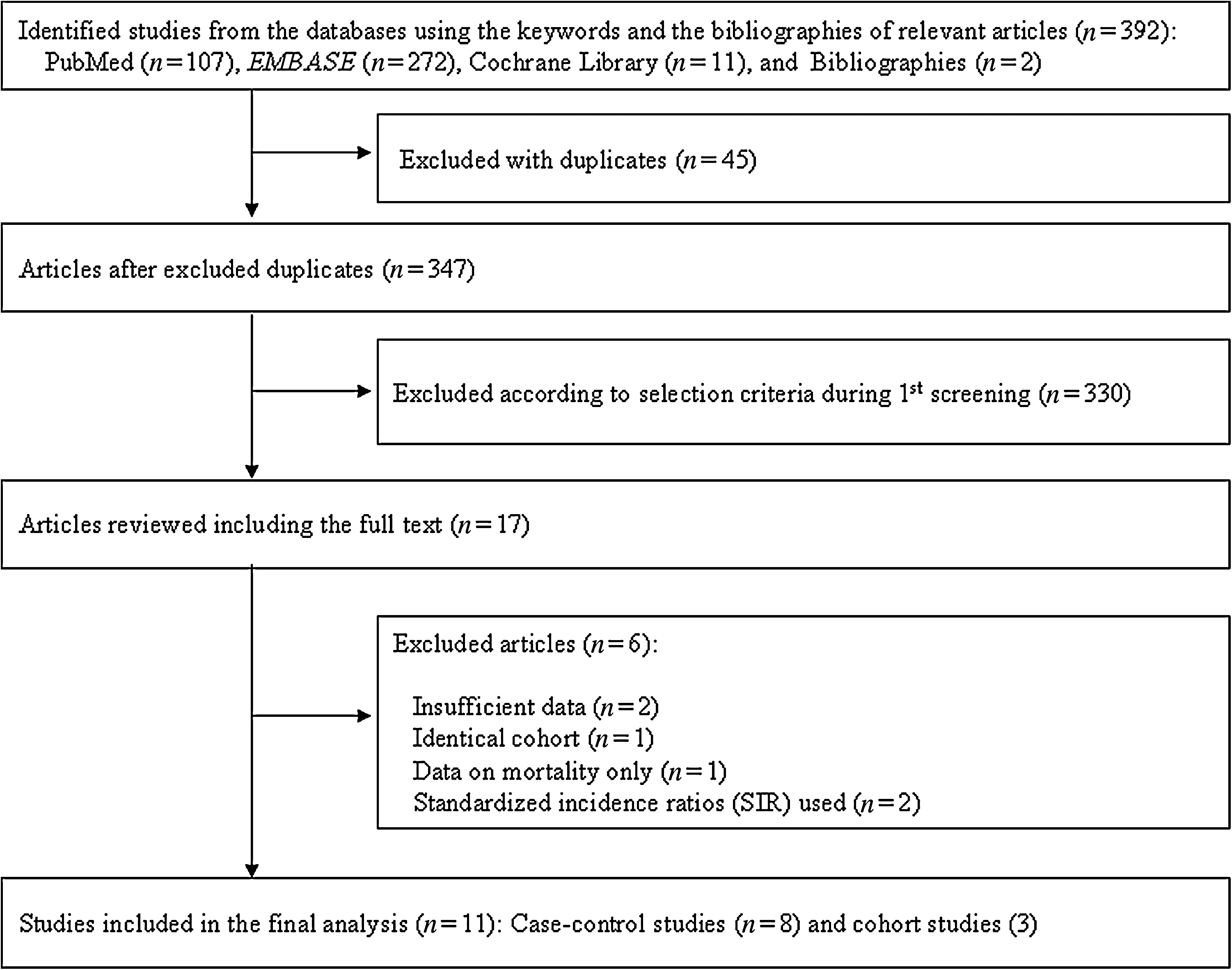
Flow diagram of identification of relevant studies.
Characteristics of studies included in the final analysis
Table 1 shows the main characteristics of all 11 studies included in the final analysis. Ten studies were published in the 2000s, while only 1 case-control study 3 was published in the 1990s. The countries in which the studies had been conducted were as follows: the United States (n = 6), 4,5,7,10,11,14 the United Kingdom (n = 1), 8 Canada (n = 1), 13 China (n = 1), 9 Germany (n = 1), 6 and Japan (n = 1). 12 Of these, five 4,5,7,9,10 were hospital-based case-control studies, two 6,11 were population-based case-control studies, one 8 was a nested case-control study, and three 12 –14 were prospective cohort studies.
HCC, hospital-based case-control study; PCC, population-based case-control study; NCC, nested case-control study; PCS, prospective cohort study; HRT, hormone replacement therapy; BMI, body mass index; CI, confidence interval; OR, odds ratio; RR, relative risk.
The range of enrollment periods for participants was from 1969 to 2006. In studies in which the age was reported, the mean age was 51 years (range, 18 to 76 years). The types of HT used were unopposed estrogen in 7 studies 4 –7,10,14 , estrogen plus progesterone in 5 studies 7,11,14 , and unspecified HT in 3 studies. 8,12,13
Methodological quality of studies
Table 2 shows the methodological quality of studies included in the final analysis. The range of quality scores was 4 to 8; the average score was 5.7. There was a significant difference in the average scores (standard deviation) between case-control and cohort studies; they were 5.25 (0.71) and 7 (1), respectively (independent two sample t-test, p < 0.01). The high-quality studies (6 or higher) included all 3 cohort studies and only 3 of 8 case-control studies.
⋆If there was no significant difference in the response rate between both groups by using a χ-square test (p > 0.05), one point was awarded.
⋆⋆A maximum of two stars can be given for the comparability category.
Overall use of HT and the risk of lung cancer
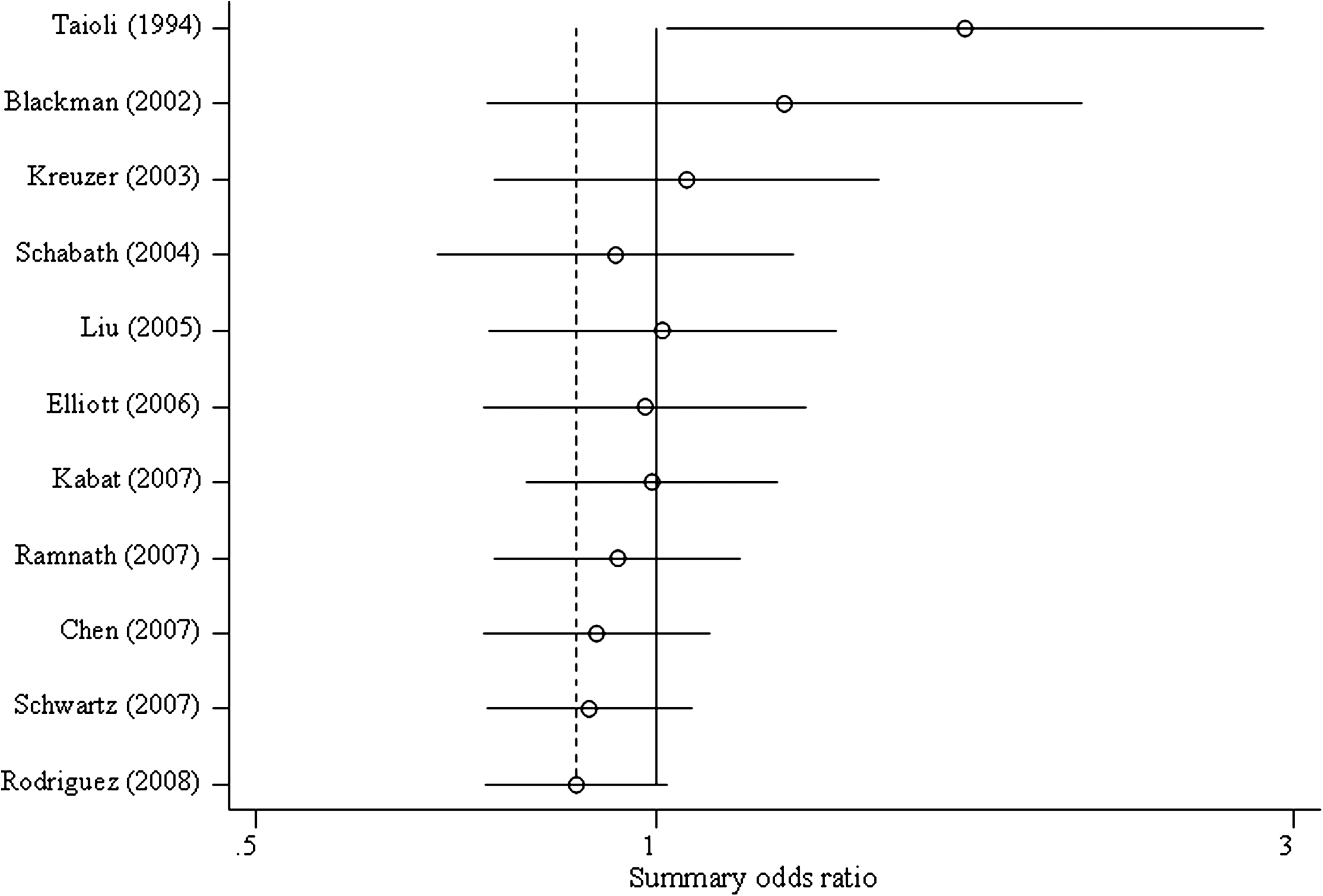
Figure 2 shows the association between HT use and lung cancer risk in a meta-analysis of all studies: case-controls studies and prospective cohort studies. In the 11 studies, the overall use of HT was not associated with the risk of lung cancer (OR 0.87, 95% CI 0.74 to 1.02, I2 = 67.7%) in a random-effects meta-analysis. No publication bias was observed in the selected studies (Begg's funnel plot was symmetrical; Egger's test, p for bias = 0.69) (Fig. 3).

Association between hormone replacement therapy (HRT) use and lung cancer risk by type of study design (n = 11). Random-effects model. OR, odds ratio; CI, confidence interval.

Begg's funnel plot and Egger's test for identifying publication bias in a combined meta-analysis of case-control and cohort studies (n = 11).
In a subgroup meta-analysis of case-control studies, HT use was associated with a significantly decreased risk (OR 0.81, 95% CI 0.68 to 0.97, I2 = 55.2%) based on a random-effects model. However, there was no association between HT use and lung cancer risk in a subgroup meta-analysis of cohort studies (RR 1.01, 95% CI 0.74 to 1.38, I2 = 80.3%) based on a random-effects model.
Cumulative meta-analyses
As shown in Fig. 4, cumulative meta-analyses indicated that there was a distinct trend toward a protective effect of HT use on lung cancer risk, especially in the recent studies published for the past 2 to 3 years.
Cumulative random-effects meta-analysis of case-control and cohort studies included in the final analysis (n = 11).
Subgroup meta-analyses
Table 3 shows the associations between HT use and lung cancer risk in subgroup meta-analyses by methodological quality of study, type of HT, duration of HT use, status of HT use, smoking status, and histology of lung cancer.
OR, odds ratio; RR, relative risk; CI, confidence interval.
There was no significant association between HT use and lung cancer risk in subgroup meta-analyses by methodological quality of study, i.e., both in high-quality and low-quality studies (see Table 3).
A significant protective effect was observed among studies reporting the use of estrogen plus progesterone (OR 0.77; 95% CI 0.65-0.90), while there was no significant association between HT use and lung cancer risk among studies reporting the use of unspecified HT. There was a borderline significant protective effect among studies reporting the use of unopposed estrogen.
There was no association between HT use and lung cancer risk regardless of the duration of HT use, i.e., either short-term (< 5 years), mid-term (5–10 years), or long-term (> 10 years) (Table 3). Current users of HT had a decreased risk of lung cancer compared with never users (OR 0.76; 95% CI 0.76-0.93; n = 2), but this was not true for former users.
Significant protective effects of HT use on lung cancer were observed among former smokers (OR 0.74; 95% 0.59-0.93) and never smokers (OR 0.77; 95% CI 0.65-0.91), but not among current smokers. There was no association between HT use and lung cancer risk regardless of the histology of lung cancer, i.e., either adenocarcinoma, squamous cell carcinoma, or small cell carcinoma.
Discussion
In the current meta-analysis of epidemiological studies, including case-control and cohort studies, we found that the overall use of HT was not associated with the risk of lung cancer. However, when we conducted subgroup meta-analyses according to study design, a meta-analysis of case-control studies showed a significant preventive effect, while a meta-analysis of cohort studies showed no association. These inconsistent findings between two study designs are associated with the methodological quality of case-control studies. In the current study overall, case-control studies had a lower score (ranging 4 to 6) than cohort studies (ranging 6 to 8), in that they were deficient in the representativeness of cases, the selection of controls, and the nonresponse rate. Also, none of them reported whether they used the blind method to determine the status of case/control at the time of the interview.
We believe that the difference in the nonresponse rates between the case and control groups, which is a type of selection bias, was closely associated with a protective effect in meta-analyses of case-control studies. For example, regarding the nonresponse rate, a recent study reported that refusal to participate in case-control studies investigating the association between mobile phone use and brain tumor risk seems to be related to the less prevalent use of mobile phones, and this could result in a downward bias of approximately 10% in odds ratios for regular mobile phone use; 20 that is, we could assume that the relatively healthy HT users were more likely to participate in the study than nonusers, especially as controls, and therefore, a spurious negative (protective) association was observed. Likewise, representativeness of cases and selection of controls are considered to be related to the selection bias.
The use of combination estrogen plus progesterone showed a preventive effect on lung cancer risk, and no significant associations between HT use and lung cancer risk were observed in subgroup meta-analyses by duration of HT use and histology of lung cancer. However, these findings should be evaluated further, given the small number of studies.
Furthermore, we assume that there might be a link between the types of compounds used in HT having changed over time and lung cancer risk from the findings in the cumulative meta-analyses of case-control and cohort studies based on year of publication. Also, these findings might be associated with substantial heterogeneity observed in most of the subgroup meta-analyses. However, we could not confirm the relationship, because we were unable to identify exactly the types of HT compounds used in each study, because of lack of information.
In subgroup meta-analyses, significant protective effects of HT use on lung cancer were observed among former smokers and never smokers, but not among current smokers. It might be intuitively assumed that current smoking could attenuate a protective effect of HT on lung cancer risk; however, we were unable to confirm this because of insufficient data. Of all 11 studies included in the analysis, only 4 studies reported the association among current smokers and former smokers, and 6 studies reported it among never smokers.
To date, some biological evidence has suggested that there is a link between hormonal factors and lung cancer risk. Estrogen and other hormone receptors are expressed in both normal lung tissue and lung tumors. 13,14,21 Several studies have suggested that these hormone receptors play a role in non-small-cell lung cancer; estrogen and estrogen receptors regulate growth and differentiation of tumors through altering the transcription of estrogen-responsive genes in the nucleus and cytoplasm of lung epithelial cells. 22 –24 A recent immunohistochemistry study reported that progesterone inhibited proliferation in progesterone receptor–positive lung cancer cells, and progesterone receptor–positive status was associated with better outcome. 25 Based on these studies, several subsequent studies have suggested that progesterone therapy or estrogen receptor modulator may be clinically effective in some non-small cell lung cancer patients. 26,27 However, biological evidence for a link between hormonal factors and lung cancer risk is still limited.
Our meta-analysis has several limitations. First, this study does not provide a high level of evidence because we involved a small number of prospective cohort studies, given the paucity of published studies. Therefore, this topic should be further evaluated by using data from prospective cohort studies. Second, the exclusion of non-English language articles might bias our findings. A total of 37 non-English articles were searched during the selection process. However, when we reviewed them based on English abstracts, none of them met our main eligibility criteria. Third, we were unable to perform subgroup analyses by dosage of HT because most of the studies included in this analysis did not report the dosage of HT used. Fourth, even though we found no association between the duration of HT use and the risk of lung cancer, the data were suboptimal, because studies reporting those associations are lacking. Last, we should mention common limitations of meta-analyses: pooled results could incorporate the biases of individual studies and embody new sources of bias, mostly because of the selection studies and the inevitable heterogeneity among them. 28
Conclusions
Overall, we found that there was no association between overall use of HT and the risk of lung cancer in a meta-analysis of epidemiologic studies, including case-control and cohort studies. Although a subgroup meta-analysis of case-control studies showed a preventive effect of HT use on lung cancer, interpretation should be cautious because of the potential biases of low-quality case-control studies. Our findings require further research, such as more prospective cohort studies to provide a higher level of evidence.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.