
Abstract
Background:
Since 1999, the Centers for Disease Control and Prevention's (CDC) Arthritis Program has worked to improve the quality of life for people with arthritis, in part by funding state health departments to disseminate physical activity (PA) and self-management education (SME) interventions. Initially, only one SME and two PA interventions were considered evidence-based and appropriate for people with arthritis. The purposes of this article are to describe the processes and criteria used to screen new or existing intervention programs and report the results of that screening, including an updated list of recommended intervention programs.
Methods:
A series of three sets of screening criteria was created in consultation with subject matter experts: arthritis appropriateness, adequacy of the evidence base, and implementability as a public health intervention. Screening interventions were categorized as Recommended, Promising Practices, Watch List, Future Possibility, or Unlikely to Meet criteria based on how well the intervention met the screening criteria.
Results:
A total of 15 packaged PA interventions and six SME interventions were screened. Three PA and three SME interventions met all three sets of criteria and were added to the list of recommended public health interventions for use by CDC-funded state arthritis programs. An additional two SME interventions are developing the infrastructure for public health dissemination and were categorized as Promising Practices, and six PA interventions have evaluations underway and are on the Watch List.
Conclusions:
The CDC Arthritis Program identified arthritis-appropriate interventions that can be used effectively and efficiently in public health settings to improve the quality of life of people with arthritis. The screening criteria used offer a guide to intervention developers on necessary characteristics of interventions for use in public health settings. The expanded menu of interventions is beneficial to clinical care and public health professionals and, ultimately, to people with arthritis.
Introduction
Arthritis is a significant public health issue based on prevalence and impact, and both are projected to increase substantially in the coming decades. Based on 2003–2005 data, 46.4 million (21.4%) noninstitutionalized adults over age 18 reported a doctor's diagnosis of arthritis, 1 and prevalence is projected to increase to 67 million (25%) by 2030. 2 Arthritis is the most common cause of disability 3 ; 41% of adults with arthritis report arthritis-associated activity limitations, 1 and 31% of working-age adults report arthritis-associated work limitations. 4 The number of people with activity limitation due to arthritis is projected to increase to 25 million by 2030. 2
Arthritis also disproportionally affects women, in both prevalence and impact. Sixty-one percent (28 million) of the 46 million Americans with arthritis are women. 5 Women with arthritis also report greater prevalence of arthritis-attributable activity limitation (42%), work limitation (30%), and severe joint pain (27%) than do men with arthritis. 5
Since 1999, the Centers for Disease Control and Prevention (CDC) has spearheaded the public health response to reduce the burden of arthritis. CDC's activities have been guided by two key public health documents: Healthy People 2010 and the National Arthritis Action Plan: A Public Health Approach. Healthy People 2010, the nation's 10-year blueprint for health, was published in 1999 and included, for the first time, arthritis-specific health objectives for the United States. 6 Concurrently, the Association of State and Territorial Health Officers, the CDC, and the Arthritis Foundation (AF) published the National Arthritis Action Plan: A Public Health Approach, which outlined priority public health strategies for reducing the burden of arthritis. 7 Simultaneously, CDC received its first congressional appropriation to address arthritis.
Central to CDC's public health response has been funding state health departments to address arthritis, primarily through the dissemination and implementation of evidence-based self-management interventions, specifically packaged (i.e., ready to use, with standardized implementation procedures) self-management education and physical activity intervention programs. 8 These community-based public health interventions are complementary to the traditional care provided in clinical settings. The American College of Rheumatology's guidelines for the management of rheumatoid arthritis and osteoarthritis of the hip and knee all highlight the importance of self-management education and appropriate physical activity. 9,10 Recommendations to participate in these community-based self-management interventions can be an important component of self-management support provided by healthcare practitioners. 11
When CDC first began funding state arthritis activities in 1999, only three community-based self-management education or physical activity interventions, with varying degrees of evidence to document their benefits for people with arthritis, were available. All three are disseminated by the AF. These included the Arthritis Self-Help Course (also known as the Arthritis Self-Management Program), 12 the Arthritis Foundation Aquatics Program, and the People with Arthritis Can Exercise (PACE) program. 13
A key focus of the CDC Arthritis Program has been to expand the number of community-based interventions available both by funding the development and evaluation of arthritis-appropriate physical activity and self-management education interventions and by screening existing or newly developed community-based interventions to assess their suitability for a public health approach to reducing the impact of arthritis. The purposes of this report are to describe the process and criteria used by the CDC Arthritis Program to screen potential intervention programs and to report the results of that screening, including an updated list of intervention programs recommended for dissemination by state arthritis programs, their partners, and other public health agencies interested in improving the quality of life of people with arthritis.
Materials and Methods
The initial screening focused on PA interventions, because a quick scan of the literature suggested there were more packaged PA interventions available than packaged SME interventions. In consultation with subject matter experts, CDC developed a series of three sets of screening criteria to guide the assessment of these interventions. Experts in PA and arthritis were consulted to help develop the criteria to determine whether the PA intervention program was arthritis appropriate. The CDC Arthritis Program scientific staff developed criteria to assess the adequacy of the evidence base, and state health department arthritis coordinators were consulted in the development of criteria to judge the implementability of the intervention program in settings typically used by state arthritis programs. Table 1 lists the three sets of screening criteria for interventions. These criteria were used to guide the judgments of the research team screening the interventions and formulating recommendations.
Five intervention categories were created based on the intervention screening criteria, ranging from Recommended to Unlikely to Meet Criteria. Those interventions that met all three sets of criteria (arthritis appropriateness, adequacy of evidence base, and implementability in public health settings) were designated Recommended interventions. Interventions that met the arthritis-appropriate and adequate evidence base sets of criteria and were building the infrastructure necessary to be implementable on a wide scale were designated Promising Practices. Interventions that met arthritis-appropriate criteria and were in the process of building their evidence base (i.e., had evaluation underway) were placed on the Watch List, and interventions that seemed arthritis appropriate but needed additional evidence and the structures to support widescale implementation were identified as Future Possibilities. Interventions that required an extensive amount of implementation resources not often found in public health settings were categorized as Unlikely to Meet Criteria. Any intervention with insufficient information available to allow categorization was listed as Unable to Screen. Figure 1 outlines the decision tree used in categorizing interventions.
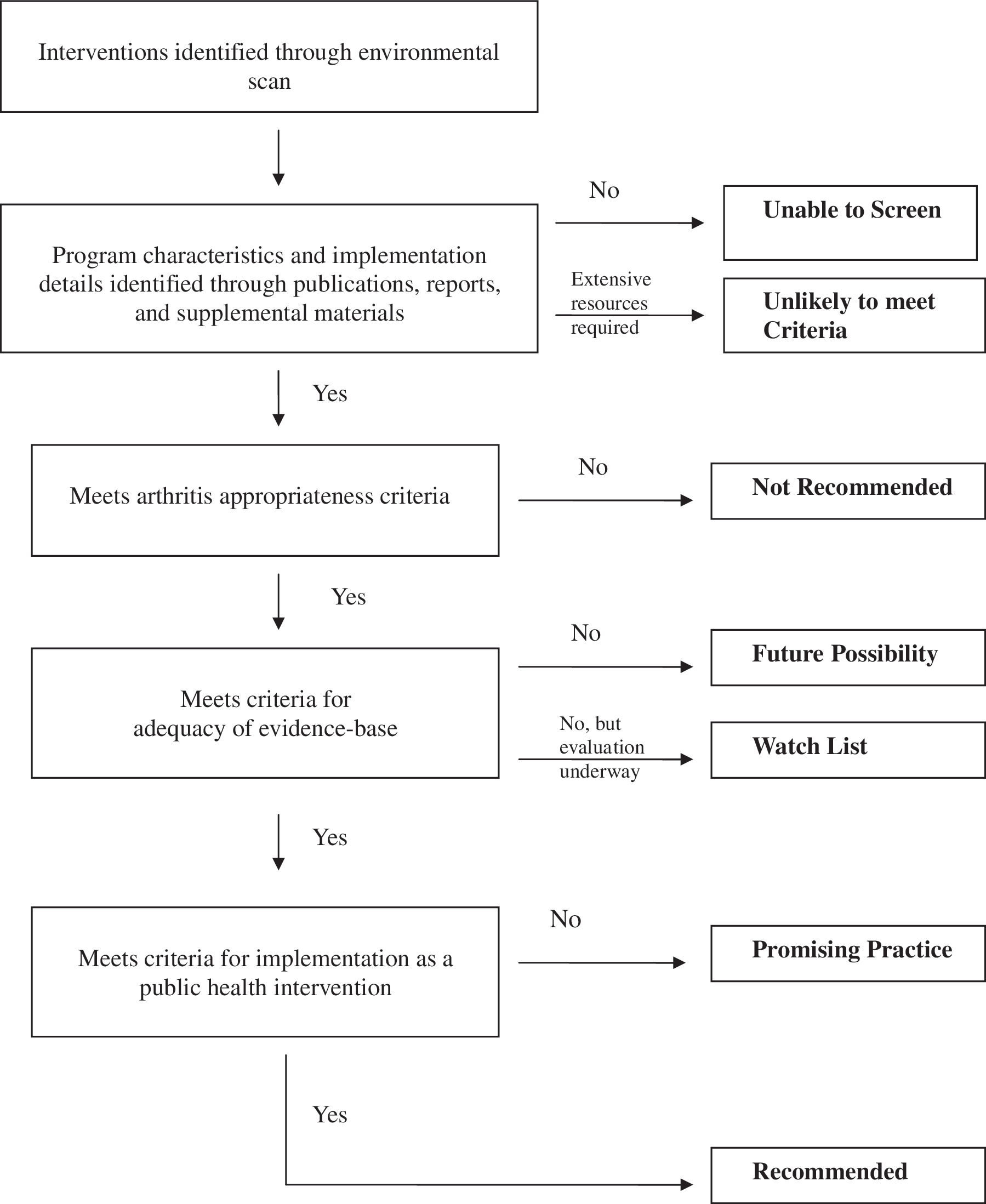
Flow diagram of decision process for assigning intervention categories using standard criteria.
A broad-based environmental scan was used to identify physical activity interventions for screening. The intervention screening team sought nominations for interventions that were appropriate for people with arthritis and deliverable through a state health department from state arthritis coordinators, arthritis subject matter experts, and staff from other CDC chronic disease programs (cancer, cardiovascular health, diabetes, and nutrition and physical activity). A brief literature search was also conducted. Medline, Embase, and Cinhal databases were searched with the search terms arthritis, exercise, and physical activity. Search results were informally reviewed by two members of the intervention screening team (S.L.J., T.J.B.) to identify interventions that appeared to have some possibility for being arthritis appropriate and deliverable through a state health department. The formal screening process was used to screen the interventions identified through this broad environmental scan.
Information was gathered on each identified intervention, including program components; participant, leader, and trainer manuals; implementation guides; implementation costs and procedures; and evaluation reports. Intervention developers and evaluators were contacted to provide the additional information not available in published reports as well as information about evaluations underway. Using a standardized abstraction form, one member of the research team (S.L.J.) abstracted information for all criteria for each intervention from the published articles, developer/evaluator information, and supplemental materials and placed that information onto an intervention summary sheet.
All intervention summary sheets were reviewed by all members of the intervention screening team (T.J.B., J.M.H., S.L.J., J.E.S.); each member independently judged how well each intervention met the screening criteria and whether or not it could be recommended. Discrepancies were resolved by consensus after discussion by the screening team and review of the published articles, developer information, and supplemental materials. Screening team discussion also was used to assign interventions that did not appear to meet all three sets of screening criteria to the appropriate intervention category.
A modified process was followed for screening and rating SME interventions. The criteria developed for screening PA programs were adapted slightly by the CDC Arthritis Program staff to fit the content and processes of educational interventions. Nominations for interventions to be screened were sought from arthritis state coordinators and subject matter experts. A brief literature search of Medline, Embase, Cinhal, and PsychInfo databases was conducted using search terms including arthritis, self-care, self-management, and patient education. The identified SME programs were screened and assigned to categories (Recommended, Promising Practice, Watch List, and Future Possibilities) based on discussion by the full CDC Arthritis Program staff.
The initial screening of interventions took place in 2005, and it was updated in 2007 and in 2009.
Results
A total of 15 packaged PA programs and 6 packaged SME programs were identified for screening. The current status of all interventions screened through these processes is shown in Table 2. Among PA programs, three intervention programs (EnhanceFitness, 14 Active Living Every Day, 15 and Fit & Strong! 16 ) were added to the menu of Recommended interventions six have evaluations underway and were placed on the Watch List, and an additional four were categorized as Future Possibilities. Two packaged PA interventions were rated as Unlikely to Meet Criteria, and one intervention (Silver Sneakers 17 ) did not include enough information in the public domain to complete the screening process.
Of the SME programs, three interventions were added to the Recommended interventions listing (the Chronic Disease Self-Management Program, 18 the Spanish Arthritis Self-Management Program, 19 and the Spanish Chronic Disease Self-Management Program, 20 ), two were listed as Promising Practices, and two were listed as a Future Possibilities.
Descriptions of the recommended interventions and promising practices are included in Table 3. All the recommended interventions meet the criteria for arthritis appropriateness of the PA or SME intervention itself and have been evaluated in their current form. All the recommended interventions measure arthritis-relevant outcomes and have documented that evidence through either a published journal article or written report and have a sample size of at least 75 people. Most importantly, the recommended interventions are feasible for implementation in a public health setting commonly used by state arthritis programs (i.e., have limited leader, site, and equipment requirements) and have structures such as leader training, implementation guides, and technical assistance available to support their implementation. The interventions listed as promising practices meet the arthritis-appropriateness criteria, have evidence supporting their efficacy or effectiveness in the present form of the intervention and are in the process of developing the implementation supporting structures.
All Stanford University Patient Education Research Center interventions can be covered under the same license and fee. License fees depend on number of courses offered per year, but a single license can cover multiple interventions.
Discussion
A total of six packaged PA and SME interventions were added to the list of Recommended interventions; these six were judged to be appropriate for people with arthritis, to have documented health benefits, and to have the infrastructure and program characteristics needed to facilitate widescale dissemination and implementation by public health agencies and their community partners. This brings the total number of Recommended interventions to nine, including the original Arthritis Foundation-disseminated interventions in use when the CDC Arthritis Program began in 1999. An additional two interventions are considered Promising Practices.
Two salient issues need to be addressed by several of the interventions that have not yet qualified as Recommended: lack of evidence and lack of infrastructure and materials to support implementation. In some cases, intervention developers continue to build their evidence base; in others, developers have yet to develop trainer/instructor manuals and implementation guides, to plan training events, or to have a mechanism to answer questions from the field. The lack of adequate supporting structures to support widescale dissemination and implementation makes the intervention impractical for wide use. These elements are essential to the successful translation of a research project into a public health intervention. 61
A small number of interventions was rated as Unlikely to Meet Criteria as a community-delivered public health intervention because of the high resource requirements for program delivery. Extensive site, equipment, or program implementer requirements make it unlikely that an intervention will be deliverable on a population basis through the public health system.
The majority of intervention programs added to the list of Recommended interventions are arthritis appropriate but not designed exclusively for people with arthritis. This can be advantageous both for the individual participant/patient and for the organizations offering the programs. More than half the people with arthritis have another chronic condition, 62 and over half the people with diabetes or heart disease also have arthritis, 63,64 so offering programs that promote generic self-management skills can allow patients with multiple chronic conditions the opportunity to meet their multiple needs. Similarly, organizations offering these interventions may not have the resources to offer a wide variety of disease-specific services, but may find sustaining programs easier when they meet the needs of multiple patient/population groups. The CDC Arthritis Program is currently supporting efforts to expand the implementation of these programs among groups with a range of chronic conditions.
Two of the interventions added to the list of Recommended SME interventions are offered in Spanish and are designed specifically to meet the needs of Spanish-speaking people with chronic disease. 19,20 These two interventions are not mere translations of English interventions but are developed based on needs assessments of Spanish-speaking people with arthritis or chronic disease and are designed to be culturally appropriate for that population. These Spanish language interventions are important because between 1970 and 2000, the Hispanic population in the United States grew by 26 million; nearly half of that growth was due to immigration. 65 Although the prevalence of doctor-diagnosed arthritis is reported to be lower among Hispanics than Caucasians, Hispanic people with arthritis report a higher proportion of work limitations and severe joint pain than do non-Hispanic Caucasians. 66
Several of the interventions on the Promising Practices list, such as The Arthritis Toolkit 21 and the internet-delivered ASMP, 22 offer new ways of delivering programs, beyond the small group model typical for community-delivered public health interventions. These new delivery modes can help meet the needs of people who do not have the time, resources (like transportation), or inclination to attend a small group PA or SME program. Because at present, 44% of people with arthritis are inactive 67 and only 11% of people with arthritis report attending a course or class to help solve problems related to arthritis, 68 it is clear that these new modes of program delivery are essential to meeting the needs of people with arthritis. Several more of these self-directed or self-study interventions are on the Watch List, and their availability will be eagerly awaited.
Conclusions
Using a systematic process allowed the CDC Arthritis Program to review a wide array of potential intervention programs to identify those arthritis-appropriate evidence-based interventions that can be effectively and efficiently offered through a state health department or in a public health setting. Many promising interventions, whether developed in the field or as research projects, have not built the necessary evidence base or infrastructure. Public health resources are too scarce to recommend programs that have not demonstrated and reported effectiveness. Adequate infrastructure also is necessary for an intervention to be used as a widespread public health intervention. The categorization of interventions by the adequacy of their science base and implementability as a public health intervention can inform intervention developers and evaluators on gaps that need to be filled to prepare an intervention for widespread public health implementation and can inform funding agencies on promising interventions for further intervention research.
Expanding the list of recommended interventions with three SME interventions and three PA interventions is good news for people with arthritis and for both public health and clinical care practitioners. For public health practitioners, it expands the menu of program offerings that can help meet the needs of their constituents with arthritis (and other chronic conditions), and it facilitates partnering with a wider variety of delivery system partner organizations. This expanded list of Recommended interventions provides clinical care providers with a wider array of evidence-based interventions to recommend to their patients with arthritis, and the screening process can give them confidence that these Recommended intervention programs have documented health benefits. Finally, this expanded list of Recommended interventions, both arthritis specific and generic to chronic disease, are beneficial for people with arthritis. This review process can increase their confidence in the merits of these interventions, and the wider array of interventions and potential program delivery organizations can increase their opportunities to participate in these community-based SME and PA interventions that are designed to help them improve their quality of life.
Footnotes
Acknowledgments
The findings and conclusions in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Disclosure Statement
No competing financial interests exist.