
Abstract
Aims:
Improper and inconsistent contraceptive use contributes to the unintended pregnancy rate. The intrauterine device (IUD) is an effective, safe method of contraception that cannot be used improperly or inconsistently. However, it is relatively underused in the United States. We developed a qualitative study to better understand patient beliefs and attitudes that may act as a barrier to acceptance or use of an IUD.
Methods:
We conducted semistructured interviews with a convenience sample of 40 reproductive aged women from two Bronx, New York, family medicine practices. Self-report of having heard of the IUD was the main eligibility criterion. We used an iterative process of data collection and analysis.
Results:
Although respondents appreciate the advantages of an IUD, they express a number of conceptual concerns and fears about the device. These are primarily related to voluntarily placing a device inside the body for a prolonged period of time and to a knowledge gap about internal female reproductive anatomy. The IUD is viewed as a contraception option to use when other methods have failed or after childbearing. Additionally, respondents report a lack of discussion and information about the IUD from healthcare providers, the media, and informal networks.
Conclusions:
Directly addressing patient reservations that might otherwise be left unsaid could potentially increase acceptance of the IUD. The issues elucidated in this study begin to shed light on specific patient concerns that providers or public health messages may address during IUD contraception counseling. Given the high efficacy and safety of IUDs, increasing use could impact rates of unplanned pregnancy.
Introduction
Despite the fact that contraceptive use in the United States is relatively high 1,2 and that most contraceptive methods are nearly 100% effective when used perfectly, 3,4 unintended pregnancy rates remain high and have been relatively unchanged in the past decade. 5 Improper and inconsistent use of contraceptives contributes to the rate of unintended pregnancy. 6,7 Over 50% of women receiving abortion services in the United States report using contraception at the time of their unintended pregnancy. 8
A number of factors influence contraceptive use and, thus, by extension, unintended pregnancy rates. These factors include the effectiveness of the contraceptive method when used as directed (perfect use), the user's ability to employ the method consistently and correctly (typical use), and the continued use of the method. With perfect use, hormonal contraceptives are nearly 100% effective, yet with 1 year of typical use, oral contraceptive pills' failure rates are approximately 8%, 9 and only 68% of users continue to use the method after 1 year. 3 In contrast, an intrauterine device (IUD) is almost 100% effective with both perfect and typical use; 78–81% of women continue to use the method after 1 year. 3
IUDs are the most effective long-term reversible method of contraception 4,10 and one of the most popular reversible contraceptive method worldwide, 11 yet they are used by few women in the United States. Before the morbidity and resulting litigation around the faulty Dalkon Shield IUD in the 1970s and 1980s, approximately 10% of U.S. women using contraception used an IUD. 12 Currently only 2% of U.S. women using contraception use an IUD. 1,13 Two types of IUDs are available in the United States today: the Copper T 380A (Duramed Pharmaceuticals Inc, Cincinnati, OH, marketed as as ParaGard®), and the levonorgestrel-releasing intrauterine system (LNG-IUS, Bayer HealthCare Pharmaceuticals, Morristown, NJ, marketed as Mirena®).
The reason for the low rate of IUD use in the United States is multifactorial, with healthcare provider, 14,15 health system, 16,17 and patient issues impacting IUD use. In this study, we explore women's conceptions and beliefs about the IUD that may act as a barrier to use. Whereas prior studies of U.S. women have examined acceptability of 18,19 and knowledge about 20,21 the IUD, we theorized that myths and misconceptions—distinct from acceptability and knowledge—act as deterrents to use. Specifically, we asked reproductive aged female patients in two urban family medicine clinics their (1) experience with and attitude toward IUDs and (2) opinions about why few women in the United States use IUDs. Our intent in conducting this study was to elucidate patient concerns (that may otherwise be left unsaid) that providers could include in patient-centered IUD counseling.
Materials and Methods
A female research assistant (I.W.) conducted semistructured interviews at two family medicine clinics affiliated with an academic medical center in the Bronx, New York. Family physicians at both clinics insert IUDs. We chose to conduct the study at these clinics because they serve a predominantly minority, low-income population; women with these demographic factors experience higher than average rates of unintended pregnancy. 6,22 Although multiple issues contribute to this disparity, developing patient-centered IUD counseling could affect IUD use and help more women attain their desired reproductive goals.
I.W. interviewed a convenience sample of female patients aged 18–45 years who were approached while waiting to access clinical services. The interviewer explained that she was “talking with some female patients about what they have heard and know about a method of birth control called an IUD or intrauterine device.” In addition to the age and gender requirements, inclusion criteria included having heard of the IUD, being a clinic patient, and having the ability to understand and communicate in English. If the woman expressed interest in the project and was eligible, she was taken to a private location within the clinic where oral consent was obtained and the interview was conducted. The interviews lasted approximatly10 minutes and were digitally recorded and later transcribed.
Based on our literature review and research question, a semistructured interview guide was developed, piloted with female patients at one family medicine clinic, and modified accordingly. In addition to providing demographic information, respondents were asked about their experience with the IUD, their knowledge of the “word on the street” concerning IUDs, why they think it is underused, and their opinion of why a woman would or would not choose to use an IUD. We collected patient demographic characteristics that had previously been found to be associated with IUD use. 23
We used an iterative process of data collection and analysis. 24 Throughout the data collection, we read and coded transcripts to identify themes and appropriately refined the interview guide. Once data collection was completed, we finalized emerging codes, independently reread the transcripts to apply the new codes, and then met to compare coding of the final version. Differences in coding were minimal and were resolved by discussion. Transcripts were coded and entered into NVivo (QSR International Pty Ltd., Melbourne, Australia version 8, 2008) to assist with analysis. 25 No a priori codes were used.
Initially we had hoped to understand myths, urban legends, and misconceptions about the IUD. After the first eight transcripts were reviewed, it became apparent that not many IUD myths existed in our population. Thus, the questions were modified to elicit common perceptions and thoughts about the IUD and respondent's beliefs on why a woman may or may not want to use an IUD.
This study was granted exempt status from the institutional committee on the protection of human subjects at the Albert Einstein College of Medicine.
Results
During July 2008, we interviewed a total of 40 women from two different family medicine clinics. Seventy-three percent of eligible women approached agreed to participate. Figure 1 depicts participant recruitment, and Table 1 shows some demographic characteristics of the women interviewed and their experience with the IUD. Only 6 (15%) had personal experience with the IUD. In contrast, 32 (80%) knew someone who had used an IUD; of those 32 respondents, 21 described either positive or mixed experiences.
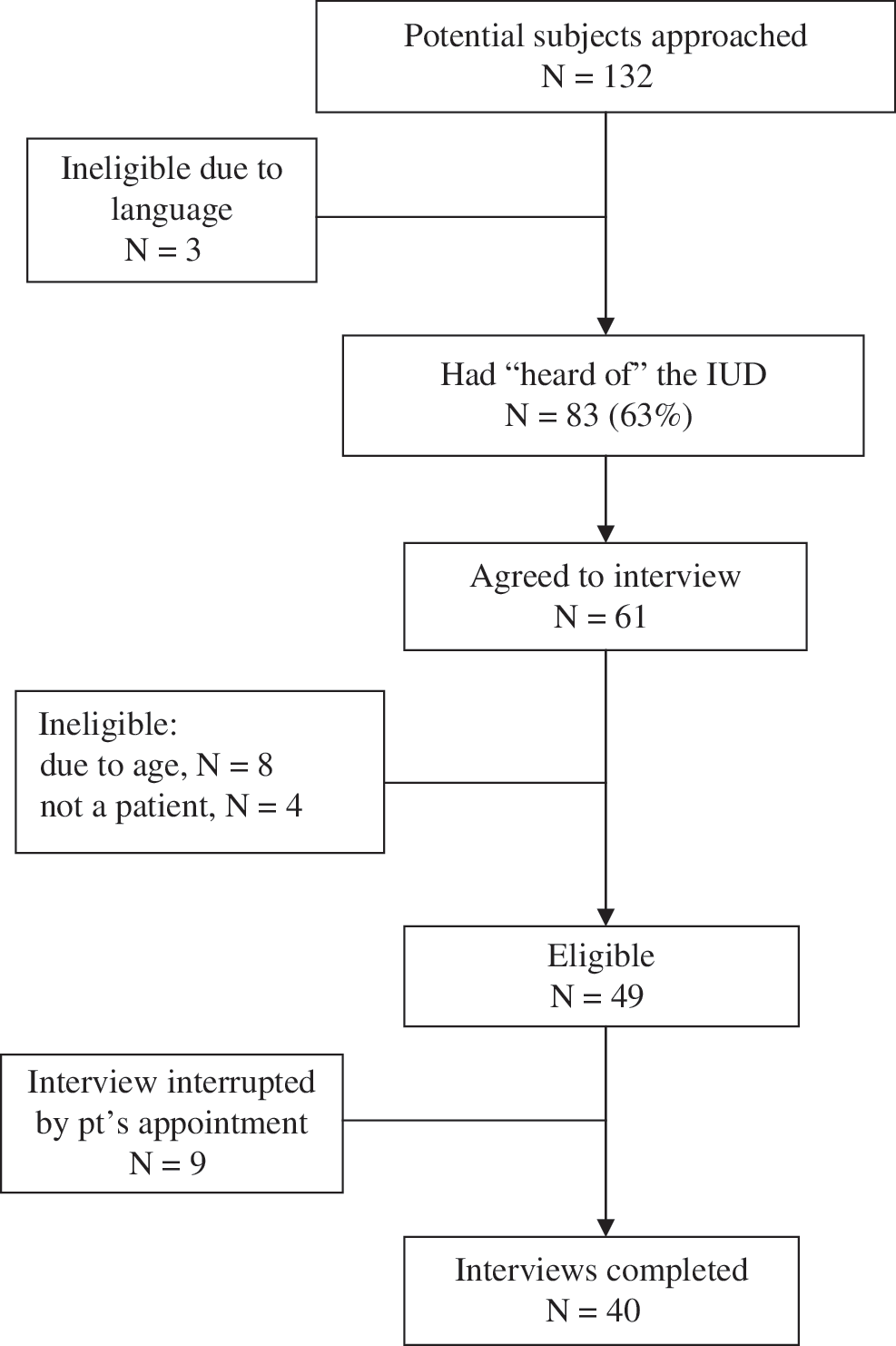
Participant recruitment.
Women are clear, though limited, in their knowledge about the advantages of an IUD (Table 2). Concrete concerns about potential side effects or disadvantages are described in Table 3. What we describe reflects their major conceptual device-related concerns and themes. Representative quotations are included to illustrate these concerns.
Device-related concerns
Intrauterine placement
The most frequently cited theme that emerged are negative feelings, concerns, or discomfort with a device inside the body. Respondents often refer to this as “up in me” (n = 22). A number of our respondents are unsettled by the idea of a healthy woman voluntarily placing a device inside her body. It's something that is placed inside for a long time. It's not like you are doing it because you are sick. It's something that you choose to do. (27-year-old African American mother of one, Respondent 1) For me it was the whole idea of having to have it placed within me, you know, I didn't really want that. (25-year-old African American woman, Respondent 40)
Some respondents (n = 6) articulate concern about the insertion, which is viewed by many as a surgery. With the IUD they have to go inside you, so that's what I think they are scared of … When they first tell you about the IUD, how they say there putting it in there. … they are probably scared because maybe it's like a surgical procedure. (24-year-old Latina mother of three, Respondent 6)
For others, this relates to the lack of personal control (n = 6) that comes with dependence on a healthcare provider to insert and remove the device. These two respondents describe the importance of control over starting and, especially, stopping their contraceptive method. … that you have to put a contraption in your body and you can't get it out and something goes wrong, or it doesn't act right, then what? You are standing there panicking. … You have to wait for them to take it out. You could not just take it out. I would have been screaming. (33-year-old African American mother, Respondent 13) I used to take the pill, and if something goes wrong, I know that I don't have to take the pill any more. I can stop taking it. IUD, I have to get someone to go in there and take it out. … I don't want to have this thing in me and have this feeling that I just can't stop, that I have to wait. (32-year-old Latina mother, Respondent 8)
Although many cite long-term pregnancy protection as an advantage of the IUD (Table 2), others voice concern about the long-term effects of having an object inside their body (n = 12). Similar to this respondent, they worry: It's like 5 years, or 10 years. For me that is a long time for something to be inside you. (36-year-old African American mother of three, Respondent 17)
For another woman, both the time frame and internal placement of the IUD are seen in a negative light in comparison to other contraceptive methods.
Is it going to hurt me … sitting inside of me, is [the IUD] going to go bad? You think about things like that because it is something inserted inside of you. As for the patch, it is right here on your skin, the depo is inserted, it's like a shot, and the pill you take it and it dissolves. You do not think oh, they are sitting there for 5 years. (22-year-old African American woman in her first pregnancy, Respondent 23)
Doubts about placement and how the IUD works
Many women express a knowledge gap or misunderstanding about internal female reproductive anatomy. The hidden nature of the device coupled with this poor anatomical understanding lead women to question if and how the IUD could be an effective form of pregnancy prevention. They question where the device is placed and how it could remain in place (n = 11). As this respondent asks: On TV it looked a little comfortable, it wasn't so big. I was, oh ok, now where is that going and how does it stay in place? (25-year-old Latina mother of one, Respondent 4)
This woman's lack of knowledge of where the IUD is placed as well as concerns about the IUD's mechanism of action lead her to question its efficacy. If it's easy to put up there, it's easy to take out … then when you are intimate with someone, it needs to be removed, because what is it holding on to? … . Will it really work, because its' like a little T?. … . Maybe [women] don't want to put that, a piece of T up in them, thinking … it has metal on it, does it really kill the sperm, what does it do? (36-year-old African American mother of three, Respondent 17)
Although most respondents generally feel confident about the IUD's effectiveness, the relative invisibility of the device (compared with other contraceptive methods) leads to concern about the inability to ensure the IUD remains in place; thus, women might unwittingly place themselves at risk of pregnancy. They often described this as an undetected “slippage” (n = 16). As this woman describes: Just for the fact that it's up there, you don't know what's happening, you don't know exactly if it falls out, what could happen if it falls out and you don't know … That's the major thing, how do you know it's still there? (20 years old, Respondent 30)
Additionally, a number of women are not concerned about expelling the IUD per se, but they express fear about the consequence of the device moving around inside their bodies. … you know everyday [the IUD is] there, you are careful to what you are doing, when you are doing it, how you are doing it, and all that, so it doesn't shift from this place to the next place or move around. (Respondent 25)
Reasons for underuse
Lack of discussion and lack of information
Women's limited baseline knowledge precluded them from giving detailed information on underuse. However, when questioned directly about their conversations with friends, family, and medical professionals about the IUD and their thoughts of why the IUD is underused in the United States, respondents cite a general lack of information (n = 28) from both informal and formal sources, as well as lack of discussion (n = 22) about the device.
Respondents do not talk with their friends about the IUD in the same way they discuss other contraception. When asked by the interviewer what friend and colleagues are discussing about the IUD, these respondents reply: People hardly talk about it. People talk more about the birth control [pill]. (25-year-old Hispanic mother of three, Respondent 19) I don't really hear about it. It's mainly the other things that are out now. (28-year-old African American mother of one, Respondent 22)
If it had been discussed with their healthcare provider, respondents say their provider generally presented the IUD as an option to be used after pregnancy or childbearing or when unable to use other methods. IUDs are viewed as somehow outside the usual, common methods for pregnancy prevention.
When you come to the doctor, they don't say IUD first, they say pills and shot, that's like the first row, then they throw in the patch. They don't mention the IUD, you have to basically somewhat ask about it and you may come across one doctor that will be like “Oh—you haven't tried this?” And that's probably because you have been through everything else. (23-year-old pregnant woman, Respondent 23)
Women also note that there is not much advertising or media attention about the IUD, especially as compared with other methods of contraception.
I don't think it's been advertised enough to be out in the community. … If it's not advertised, you are not aware of it. How can you ask for something you are not aware of? (30-year-old mother of two, Respondent 11)
Discussion and Conclusions
The IUD is an effective contraceptive method, yet it remains underused in the United States. In this study, we found that, overall, women have many concerns related to qualities of the device itself and report that they do not know as much about the IUD as they do about other methods of pregnancy prevention. An IUD is viewed as a convenient and reliable method of pregnancy prevention, but it is full of unknowns. From the perspective of our respondents, the biggest barrier to use appears to be that the device itself is intrauterine. There are few other medical devices or medication delivery systems that an otherwise healthy person chooses to have placed inside the body. If IUD use is to increase in the United States, this concern may need to be addressed directly during contraception options counseling.
Although concerns appear primarily to be related to the uniqueness of the intrauterine placement itself, it is compounded by a lack of knowledge of the internal female reproductive anatomy; an issue not unique to this group of women. 26 –28 Better education about female reproductive anatomy and fertility might help to address some of these concerns. As noted in the Introduction, only 2% of U.S. women using contraception use an IUD, 1 yet 18% of U.S. female obstetricians/gynecologists use an IUD. 29 This may indicate that U.S. women who are informed about the method and who have an understanding of many of the areas of concern for our respondents, including internal female reproductive anatomy, could be much more accepting of an IUD.
Our findings of women's concerns about the IUD echo findings in international settings. Researchers in an English general practice in 2005 also found that women lacked information about the IUD and were concerned about the lack of personal control. 18 In contrast to the English respondents, our respondents appear to have a better understanding of the potential side effects and less concern about insertion and infection; we are surprised that our respondents infrequently mentioned concern about infection risk. Similar to our findings, an Iraqi study also found that many women had fears about the device migrating. 30
These results point to a need to increase IUD visibility and discussion within the medical encounter, as well as increased public health and public service messaging. This approach has shown to be effective in other countries. Mexican women's IUD use rates significantly increased primarily as a result of IUD counseling during prenatal care as well as a policy approach to reduce systems barriers. 10 Both studies of providers 31 and practice guidelines 32 emphasize the importance of contraceptive counseling. The IUD should be included in contraceptive counseling as a first-line method for most women. The Copper T 380A is FDA approved for nulliparous and adolescent women. 33 Many women with heavy vaginal bleeding experience relief with the hormonal IUD. 34,35 IUDs can be used safely in women with a history of ectopic pregnancy, pelvic inflammatory disease (PID), or sexually transmitted infection (STI). 17,21 As there is a transient increased risk of PID during the first few weeks after insertion, 36 which appears to be associated with the insertion process, 37 the recommendation is to wait 3 months after treatment of an STI or PID before inserting an IUD. 38,39 Additionally, clinicians must counsel women that IUDs do not protect against STIs.
The study limitations include our use of a convenience sample. The results, therefore, are not generalizable. However, the findings, as described, are consistent with research done in other settings. Another limitation is our recruitment from a clinic patient population. Although we did not ask explicitly, we assume that the vast majority of our respondents have health insurance. Thus, access to providers for insertion/removal and the cost of the device were not mentioned as concerns for our sample, although it likely contributes as a patient factor limiting IUD use.
Although few U.S. women choose an IUD, those who do tend to have much higher continuation rates 4 and method satisfaction compared with other contraceptive methods. 19 Given the high efficacy and safety of IUDs, increasing use could impact rates of unplanned pregnancy, but in order to increase the use of IUDs, providers must address patient concerns. The apprehensions elucidated in this study begin to shed light on specific concerns providers may want to discuss with their patients during IUD contraception counseling. Future research evaluating counseling interventions would be helpful.
Footnotes
Acknowledgments
We would like to acknowledge M. Diane McKee for her input on the study analysis and manuscript review.
Disclosure Statement
The authors have no conflicts of interest to report.