
Abstract
Aims:
To determine predictors of adherence to cervical cancer screening guidelines among women working in Monterrey, Mexico. Cases (n = 94) were sexually active female store clerks working in Monterrey, Mexico, aged 18–64, who were not adherent to Official Mexican Standard cervical cancer screening guidelines; controls (n = 135) were adherent to guidelines. The outcome of interest was adherence to cervical cancer screening services according to national screening guidelines.
Methods:
Multivariate logistic regression analyzed knowledge factors and perceptions associated with adherence.
Results:
Having no or inaccurate knowledge of screening guidelines (odds ratio [OR] 11.1, 95% confidence interval [95% CI] 4.3-28.5) and no knowledge of Pap examination utility (OR 6.8, 95% CI 1.0-46.4) were associated with screening guideline nonadherence. Perceptions of fear/embarrassment (OR 16.2, 95% CI 5.1-51.5) and lower levels of spousal/partner acceptance (OR 5.8, 95% CI 1.3-25.3) of the Pap examination were associated with screening guideline nonadherence. Results were adjusted for age at initiation of sexual activity, civil status, level of education, use of family planning/birth control, and income.
Conclusions:
Identification of knowledge factors and perceptions that predict screening guideline adherence can inform population-specific recommendations to increase screening and reduce cervical cancer morbidity and mortality among employed Mexican women.
Introduction
In Mexico, approximately 12,516 new cases of cervical cancer are diagnosed each year, with a crude incidence rate of 24.4/100,000 women. It is the most frequent cancer among Mexican women, with an age-stratified incidence rate of 29.5/100,000 women. The overall cumulative risk for developing cervical cancer is 2.0. 1 Cervical cancer is also the most common lethal cancer among Mexican women (ranked eleventh among all causes of female mortality in 2005) and causes roughly 5,777 annual deaths, with a mortality rate of 7.5/100,000 women and cumulative risk of 0.9. 2,3
Genital human papillomavirus (HPV), the cause of cervical cancer, is the most common sexually transmitted disease (STD) globally and is highly prevalent among women of reproductive age. 3 –6 In Mexico, HPV prevalence among females is 11.0% (95% confidence interval [CI] 9.7-12.3), and the virus is detected in 91.5% (95% CI 85.3-95.7) of all cervical cancer cases. 3 Risk factors for contracting HPV include higher number of lifetime sexual partners, 7 younger age at first intercourse, 8,9 sexual activity before the age of 19, 10 and higher parity. 11
The Papanicolaou (Pap) examination is the most effective screening test for increasing early intervention opportunities to reduce cervical cancer incidence and mortality. 11 Despite the effectiveness of Pap screening, however, cervical cancer continues to plague the developing world, where screening program coverage does not adequately reach high-risk women. 8 In Mexico, a national screening program has been in place since 1974, and the Official Mexican Standard, Normal Oficial Mexicana (NOM), for the prevention, detection, and control of cervical, uterine, and breast cancer in primary care recommends that sexually active women or those >age 25 obtain an annual Pap examination. 12,13 Despite the national screening program and guidelines, incidence and mortality rates have remained fairly constant. 14 Nationwide, an estimated 50% of women and 30% of sexually active women have never received a Pap examination, and the Pap examination rate is estimated at 35%. 15
Screening service use has been shown to be related to knowledge factors and perceptions of cervical cancer and the pelvic examination. 16 –18 Knowledge factors may include a woman's specific knowledge about cervical cancer and the Pap examination, whereas a woman's perceptions toward Pap examination use may be related to various organizational and sociocultural factors. 17,19,20 Previous studies have reported several factors that significantly predict cervical cancer screening use (Fig. 1). In Latin American and Caribbean (LAC) countries, organizational factors, including limited accessibility of medical services and poor medical personnel attention, have been reported, and fear of cancer and death and failure to prioritize personal health are often cited as potential sociocultural barriers to screening. 17,21,22
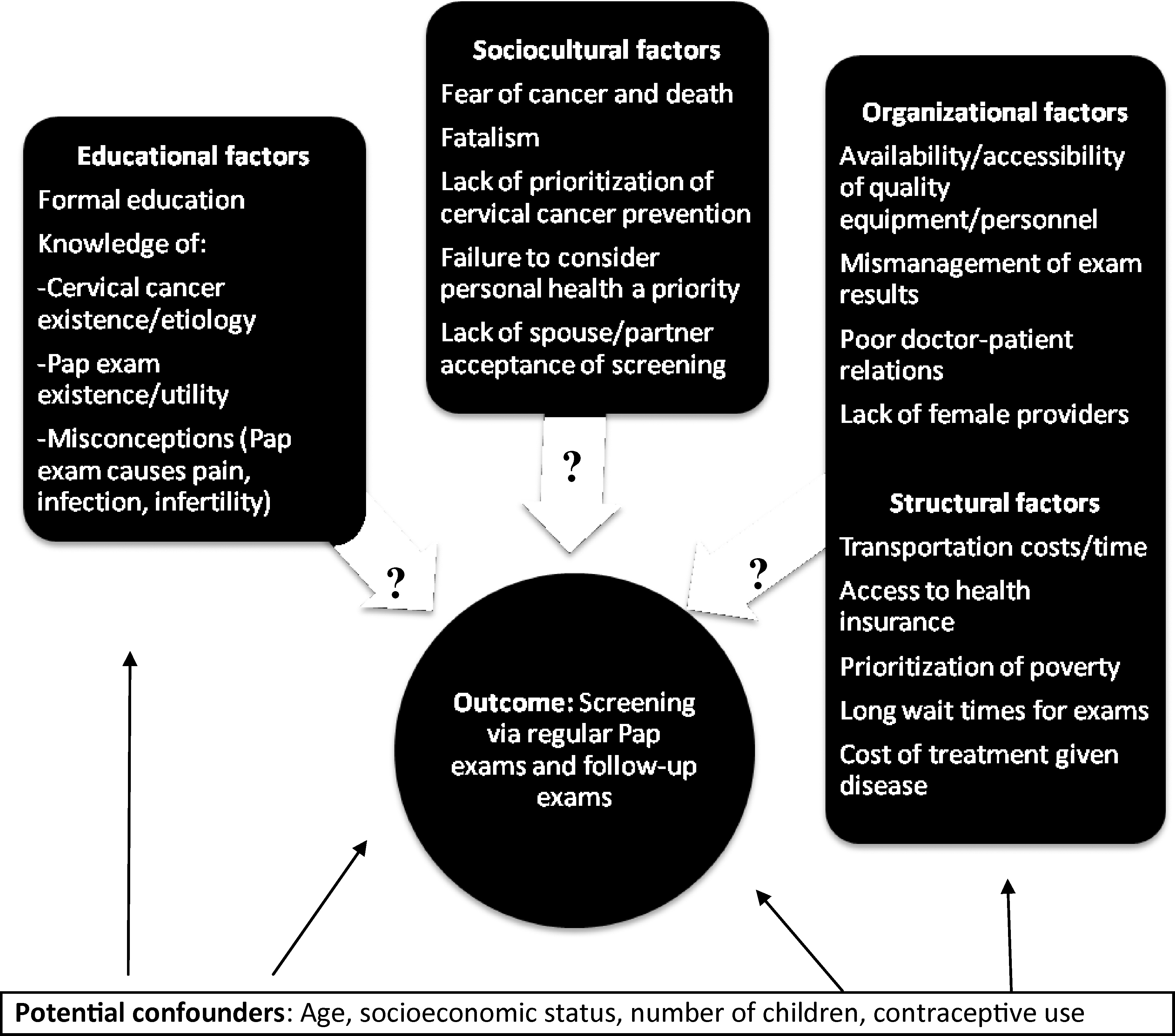
Conceptual model for potential cervical cancer screening use predictors.
Few studies consider both the objective state of knowledge and subjective perceptions of cervical cancer screening held by working Mexican women. The high prevalence of cervical cancer and consistently low rates of Pap examination use in Mexico clearly indicate the need to further explore both types of screening barriers. Additionally, the health of the economically productive female population can greatly affect economic and workforce productivity and have a high social cost within the family unit. Information from this study adds to the current state of knowledge about modifiable barriers to cervical cancer prevention via early detection among working Mexican women and allows for recommendations to increase Pap examination use in this population.
Materials and Methods
Study design and sample population
Data collected in a case-control study during September–November of 2006 in Monterrey, the third largest urban area in Mexico, investigated predictors of cervical cancer screening guideline adherence. Cases were sexually active female store clerks aged 18–64 who did not adhere to NOM cervical cancer screening guidelines. Controls were sexually active female store clerks aged 18–64 who did adhere to NOM guidelines. The operational definition of the outcome, adherence to NOM guidelines, was defined as receiving an annual Pap examination on initiation of sexual activity, given a previous normal Pap result, or receiving a 6-month follow-up Pap examination, given a previously abnormal Pap result.
All participants were formally employed as convenience store clerks by businesses in the formal sector of the Mexican economy. These establishments generally comprise <500 square meters of space and typically operate >18 hours a day, 365 days a year. In accordance with federal employment laws in Mexico, all formally employed workers and, therefore, all participants of this study, are affiliated with the Mexican Institute of Social Security (Instituto Mexicano del Seguro Social) (IMSS) and are provided with social security and healthcare services, including free Pap screening services.
Female store clerks were selected because they are a vulnerable group with high economic and social impact in Mexican society. Specifically, we included women employed as store clerks because of their ability to respond to the survey in their place of business during their working hours, unlike women in other businesses, such as manufacturing. Thus, clerks could easily be surveyed without the influence of peers or family. Additionally, as these women are formally employed (a large percentage of the working female population work in the informal sector), they are provided access to government health services. Women with a history of cancer were excluded, as their screening behaviors are not likely to represent the general population.
A minimum sample size of 78 cases and 78 controls was established using EpiCalc 2000 (version 1.02, Gilmann and Myatt) for an α-level of 0.05 and 80% power to detect an odds ratio (OR) of 2.5, given the hypothesis that risk factors for nonadherence to Pap examination screening guidelines were present in 50% of the cases and ≥33% of the controls.
Survey administration
Information on breast and cervical cancer screening use among women working in Monterrey was captured using a 63-item self-administered survey. Surveys written in elementary level Spanish were pretested with 15 employed women (10 store clerks, 3 waitresses, and 2 administrative assistants) and revised to improve understanding. Surveys were administered at 312 randomly selected businesses throughout Monterrey, proportioned by district and working shift hours (morning, afternoon, and evening). The study was explained to eligible clerks, and surveys were left with participants in their place of work and collected within 2 hours. Most women surveyed (94%) were the only workers present at the place of business; when more than one eligible worker was present, the importance of each woman responding individually was stated, and surveys were administered to both women.
Of the 379 women approached to participate in the study, 87.1% provided written authorization after reading the letter of informed consent; 12.9% declined to participate. Reasons for declining included not having enough time (91.8%) and believing that cancer is incurable (8.2%). Six women (1.8%) were excluded for not completing at least 80% of the questionnaire. Of the 324 completed surveys, 241 participants were sexually active, had no history of cancer, and had not undergone a hysterectomy. Of those who completed the study, 94 were classified as cases and 147 as controls based on their questionnaire responses. These cases and controls were then age-matched in a 1:1 ratio within 5-year age group distributions. To achieve this equal distribution (±5% age difference within the 5-year age groups), 12 controls aged 33–37 remained unmatched. Therefore, 12 controls were randomly removed from a sample frame comprising all the controls aged 33–37, resulting in 135 controls. The authors considered the reinclusion of these excluded women by performing the analysis with the entire population. This did not give results and conclusions different from those presented here. Study methodology and protocol measures were approved by the Local Committee in Ethics and Health Research of the Monterrey Mexican Social Security Institute.
Survey measures
Survey items measured variables of interest, including sociodemographics, cancer screening practices, educational factors, and organizational and sociocultural perceptions related to the Pap examination. Response choices were (1) open-ended, (2) categorical and yes/no, or (3) ranked on a 5-point Likert scale.
Sociodemographic variables included age, years of formal education, age during first childbirth, total number of pregnancies, total number of children living, age at initiation of sexual activity, and past screening practices, such as number of lifetime Pap examinations and number of Pap examinations in the previous 3 years (captured as open-ended responses), as well as weekly hours of work, monthly familial earnings, civil status, having more than one sexual partner, history of gynecological symptoms, lifetime use of family planning methods, current form of family planning used, current occupation, and working shift (captured as categorical and yes/no responses).
Variables describing knowledge factors included knowledge of cervical cancer (any awareness of the existence of cervical cancer and potentially how it is transmitted), the existence of the Pap examination, the utility of the Pap examination, and national screening recommendations. Knowledge of screening guidelines were defined as a woman's knowledge of how often to receive a Pap examination in accordance with the NOM. Specifically, respondents were asked: Do you have any knowledge of cervical cancer? (categorical yes/no). Are you aware of the existence of the Pap examination? (categorical yes/no). What is your knowledge of the utility of the Pap examination? (5-point Likert scale ranging from no knowledge to very high). Do you know the national cervical cancer screening guidelines? (categorical yes/no).
Organizational factors included perceptions of sufficiency of time to obtain a Pap examination, wait time to receive an examination, wait time to receive examination results, and sufficiency of Pap examination personnel and equipment. Specifically, respondents were asked: How much time do you have to obtain a Pap examination? (5-point Likert scale ranging from none to more than sufficient). How do you perceive the wait time to receive Pap examination? results (5-point Likert scale ranging from very long to very little). How is the sufficiency of the equipment and personnel for Pap examination? (5-point Likert scale ranging from no sufficiency to more than sufficient).
Sociocultural variables evaluated fear or embarrassment to receive a Pap examination, beliefs that cancer is invariably fatal, and spousal/partner acceptance of the Pap examination. Specifically, respondents were asked: Do you think cancer is invariably fatal? (5-point Likert scale ranging from invariably fatal to low fatality). Do you have any fear or embarrassment related to obtaining a Pap examination? (5-point Likert scale ranging from very high fear/embarrassment to none). Does your spouse or partner accept that you receive a Pap examination? (5-point Likert scale ranging from no acceptance to very high, with the option of selecting no spouse or partner).
Statistical analyses
STATA release 10.0 statistical software (StataCorp) was used to conduct statistical analyses. Descriptive analyses determined means and standard deviations (SD) of responses to continuous variables and percentages of responses to categorical variables. Significant differences in continuous and nominal variables between cases and controls were identified using Student's t tests and chi-square tests, respectively.
Results
Crude ORs between individual exposures (knowledge factors and organizational and sociocultural perceptions) and adherence to screening guidelines were calculated. Multiple logistic regression models were built using variables significant in univariate analyses. Model 1 considered sociodemographic variables and knowledge factors as potential determinants of adherence to Pap examination screening guidelines. Model 2 considered sociodemographic variables and the subjective organizational and sociocultural perceptions associated with cervical cancer screening as potential determinants of adherence.
Variables within each model were first tested for collinearity. Age at first childbirth and age at initiation of sexual activity were collinear (correlation coefficient 0.7529, p < 0.01); age at first childbirth was removed to retain the sample size, as only 177 women had at least one childbirth. Participant age and number of children living were collinear (correlation coefficient 0.6550, p < 0.01) but were retained because both are significantly associated with Pap examination screening in the literature. Awareness of Pap examination utility and knowledge of the existence of the Pap examination were collinear (correlation coefficient 0.7705, p < 0.01), and the latter was removed as it defines, but does not necessarily predict, case status.
Variable selection was accomplished using the likelihood ratio test in univariate analysis (cutoff of p < 0.25) or clinical importance. Variables significant in univariate analysis were included in a multivariable model, and those with nonsignificant (p > 0.05) Wald statistics were removed. Age at initiation of sexual activity (the only continuous variable included) was checked for linearity in the logit of both models. The knowledge factors: Awareness of Pap examination and Awareness of Pap examination utility were significant but were not included in the final model because of low sample size (n = 2 controls reporting the risk factor).
In model 1, potential interactions were considered between education and income, education and ever having used birth control, and education and knowledge of Pap examination screening recommendations. In model 2, potential interactions were considered between education and income and education and ever having used birth control. Likelihood ratio tests for the significance of individual interaction terms found no significant interactions.
The overall fit was assessed via the Hosmer-Lemeshow test for model 1 (4.66, df = 8, p = 0.7929) and model 2 (5.77, df = 8, p = 0.6726), indicating that the fit of both models is adequate. The area under the ROC curve for model 1 (area under ROC curve = 0.92) and model 2 (area under ROC curve = 0.91) indicated that the models have excellent ability to discriminate between those who adhere and those who do not adhere to screening guidelines. Diagnostic statistics were considered to identify poorly fit or overly influential covariate patterns. Two potential outliers with overly influential diagnostic statistics were identified in model 1. When removed from the model, neither of the outliers significantly changed the point estimates and were, therefore, retained. No potential outliers were detected in model 2.
Sociodemographic profile
Cases reported having their first child and initiating sexual activity at significantly younger ages than controls. Significantly more cases than controls were unmarried or separated at the time of the survey, had no previous gynecological symptom requiring medical attention, did not use family planning or birth control previously or at the time of the survey, were of lower education, and had a lower monthly familial income. Number of pregnancies, number of children living, number of hours worked per week, and having more than one sexual partner were not significantly different between cases and controls (Table 1).
Among women with at least one childbirth (63 cases, 114 controls).
Chi-square calculated by adding 0.5 to zero cell.
SD, standard deviation.
Univariate analysis
Univariate analysis revealed that cases were significantly less likely than controls to report having any knowledge of cervical cancer or the Pap examination, knowledge of the utility of the Pap examination, and knowledge of Pap examination screening guidelines. Cases were also less likely to report having sufficient time to obtain a Pap examination, that the wait time to receive Pap examination results is reasonable, and that sufficient Pap examination equipment and personnel are readily available. Cases were more likely to report increased fatality beliefs and fear/embarrassment about the Pap examination, and less spousal/partner acceptance of the Pap examination (Table 2).
Adjusted for age at initiation of sexual activity, civil status, level of education, previous or current use of family planning/birth control, and income.
The knowledge factors, Awareness of Pap examination and Awareness of Pap examination utility, were significant but were not included in the final model due to low sample size (n = 2 controls reporting the risk factor).
Among women with at least one Pap examination (36 cases, 135 controls).
Includes women with no spouse or partner.
CI, confidence interval; OR, odds ratio; Ref, reference group.
Multivariate analysis
Cases were 7 times more likely to be unaware of Pap examination utility, although this association was approaching significance (p = 0.051). Cases were 11 times more likely to have no or inaccurate knowledge of national cervical cancer screening guidelines (p < 0.01). These results were adjusted for age at initiation of sexual activity, civil status, level of education, previous or current use of family planning/birth control, and income (Table 3).
Adjusted for age at initiation of sexual activity, civil status, level of education, previous or current use of family planning/birth control, and income.
CI, confidence interval; OR, odds ratio; Ref, reference group.
Sufficiency of equipment and personnel for Pap examination and cancer fatality beliefs were not significantly associated with nonadherence to cervical cancer screening guidelines in multivariate analyses. Higher levels of fear or embarrassment of the Pap examination were over 16 times more likely in cases than controls (p < 0.01). Cases were almost 6 times more likely than controls to report lower levels of spousal/partner acceptance of the Pap examination (p = 0.02). These results were adjusted for age at initiation of sexual activity, civil status, level of education, previous or current use of family planning/birth control, and income (Table 4).
Adjusted for age at initiation of sexual activity, civil status, level of education, previous or current use of family planning/birth control, and income.
CI, confidence interval; OR, odds ratio; Ref, reference group.
Discussion
In this population, nonadherence to screening guidelines was associated with lower education, lower familial income, and poor knowledge of screening guidelines and Pap examination utility. Perceptions of fear or embarrassment and lower levels of spousal/partner acceptance of the Pap examination were also associated with nonadherence in this population.
The finding that, significantly, cases had lower education and familial income is consistent with previous investigations in which women with low socioeconomic status and formal education are more often diagnosed with later stages of cervical cancer. 23,24 A cross-sectional study in Mexico City, Mexico, to determine demographic and educational predictors of Pap use among women working at different social levels (110 university professors and 118 university administrators) showed that both income and years of formal education related positively with knowledge about cervical cancer. Formal education (but not income) related positively with knowledge of the cervical cancer screening program. This study concluded that socioeconomic inequalities among Mexican women are reflected in differences in knowledge and practice of Pap examinations, and that these differences are associated primarily with level of education. 21
It is interesting that although the population of Nuevo León has higher socioeconomic growth and a higher percentage of women in social security than the national level (69.7% vs. 47.7%, respectively), the use of the Pap test is below the country average. Also, the higher frequency of women with formal employment who are entitled to social security in Nuevo León relative to the national level (59.2% vs. 40.1%) is notable, explaining the findings that barriers are related to accessibility factors and not to health coverage. 15,21 This indicates that although higher education and income are significantly associated with increased screening, these factors alone are not sufficient for high Pap examination screening use.
In multivariable analysis, this study found two knowledge variables associated with adherence to cervical cancer screening guidelines independent of level of education or familial income: knowledge of the national cervical cancer screening guidelines and awareness of the utility of the Pap examination. Roughly 68% of cases and 93% of controls reported knowledge of cervical cancer screening guidelines, and 69% of cases and 99% of controls reported awareness of the utility of the Pap examination.
These finding are consistent with other studies in Mexico and LAC countries. Among women with history of at least one Pap examination, Pap tests were perceived as necessary but only given prior gynecological symptoms. 16,19 A cross-sectional study in Mexico City among 2107 women of reproductive age using one family planning service determined that women reporting accurate knowledge of the utility of the Pap examination were six times more likely to use this screening service. 25 In a cross-sectional study of 105 women aged 25–65 in Monterrey, only 43% of women reported receiving any information on the Pap examination, and 70% of the participants had insufficient (<70%) knowledge scores about the Pap examination with an average score of 53%. Misconceptions were also common: 36% of women believed that the Pap examination is painful, and 21% believed that it may cause infection. 10
Although poor knowledge of Pap examination guidelines and utility was a significant barrier to adherence, most women did report knowledge of the existence of cervical cancer (83% of cases and 96% of controls) and are, therefore, receiving at least basic information from healthcare personnel, the media, or personal relations. Many women also reported some current family planning method requiring a doctor's visit (oral contraceptive, IUD, or injections) (22% of cases and 51% of controls) or a history of gynecological symptoms requiring medical attention (16% of cases and 29% of controls), providing opportunities for women to receive information from medical personnel about Pap examination utility and screening guidelines. The Secretary of Health (Secretaría de Salud) is the director of the Mexican Health System and is responsible for cervical cancer prevention and education through the Specific Action Program on Cervical Cancer 2007–2012) (Programa de Accion Especifico de Cancer Cervico Uternino 2007–2012). In addition to reiterating the NOM, this program gives health promotion messages about Pap examination utility and screening guidelines directed at the general population as well as medical care providers. 26
Although organizational factors were not significantly associated with adherence to screening guidelines in multivariate analysis, fear or embarrassment of the Pap examination and spousal/partner acceptance were perceived as significant barriers to screening. Fear or embarrassment and spousal/partner acceptance of the Pap examination have been reported previously as important barriers to screening use. Among Mexican women, rejection of the pelvic examination (specifically because of feelings of modesty, shame, invasion, or domination opposition by their male sexual partners) has been reported. 19 In a descriptive study of 290 women in Nuevo Leon, 15% cited fear as the main reason for never having received a Pap examination, and this study concluded that fear is a principal factor preventing its use in this population. 27 Similarly, in a cross-sectional study of 105 women aged 25–65 in Monterrey, 70% of participants reported embarrassment, 63% reported anxiety, 34% expressed anguish during wait times to receive examination results, and 25% reported male partner negation of the Pap examination. 10
The significant knowledge, organizational, and sociocultural variables identified here are modifiable and may be used to affect screening compliance despite study limitations. In addition to the opportunities mentioned previously for healthcare providers to disseminate knowledge about Pap examination utility and screening guidelines, other forums may be used to address perceived organizational and sociocultural barriers to Pap test use. Interventions that engender trust and acceptance of the Pap examination while imparting knowledge about cervical cancer screening are clearly needed. Community organizations or religious meetings would be potential outlets for focusing on the perceptions identified as barriers to screening use. Future research could focus on the design and efficacy of such interventions to increase screening use based on these recommendations.
A limitation of this investigation is potential recall bias in accurate reporting of cervical cancer screening practices. For example, recalling lifetime number of Pap examinations is likely to be an estimate by many participants, especially those who are older and those cases who have received at least one examination but have not adhered strictly to screening guidelines. Therefore, controls, those women who adhered to guidelines, were more likely to recall their cancer screening practices accurately.
Additionally, the potential for information bias exists in the accurate disclosure of personal information. Women may be hesitant to report having multiple sexual partners, their age at initiation of sexual activity, and monthly familial income. We attempted to minimize this bias by surveying women outside the home, typically when they were alone at work, and by ensuring participant confidentiality. Our selection of store clerks implies a selection bias. There is a nondifferential selection bias in the choice of formally employed women because working women face barriers unemployed women do not, such as higher time constraints as lack of opportunity to obtain health services during working hours, among other obstacles. Meanwhile, their free time often is divided spent on household tasks, and they often prioritize the health of other family members above their own. 28,29 This potentially limits the applicability of our results to an unemployed population.
Self-selection bias may exist, as the women had control over whether or not to participate. Women more likely to take an active role in their healthcare or to have strong feelings toward the government-provided healthcare system may be more responsive to taking the survey. Finally, because only literate women were included in the study, this nondifferential selection bias could limit applicability of the results to an illiterate population. Also, the small sample size of the study restricts applicability of the results to working women in urban Mexico; the study must be repeated with larger numbers and in other populations to confirm these findings and to allow for generalizations beyond this population. Finally, confounding bias may be present because of incomplete assessment of potential confounders. There is a particular need for further consideration of socioeconomic status, which is consistently indicated in the literature to be a critical confounder in the relationship between the selected screening barriers and screening guideline adherence.
Footnotes
Acknowledgments
We are grateful to Dr. Judith Dunn for statistical support and Dr. Kristy Murray for editorial comments.
Disclosure Statement
The authors have no conflicts of interest to report.