
Abstract
Background:
Ovarian cancer usually spreads intra-abdominally. Supradiaphragmatic metastases are rare, and axillary lymph node metastases are exceptional. Here, we present the first case of ovarian carcinoma detected at screening mammogram as intramammary lymph node metastases.
Case report:
A 44-year-old obese woman underwent core biopsy of a suspicious mammographic finding histologically consistent with lymph node metastases from breast cancer. Serum tumor markers, including CA 125, were normal, and clinical staging was negative. The patient underwent quadrantectomy and axillary dissection that revealed four involved lymph nodes but no primary breast carcinoma. Accurate re-evaluation of the histological specimens suggested the possible ovarian origin of the tumor. An [18F]-fluorodeoxyglucose (FDG) positron emission tomography/computed tomography revealed a 33-mm solid mass with intense metabolic FDG uptake in the right groin and a small simple ovarian cyst with normal FDG uptake. The ovarian cyst was removed laparotomically and was malignant on frozen section. Surgical staging revealed a well-differentiated serous ovarian carcinoma microscopically involving the omentum and massively infiltrating the groin node. After chemotherapy, the patient developed metastases in the contralateral axilla that was removed surgically. The patient is alive with no evidence of disease 20 months after surgical removal of the primary tumor.
Conclusions:
Surgeons should be aware that ovarian cancer may rarely metastasize to intramammary and axillary nodes, mimicking a primary breast carcinoma.
Introduction
Ovarian cancer is the sixth most frequent female malignancy, but it represents the most common cause of death from gynecological tumors. This disease develops most frequently in postmenopausal women, and >70% are initially diagnosed with International Federation of Gynecology and Obstetrics advanced stages (III or IV). Metastases occur by peritoneal fluid's tracking via hematic and lymphatic systems, mainly to intraperitoneal organs. Supradiaphragmatic metastases, including those to the breast, are rare, and axillary lymph node involvement is exceptional. To clarify the issue of breast and axillary lymph node metastases from primary ovarian cancer, we searched the English language literature on PUBMED (
Case Report
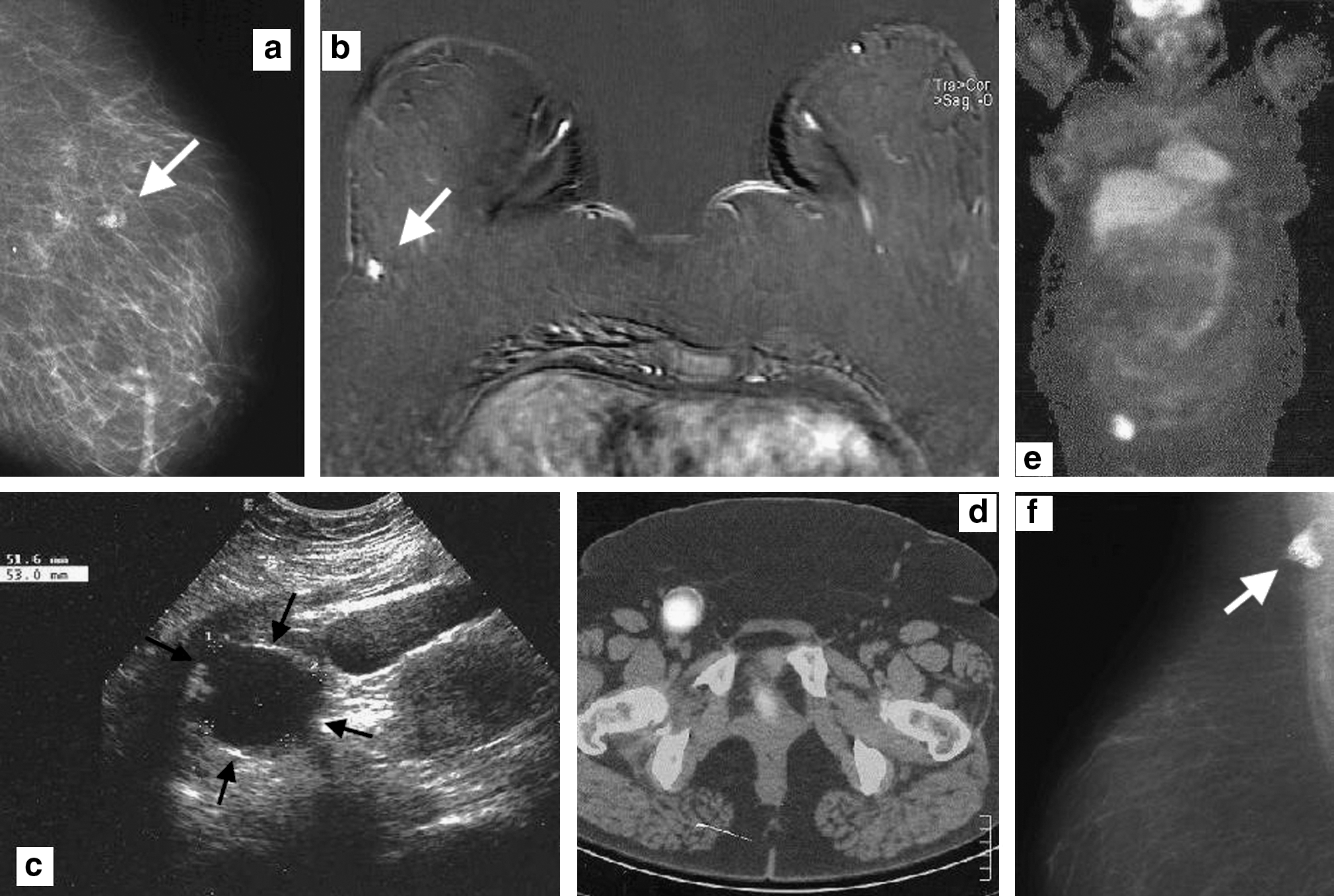
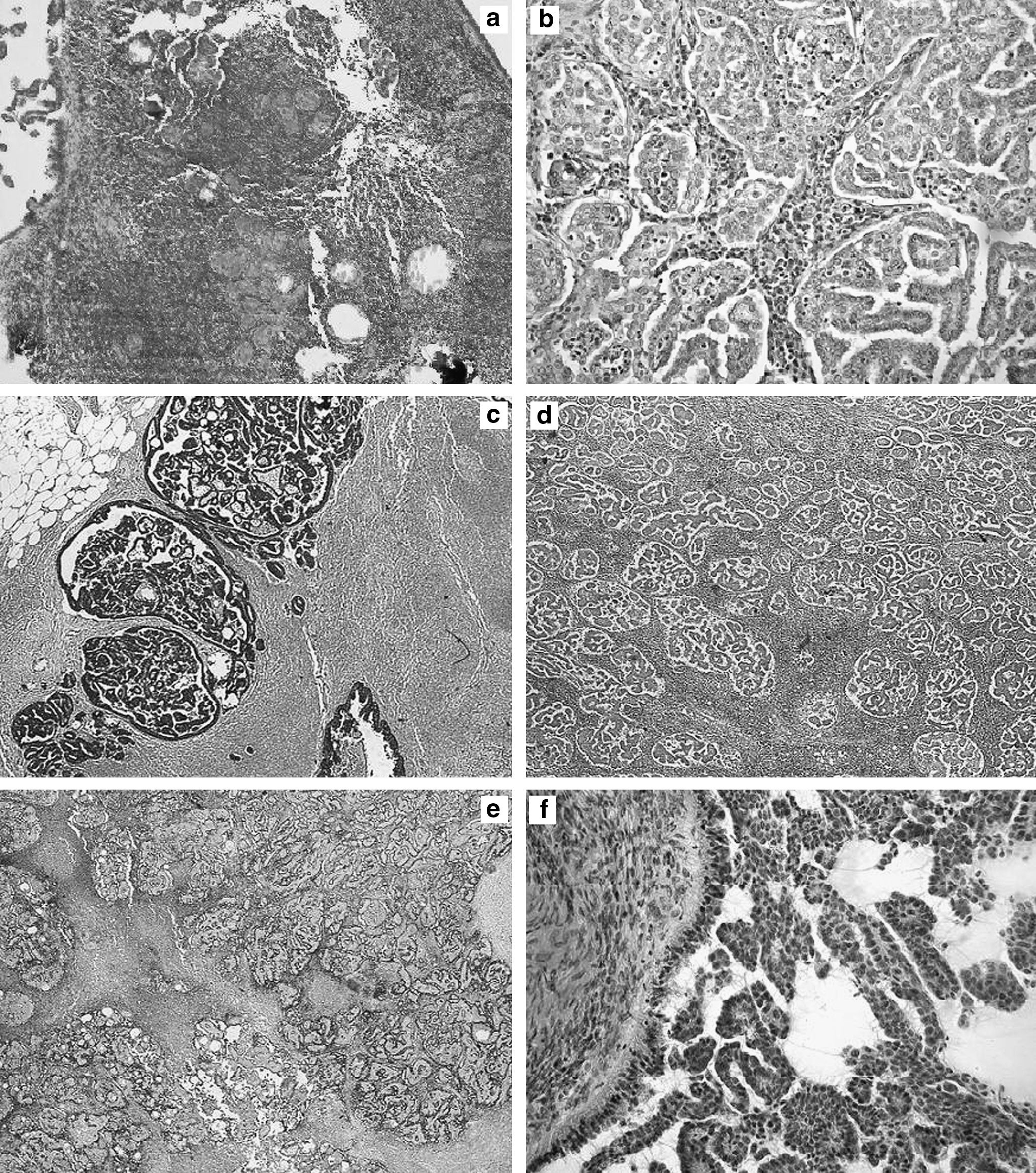
A 44-year-old woman, gravida 2, para 2, with severe obesity (body mass index [BMI] = 37 kg/m2) and no history of previous illness, endocrine dysfunction, or neoplastic diseases, presented a 6-mm solid radiopaque nodule with irregular microcalcifications in the external-central quadrant of the right breast at screening mammogram (Fig. 1a). This finding was considered highly suggestive of a primary breast cancer by the breast radiologist. The core biopsy showed metastatic invasion of a lymph node, histologically consistent with breast cancer metastasis (Fig. 2a). The patient underwent a bone scintigraphy that was negative. Breast magnetic resonance imaging (MRI) confirmed the presence of a focal enhancement in the external-central quadrant of the right breast, corresponding to the metastatic intramammary lymph node, but failed to identify the primary tumor in both breasts (Fig.1b). An abdominal ultrasound scan (US) revealed no liver metastasis and, in the pelvis, a 5-cm unilocular right ovarian cyst (Fig. 1c). Serum tumor markers were all negative. As it was necessary to remove the positive intramammary lymph node located within the parenchyma of the external-central quadrant of the right breast, we decided to perform a quadrantectomy. Because of the absence of suspicious findings in both mammogram and MRI other than the radiopaque nodule already biopsied, the nodule was initially interpreted as the primary tumor in close proximity to the lymph node. The surgical procedure was completed with total axillary dissection because of positive sentinel node biopsy on frozen section.
(
(
The definitive histology of the intramammary lymph node and of four axillary lymph nodes showed infiltration from a papillary-pattern carcinomatous proliferation with microcalcifications, without evidence of primary breast carcinoma. The morphological and immunohistochemical profile (cytoberatin [CK7+], (Wilm's tumor) WT1+, CA 125±) suggested the possible ovarian origin of the lesion (Fig. 2b, c, d). This immunohistochemical profile, although typical of ovarian cancer, can also be found in breast cancer. However, the lack of any primary breast carcinoma in the surgical specimen as well as in the breast MRI prompted us to further investigate the ovaries. Estrogen and progesterone receptor immunostaining was not performed.
After 2 weeks the patient underwent an [ 18 F]-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) that revealed a 33-mm solid mass with intense metabolic FDG uptake in the right groin (Fig. 1d, e). Moreover, the PET/CT showed a 46-mm right ovarian cyst and a left axillary nodule, both with normal FDG activity. The patient underwent laparotomy. The right ovary was cystic but macroscopically benign, capsulated, and without surface vegetations, adhesions, or ascitic fluid. Careful inspection and palpation of intraperitoneal and retroperitoneal organs did not reveal suspicious findings. The right adnexus was removed and sent for a frozen section that was suspicious but inconclusive. A total hysterectomy, left salpingo-oophorectomy, omentectomy, appendectomy, multiple peritoneal biopsies, and removal of the groin mass through a separate inguinal incision were performed. Histological diagnosis showed well-differentiated serous ovarian carcinoma (Fig. 2f) diffused to the omentum and massively infiltrating the inguinal lymph node (Fig. 2d, e). The uterus, left ovary, and appendix were uninvolved. The patient underwent standard chemotherapy (carboplatin AUC 7.5 and paclitaxel 175 mg/m2 for six courses).
Eight months after chemotherapy, a follow-up CT scan revealed the presence of a 18-mm solid mass in the left axilla. The patient underwent a mammogram (Fig. 1f) and US scan that confirmed the presence of a lymph node with microcalcifications in the left axilla, which was then sampled by core biopsy with diagnosis of serous ovarian carcinoma metastasis. A new PET/CT was negative, confirming the presence of the left axillary node with normal FDG uptake. Then, 1 year after the abdominal operation, the patient experienced symptoms caused by a large median laparocele. She underwent repair with prosthetic material and a second-look procedure with multiple peritoneal biopsies, with no evidence of intraperitoneal disease. Concomitantly, the left axillary node was removed, with histological confirmation of lymph node metastasis from ovarian carcinoma. The patient is alive with no evidence of disease 20 months after surgical removal of the primary tumor.
Discussion
This is the first reported case of ovarian carcinoma with intramammary lymph node metastases, bilateral axillary metastases, and occult groin involvement. We found this case intriguing because the initial diagnosis from screening mammogram was highly suggestive of a primary breast carcinoma. The first core biopsy showed the presence of an intramammary metastatic lymph node, histologically consistent with breast carcinoma metastases. Therefore, it was interpreted as a primary breast carcinoma in close proximity to the lymph node; for this reason, we elected to perform a quadrantectomy. In view of the possibility of occult breast carcinoma, axillary lymphadenectomy and chemotherapy could have been considered. However, the need to remove the positive intramammary lymph node obliged us to resect the breast quadrant harboring the metastatic lesion. In addition, it was necessary to delay chemotherapy until a clear and definitive diagnosis was obtained. Hockstein et al. 26 reported a case of ovarian adenocarcinoma with axillary lymph node metastases initially treated with tamoxifen, wrongly assumed to be a primary breast tumor. The authors concluded that when a patient has metastatic disease, it is critical to determine the origin of the malignancy, especially given that adjuvant therapies differ.
In the present case, the small ovarian cyst was disregarded initially because of its benign appearance and the normal CA 125 levels. After the breast excision, the lack of a primary breast carcinoma in the surgical specimen along with the presence of multiple positive axillary lymph nodes led to further histopathological evaluation, including an immunohistochemical profile that suggested the possible ovarian origin of the tumor (Fig. 2b, c). In addition, the PET/CT scan performed after the breast operation failed to show pathological FDG uptake in the ovary, supporting the interpretation of the small ovarian cyst as benign. Nonetheless, the PET/CT scan was useful because it revealed a groin mass with intense FDG uptake that was not palpable because of the patient's obesity (Fig. 1d, e). The left axillary lymph node was also seen on the PET/CT, albeit with normal FDG activity, but it was not given consideration until a mammogram suggested the possibility of a metastatic node.
We believe this case is noteworthy because we have not found a similar case previously described in the literature. Most of the reported cases deal with breast or axillary metastases developing during follow-up of a previously treated ovarian cancer. Only one case has been published in which axillary metastasis from ovarian cancer was detected before the primary tumor. 26 In that case, however, the metastatic lymph node was axillary rather than intramammary, and a staging CT scan easily found a large ovarian mass, leading to preoperative diagnosis. In the present case, in contrast, the ovary was slightly enlarged, with a simple, benign-looking cyst (Fig. 1c) and normal CA 125 serum levels. Another interesting and unusual feature of the current case was the massive involvement of an ipsilateral groin node. The 3.5-cm solid inguinal mass represented the largest single tumor deposit, even greater than the primary tumor. The presence of groin metastases from serous ovarian cancer have been reported in a few cases previously. 33 –37 The PET/CT scan, although useful in detection of the groin mass, failed to identify the primary tumor in our case. This is in contrast with the findings of Manci et al., 35 who reported the usefulness of PET/CT in detecting the ovarian origin of a tumor while staging a patient with bilateral groin metastases of unknown origin. The present case points out the strong lymphotrophic behavior that ovarian cancer may sometimes display, with involvement of several distant lymph nodes, in spite of the limited ovarian proliferation and the well-differentiated histological pattern. Extra-abdominal lymph node metastases from ovarian cancer are rare, but they can occur given the anatomy of the pelvic lymphatic system. The presence of lymphatic drainage from the ovary that reaches the inguinal canal through the round ligament allows us to understand how groin metastases are possible. Concerning axillary lymph node involvement, the development of ovarian metastases is more difficult to explain; a possible explanation could be the ability of serous ovarian carcinoma metastases to skip pelvic and aortic lymph nodes, reaching the central lymphatic duct and subsequently supradiaphragmatic lymph nodes. 38
Another interesting finding of the current case was the mammographic appearance of the metastatic intramammary and axillary lymph nodes, with several microcalcifications (Fig. 1a, f ). Singer et al. 28 reported a similar mammographic pattern with microcalcifications in a case of ovarian cancer with metastases to the axillary lymph nodes. Patel et al. 39 suggested that the calcifications may be the radiological correlate of psammoma bodies, which are a typical pathological feature of serous ovarian carcinoma. Indeed, psammoma bodies were detected at histological examination of metastatic axillary lymph nodes in the present case as well. Therefore, the finding of axillary lymph nodes with microcalcifications should prompt careful evaluation of the ovaries to rule out the possible presence of a primary ovarian malignancy. There is no question that establishing the right diagnosis from the beginning is beneficial for the patient, avoiding unnecessary surgical and radiation treatments and defining optimal adjuvant chemotherapy. In our case, the minimal tumor burden in the ovary, along with normal serum CA 125 levels and patient obesity, prevented early clinical diagnosis of the groin mass.
Although Hockstein et al. 26 reported a case with ovarian cancer with axillary lymph node metastases, this is the first case in which screening mammogram detected an intramammary abnormal finding that ultimately yielded a metastatic intramammary lymph node from a previously unknown primary ovarian cancer. In addition, this is the first case in which breast and axillary metastases from ovarian cancer were found concomitantly with groin metastases.
In conclusion, general surgeons and gynecological oncologists should be aware of the possibility that primary ovarian cancer may occasionally occur with multiple extrapelvic lymph node metastases, sometimes mimicking a primary breast carcinoma. The presence of metastatic axillary lymph nodes with microcalcifications should remind clinicians to evaluate the ovaries.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.