
Abstract
Background and Aims:
Empowerment and opportunities to experience power and control in one's life contribute to health and wellness. Although studies have assessed specific factors related to women's empowerment and their influence on health outcomes, there is a dearth of published literature assessing the relationship of the empowerment of women with the overall health of a community. By means of this article, we aim to assess the relationship of women's empowerment with health in 75 countries.
Methods:
We used the gender empowerment measure (GEM), a composite index measuring gender inequality in economic participation and decision making, political participation and decision making, and power over economic resources. All 75 countries with GEM values in the 2006 Human Development Report (HDR) were included in the study. Association between the GEM values and seven health indicators was evaluated using descriptive statistics, scatter plots, and simple and multiple linear regression models. We also controlled for gross domestic product (GDP) as a possible confounding factor and included this variable in the multiple regression models.
Results:
When GDP was not considered, GEM had a statistically significant association with all health indicator variables except for proportion of 1-year-olds immunized against measles (correlation coefficient 0.063, p = 0.597). After adjusting for GDP, GEM was significantly associated with low birth weight, fertility rate, infant mortality, and age ≤5 mortality; the strongest correlation was found to be between GEM and infant mortality (R2 = 0.601).
Conclusions:
The results of this study suggest that the empowerment of women is associated with several key health indicators at a national level. Further research is necessary to determine the cause-effect relationship of these factors, confounding factors that may influence the relationship, and specific aspects of empowerment of women that effectively influence the health of the larger community.
Introduction
Research has demonstrated that health and well-being are intimately tied to and are consequences of power and powerlessness. Powerlessness or lack of control in one's life is a well-known risk factor for disease. Conversely, empowerment and opportunities to experience power and control in one's life contribute to health and wellness. 1 Empowerment is a process by which individuals, communities, and organizations gain control over issues that concern them most. 2,3 A more formal definition of the empowerment of women is that:
Empowerment is about people—both women and men—taking control over their lives: setting their own agendas, gaining skills, building self-confidence, solving problems, and developing self-reliance. It is not only a collective, social and political process, but an individual one as well—and it is not only a process but an outcome too. 4
In addition to its social impact, empowerment of women may influence health outcomes. Several studies have shown that women's empowerment and involvement can have significant positive effects on the health and quality of life of their family and community. 5 Women are most commonly the primary caregivers of the family and more often than men spend discretionary money on family and children. It has been proposed that the empowerment of women tends to reduce child neglect and mortality, decrease fertility and overcrowding, and broaden social concerns and cares. 6 Similarly, Kawachi et al. 7 concluded that indices of women's political participation and economic autonomy were strikingly related to overall female and male mortality rates in the United States. In a U.S. study by Koenen et al., 8 child well-being was worse in states where women have lower political, economic, and social status. Similarly, women's educational status and employment have been shown to be inversely related to child mortality and fertility. 9
Although studies have assessed specific factors related to women's empowerment and their influence on health outcomes, 10 there is a dearth of published literature assessing the relationship of the empowerment of women with the overall health of a community. By means of this article, we aim to assess the relationship of a gender empowerment measure with eight health indicators in 75 countries.
Our hypothesis was that the gender empowerment measure (GEM) would be positively correlated with male and female life expectancy and the proportion of 1-year-olds immunized against measles and that GEM would be inversely correlated with total fertility rate, infant mortality rate, under-5 mortality rate, and maternal mortality rate.
Materials and Methods
This retrospective study considered the data available in United Nation's Development Program's (UNDP) 2006 Human Development Report (HDR). 11 The HDR office relies on international data agencies with the resources and expertise to collect and compile international data on specific statistical indicators as noted on its website. 12 We used the GEM included in UNDP's HDR that has been used to measure women's empowerment. It is a composite index measuring gender inequality in three basic dimensions of empowerment: (1) economic participation and decision making, (2) political participation and decision making, and (3) power over economic resources. It measures political participation and decision-making power through calculation of women's and men's percentage shares of parliamentary seats; economic participation and decision-making power by measuring male and female percentage shares of positions as legislators, senior officials, and managers and women's and men's percentage shares of professional and technical positions; and power over economic resources by calculating women's and men's estimated earned income. 11 A higher value of the GEM signals a higher level of gender empowerment.
The UNDP reports had health indicators listed for 177 countries of which 75 had GEM values listed. 13 All 75 countries with GEM values in the 2006 HDR were included in the study. Health indicators considered included total fertility rate (births per woman), 1-year-olds fully immunized against measles (%), infants with low birth weight (%), infant mortality rate (per 1,000 live births), under-5 mortality rate (per 1,000 live births), maternal mortality ratio adjusted (per 100,000 live births), female life expectancy at birth (years), and male life expectancy at birth (years). In addition, we also considered the gross domestic product (GDP per capita in US$) data from the 2006 HDR for each of these 75 countries.
We investigated associations between the GEM values and the various health indicators using descriptive statistics, scatter plots, and simple and multiple linear regression models. We also controlled for GDP as a possible confounding factor and included this variable in the multiple regression models. We assessed normality of residuals and appropriateness of other regression assumptions using standard plots and tests of normality. 14 Where necessary, the health indicator variable was transformed to meet regression assumptions. A logarithmic transformation of low birth rate, fertility rate, and mortality rate was deemed appropriate. The plots for female and male life expectancy suggested that three outliers were present in each, and regression models were run with and without those outliers to check for their influence on the relationships.
Results
The mean GEM of all 75 countries in this study was 0.588 and varied from 0.128 in Yemen to 0.932 in Norway. The mean GDP was 1.387 and varied from 0.029 in Tanzania to 5.447 in Norway. A summary of the mean and range values of the eight health indicators for the countries in this study is provided in Table 1. Three countries (Botswana, Namibia, and Tanzania) were outliers in the health indicators of male and female expectancy.
Estonia, Finland, Iceland, Korea, Lithuania, Sweden.
Brazil, Equador, Hungary, Japan, Korea, Latvia, Panama, Ukraine.
A summary of the association of GEM with the eight health indicators considered in this study is as depicted in Figure 1. When GDP was not considered, GEM had a statistically significant association with all health indicator variables except for proportion of 1-year-olds immunized against measles (correlation coefficient 0.063, p = 0.597). GEM had a statistically significant positive association with female life expectancy and male life expectancy (Table 2). GEM had a statistically significant negative association in descending order with infant mortality, ≤5 mortality, maternal mortality, low birth weight, and fertility rate.
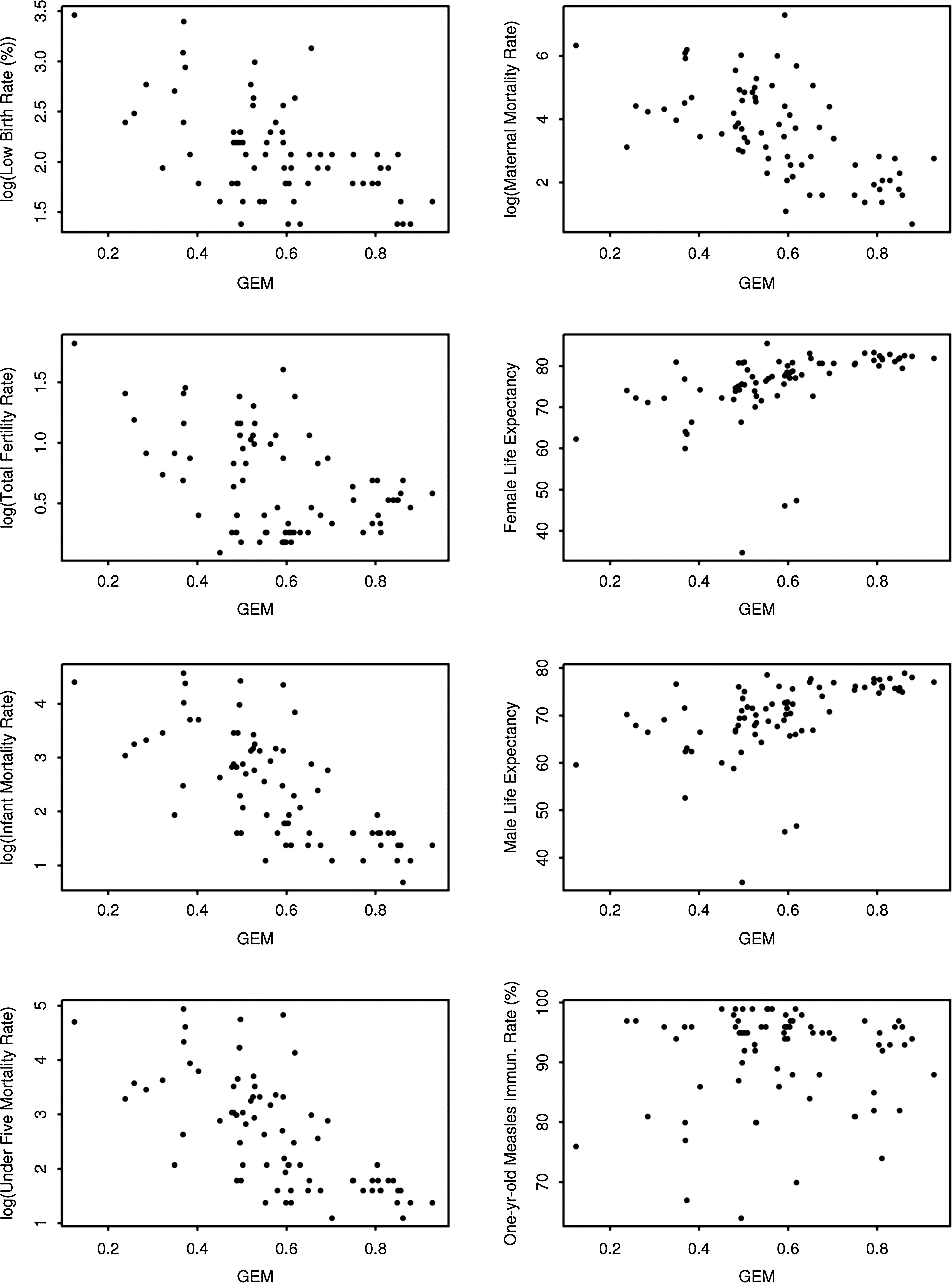
Association between GEM and health indicators for 75 countries. Some health indicators have been log transformed to meet regression assumptions.
This health indicator variable was log transformed to meet regression assumptions.
Three outliers (Botswana, Namibia, Tanzania) removed.
GDP was significantly associated with infant mortality, ≤5 mortality, maternal mortality, female life expectancy, and male life expectancy (Table 3). GDP and GEM were found to be highly correlated (Pearson correlation of 0.76). Neither variable was significantly associated with proportion of 1-year-olds immunized against measles. After adjusting for GDP, GEM was significantly associated with low birth weight, fertility rate, infant mortality, and ≤5 mortality (Table 3). The strongest correlation was found to be between GEM and infant mortality (R 2 = 0.601). GEM adjusted for GDP became a significant predictor of female life expectancy after excluding the three outliers and became a borderline significant predictor of male life expectancy. The R 2 values for the significant variables were moderate, indicating that GEM and GDP were important predictors but that they could only explain up to 60% of the variability in the health indicator variables.
GDP/10000.
This health indicator variable was log transformed to meet regression assumptions.
Three outliers (Botswana, Namibia, Tanzania) removed.
Discussion
Gender inequality harms women's health directly through sexual exploitation, domestic violence, genital mutilation, dowry deaths, sex-selective abortions, and forced marriages. 15,16 It also indirectly harms women's health through inequalities in education, healthcare, safety, employment, inheritance, leadership, mobility, sexual rights, and customs. It has been increasingly acknowledged that women's health and well-being are jeopardized by their unequal status in society, 7 whereas women's health and the health of their communities are enriched by the empowerment of women. 17 Our results suggest that in the 75 countries included in the study, the empowerment of women is associated with improvement in several health indicators.
GEM had a statistically significant association with seven of the eight health indictors we analyzed, including positive correlation with female life expectancy at birth and male life expectancy at birth and a negative correlation with infant mortality rate, total fertility rate, ≤5 mortality rate, maternal mortality rate, and low birth weight infant percentage. After adjusting for GDP, GEM continued to have a significant negative association with low birth weight, fertility rate, infant mortality, and ≤5 mortality and was correlated positively with male and female life expectancy. It is unclear why GEM did not correlate with the proportion of 1-year-olds immunized against measles; this result may have been different if all recommended immunizations were considered.
Although GDP and GEM were highly correlated, women's empowerment did not necessarily depend on national wealth, as some poor developing countries outpaced some rich industrialized ones. For example, Tanzania (GDP 288) has a higher GEM score (0.597) than Japan (GDP 36,182, GEM 0.557). The lack of relationship between empowerment and national wealth has also been suggested by other social scientists. 18
Akin to the results in our study, regional studies have shown that empowerment of women leads to decreased fertility rates and better child health in addition to increased contraceptive use and greater nutrient intake. 10 De Madres a Madres is an excellent example of community building through empowerment of women. This program attempted to overcome the low use of prenatal care by Latina women in Texas through trained volunteer mothers, who educated other women about prenatal care. No incidence of low birth weight babies occurred after the implementation of de Madres a Madres, and infant mortality declined from 16.5 per 1,000 live births in 1989 when the program was implemented to 11.4 in 1993. 19 The program also improved women's self-esteem, control, quality of life, and unity.
Economic participation, political participation, decision-making power, and power over economic resources are key components of GEM. When a woman is given agency or decision-making capacity, she is more likely to create change and mobilize toward greater equity. 20 Although Koenen et al. 8 did not use the GEM measure in their study, child well-being was worse in U.S. states where women have lower political, economic, and social status. Along similar lines, a study conducted in the countries of Bolivia, Cameroon, and Malaysia showed that when women have a greater say in spending priorities, they are more likely to spend on family and community resources for improving health, education, community infrastructure, and poverty eradication, as opposed to the military, alcohol, or gambling. 15
Education and training, media use and advocacy, public education and participation, organizing associations and unions, work training and microenterprise, enabling services and support, and rights protection and promotion are established methods to enhance the empowerment of women. 5 An extra year of female schooling increases wages by 10%–20% and has been suggested to reduce female fertility by 5%–10%. 21 Education also enables women's competitiveness, increases education of the next generation, improves health, and strengthens women's decision-making power, 22 especially in reproductive decisions. 23 It has been shown that women's secondary education is strongly associated with the greater use of healthcare, 24 less vulnerability to domestic violence, 25 and reduced infant and maternal mortality rates. 26 Although GEM does not directly consider the educational status of women, it likely indirectly measures it by considering economic participation and decision-making power as well as economic power over resources.
This study has limitations. Women's empowerment is a complex measure that spans many dimensions, including economic, sociocultural, familial/interpersonal, legal, political, and psychological dimensions. Although there is no doubt that the GEM has served as a priceless measuring tool of the status of women, it is difficult for anyone measure to fully capture these very broad dimensions in their various levels of social aggregation, and one must be careful of ecological fallacy, that is, the association observed at an aggregate level that does not necessarily represent an association that exists at an individual level. The variation in the nature and importance of empowerment across contexts poses a challenge in terms of both consistency and comparability in measurement schemes. This complexity is compounded by the lack of consistent and adequate data for most developing countries. 10 It is also important to note that the GEM is primarily interpreted as an index of gender equity in political and economic participation and decision making and does not capture the contributions of women in the vast unorganized informal sector, where the majority of the women are concentrated. 27
Although we controlled for the influence of GDP, there are likely several confounding factors that may have influenced the results of the study. Finally, when modeling female life expectancy and male life expectancy, we found three influential outlier countries, all of which were outliers in the health indicators of male and female life expectancy. Excluding those outliers changed the significance of correlations between GEM and life expectancy indicator values. Thus, the three outliers were influential, and, hence, results need to be interpreted with caution. Although we established an association between GEM and several health indicators, the study design limited us from determining a causal relationship between GEM and the health indicators.
The Beijing Declaration and Platform for Action suggested that the well-being of a society was dependent on the economic and political status of women within that society. 28 While addressing gender inequalities in the past 30 years, there has come about a progressive awareness of the need to empower women through measures to increase their social, economic, and political status within societies. Considered as a whole, a society that tolerates gender inequalities is also likely to be an unhealthier place to live, for both men and women, compared to a more egalitarian one. By identifying the effects of women's empowerment on the health of a community, we hope to provide the impetus for policymakers to strengthen their commitment to empowering women, thereby influencing the health of all people.
Conclusions
As the primary caregiver of the family, women play an important role in the health of the family. The results of this study suggest that the empowerment of women is associated with several key health indicators at a national level. Further research is necessary to determine the cause-effect relationship of these factors, confounding factors that may influence the relationship, and specific aspects of empowerment of women that effectively influence the health of the larger community.
Footnotes
Acknowledgment
We would like to acknowledge the efforts of Aarti Jerath who contributed to the literature search for previous versions of this article.
Disclosure Statement
The authors have no conflicts of interest to report.