
Abstract
Objective:
To assess the acceptability of a daily pill for prevention of HIV acquisition among 400 Ghanaian women in the oral tenofovir disoproxil fumarate (TDF) clinical trial.
Methods:
Structured questionnaires were conducted with women enrolled in the trial at enrollment and at each of the 12 monthly follow-up visits. Growth curve analysis was used to examine adherence patterns over time. Qualitative interviews were carried out with a subsample of the clinical trial population, and thematic analysis was applied to these data.
Results:
Overall, acceptability of the pill was good. Adherence remained > 82% throughout the 12-month trial. Consistent access to the pill and study assignment were both associated with adherence. Most reported problems diminished over time as women became accustomed to the pill and developed strategies to incorporate pill taking into their daily routines.
Conclusions:
If daily preexposure prophylaxis (PrEP) for HIV is found to be efficacious and has as few physical side effects as TDF, acceptability of this method among women in the study population may not be problematic. However, future studies must develop better acceptability measures, in order to more fully address the relationship among adherence, safety, and effectiveness.
Introduction
The HIV pandemic continues to grow, and condoms are still not commonly used in most regions of the world. 1 One reason has to do with the lack of female control over sexual health decisions, including condom use. 2,3 Power imbalances between men and women have contributed to much of the observed HIV risk and subsequent spread of HIV in such regions as sub-Saharan Africa. 4 Demanding condom use from a boyfriend or husband is often not feasible for many women 5 –7 and can lead to partner violence, a phenomenon increasingly implicated in HIV infection. 8,9 Female-controlled methods of HIV prevention are, therefore, needed. 10,11
Topical microbicides are one alternative, but although studies have shown microbicide products to be acceptable to users, 12 –15 an efficacious product is yet to be found. Several authors point out the need for an effective oral chemoprophylaxis, also known as preexposure prophylaxis (PrEP), in the global fight against HIV/AIDS. 16,17
As with any product, oral methods of HIV prevention need to be acceptable to end users to be effective. Because oral chemoprophylaxis for HIV is still at an experimental stage, little is known about its acceptability. The closest analogies are adherence data from antiretroviral (ARV) therapy studies among HIV-infected people and postexposure prophylaxis (PEP) adherence studies. For ARV therapy, pooled adherence estimates range from 55% in North America to 77% in sub-Saharan Africa. 18 For individuals taking ARVs for PEP, two separate studies show therapy completion rates of 67% among healthcare workers 19 and of 78% in a group of patients with nonoccupational exposures. 20 It is difficult to compare these rates with those observed in the tenofovir disoproxil fumarate (TDF) study because ARV and PEP studies typically measure adherence by counting the proportion of people who fully complete their treatment regimen for a specified period of time. The analysis presented in this article used a different measure based on the average number of pills women reported taking in the past 7 days. Another difference between PEP and ARV therapy studies and PrEP pertains, respectively, to acuity of and motivation for adherence. PEP is for a short, defined period, and ARV therapy is generally associated with higher motivation than prevention, as the outcome of nonadherence is more certain (i.e., progression to AIDS and ultimately death).
Perhaps a closer analogy for PrEP, in terms of a daily oral product for prevention, is oral contraception. A study in Bangladesh with 1031 oral contraceptive users reported 13% of respondents took pills out of sequence and 17% left incorrect intervals between pill packs. Forty percent of the study respondents reported missing one active pill in the 6 months before the survey. 21 In a North American study, the percentage of cycles with perfect dosage was shown to be 79.2% (of 605 users) and increased significantly with age (p < 0.001). 22 This latter study, as well as others, 23 show greater comparative contraceptive efficacy and compliance for transdermal systems of delivery.
This article documents participants' behaviors and perspectives of taking a pill daily during a PrEP HIV-prevention trial. We examine pill acceptability over time and integrate qualitative and quantitative data to generate an understanding of participants' experiences taking the study pill. We describe pill adherence over time, as well as the social and contextual factors associated with use.
Additional information about TDF adherence levels calculated using pill count only can be found in Peterson et al. 24 Women in the TDF trial were instructed to bring back any unused pills at each of their monthly study visits. In the analysis by Peterson et al., the number of pills used was estimated by subtracting the number of pills returned from the number dispensed and dividing this by the total number of aggregated days women were enrolled in the study. Based on this calculation, the authors estimate that the pill was used for no more than 68% of all study days in Ghana.
Because we include in our analysis variables other than adherence measures, as well as qualitative data examining participants' perceptions and experiences beyond simple pill taking, we chose to use the term “acceptability” in our title. We recognize that others have defined the term more broadly, encompassing product use in a real life setting and in the context of alternative products, 25,26 but our analysis goes beyond simple adherence measures and includes several social and contextual factors typically found in acceptability analyses.
Context
The oral tenofovir trial was a randomized, double-blind, placebo-controlled study conducted between June 2004 and March 2006 in three African sites: Ibadan, Nigeria; Douala, Cameroon; and Tema, Ghana. 24 The Nigeria and Cameroon sites were closed either before the planned number of participants had been recruited or before all participants had the opportunity to complete all follow-up visits and interviews. 27 For this reason, data collected at those sites were not included in this analysis.
The trials were designed to assess the safety and efficacy of a 300-mg daily oral dose of TDF for prevention of HIV acquisition among women at high risk for HIV. Eligibility criteria for the study included being HIV negative, 18–35 years old, not being pregnant or breastfeeding, not desiring pregnancy during 12 months of study participation, and having an average of three or more coital acts per week and four or more different sexual partners per month.
To identify women at high risk for HIV, a formative research phase was conducted in the study sites before the clinical trial. The design of the formative research was adapted from the Prioritizing Local AIDS Control Efforts (PLACE) protocol, a method developed to find and prioritize areas for HIV prevention efforts within countries. 28 This formative phase included meetings with local HIV experts in each study country, participant observation in potential recruitment sites, and in-depth interviews and focus groups with stakeholder groups, including women from the potential clinical trial population. The goal of the formative phase was to find the most effective venues and methods for recruiting women into the study and to ensure culturally appropriate informed consent procedures for the clinical trial.
In Ghana, women were recruited from high transmission areas in Tema and its surrounds. Tema is a port city of roughly 200,000 people and is home to both fishing and manufacturing industries. The city has factories producing aluminum, refined petroleum, chemicals, food products, and building materials. According to the most recent estimates from 2004, Tema also had the highest HIV prevalence rate in the country (6.4%), more than double the national rate of 3.1%. 29 The formative research for the TDF trial identified 20 high transmission venues in the city of Tema and the neighboring community of Ashaiman. 30 The venues identified were composed of bars and nightclubs and were frequented regularly by female sex workers (who refer to themselves in Ghana as “sisters”) and men looking for sexual encounters. The majority of women enrolled in the TDF clinical trial were recruited from these venues, and many (the precise number is not known), therefore, were involved in some form of sex work.
Sex work in the Tema area takes three general forms. Some women combine sex work with transporting goods to and from the markets (known locally as “transporter girls”). This group tends to be younger and often composed of migrants from other regions of Ghana and other West African countries. Other sex workers, that is, “seaters,” are typically illiterate, middle-aged women from rural areas who accept clients at their homes. Many seaters engage in seasonal sex work to raise money for their children's school fees or other expenses and then return to their villages. The third group, “roamers”, are generally younger, more vulnerable women who travel from bar to bar seeking clients. 30 As of 1997, HIV prevalence among seaters and roamers had reached 74% and 27%, respectively. 31 All three types of sex workers can be found in the high transmission areas from which the clinical trial recruited participants.
Materials and Methods
At the Ghana site, 400 women were enrolled into the trial over a 6-month period, and study participation lasted 12 months. Data were collected monthly, and sample sizes used in our analysis for each month/visit varied (ranging from 312 to 200 women). After agreeing to participate in the study, potential participants were tested for HIV at a screening visit, again at their enrollment visit, and at each subsequent monthly visit. Women received pretest and posttest HIV counseling at all these visits. Eligible women were randomized into one of two arms—placebo pill or TDF pill—and were counseled to take one pill at the same time every day. All participants received a bottle of 30 pills, HIV risk-reduction counseling, free male condoms, and treatment for sexually transmitted infections (STIs) at each monthly clinic visit.
The Ghanaian portion of the study was approved by the Ghana Health Service Ethical Review Committee and, in the United States, by the Protection of Human Subjects Committee at Family Health International. Participants completed written informed consent for the trial at screening and enrollment. In-depth interview participants completed additional informed consent immediately before administration of the interview.
Participants were administered a structured questionnaire at screening, at enrollment, and at each monthly visit. In-depth interviews were also conducted with 24 women who were randomly selected from the larger clinical trial population between their 6 and 7 months visits. At least 3 women were interviewed for each month of the 6-month enrollment period to mitigate potential temporal biases. Qualitative interviewers were not affiliated with the clinical trial. A semistructured open-ended instrument was used for the in-depth interviews. Questions assessed participants' knowledge of TDF as well as the social and physical contexts surrounding pill use. Interviews were tape recorded, translated into English, and transcribed by field staff using a transcription protocol. 32 Thematic code book development followed a standardized process, 33 and code frequencies were generated in AnSWR. 34
Visit-level quantitative data were examined to determine how adherent women were to the pill taking regimen. In the monthly structured interview, participants were asked: In the last 7 days, how many days were you able to take the pill? This was the main adherence outcome variable for our analysis. Acceptability was further measured by asking women: How easy or difficult is it to remember to take the pill every day? In the last 30 days, did you have a problem taking the pills? For the latter question, participants were provided yes/no response categories, with a “specify problem” option for positive responses.
Women were supplied with 30 pills at their monthly follow-up visits. In some cases, women did not return for one or more follow-up clinic visits within a 30-day period, leaving them without pill access for at least a portion of the last 7 days. Also, data from the trial showed that some women failed to produce the pill bottle at a clinic visit or had more pills in their bottle than the number of days since their last visit (implying that they could not have taken a pill daily). As an alternative measure of acceptability, we were interested to determine if there were differences in adherence rates between women who had access to an entire monthly regimen of the pills and women who did not. A subset of “full access to pill” women was created. This group of women included only those who had full access to the study pill at any given visit (i.e., they had a sufficient supply of pills to take one each day between the current and previous study visit). Thus, individual women could move in and out of this subset depending on their pill access for any given month. The full access group was relatively heterogeneous over time. No women were in this group more than 8 of the 12 follow-up visits. The average number of times a woman was in the full access group was 1.79 times, and the median was 1 time. In other words, the full access group was not composed of a single cohort of women.
To measure participants' adherence over time, we looked at descriptive data for both the entire study population and those women with full access to the pill. An exploratory growth curve analysis (GCA) was conducted to examine the change in reported adherence over time. This analysis describes the different trends between the complete study group and the group with full access to the pill. The following participant trait covariates were also tested for their association with adherence over the course of the trial: age (dichotomized by median), education (dichotomized by median), marital status, ever had anal sex, ever given oral sex, condom used last sex, ever had STI, and ever used contraception. Although the measurement of adherence would have been complemented with additional information on the economic and emotional stability of the participants, such data were not collected in this study because of concerns about overburdening study participants.
To determine if adherence changed significantly from one visit to the next, we assessed the aggregate difference in adherence between each consecutive visit (i.e., between visit 1 vs. 2, 2 vs. 3, 3 vs. 4, and so on). Finally, to ascertain the relationship between reported problems with the pill and study attrition, we conducted a survival analysis, as well as a correlational analysis. All testing was two-sided, and all p values < 0.05 were considered significant.
Results
Participant characteristics
The mean age and level of education for participants were 23.7 and 7.1 years, respectively. Median age and education were 23 and 8 years, respectively. A small percentage of women (9.7%) reported living with a partner at enrollment. Less than 45% of the women reported previous use of contraceptives (including condoms) or using condoms during their last sexual act. More than 70% of participants had been pregnant previously, and about 44% reported ever having been diagnosed with an STI. Close to half of the sample (41%) reported ever performing oral sex on a man. Far fewer (17.7%) reported ever having practiced anal sex.
Pill adherence
The average aggregated self-reported rate of adherence was calculated for each visit. We present the trends in reported adherence across all visits both for the entire group and for the subset of women who had full access to the study pill at any given visit (Fig. 1). For this analysis, adherence was measured as the percentage of pills (out of a possible total of 7) that women reported taking in the last 7 days at a given monthly visit.
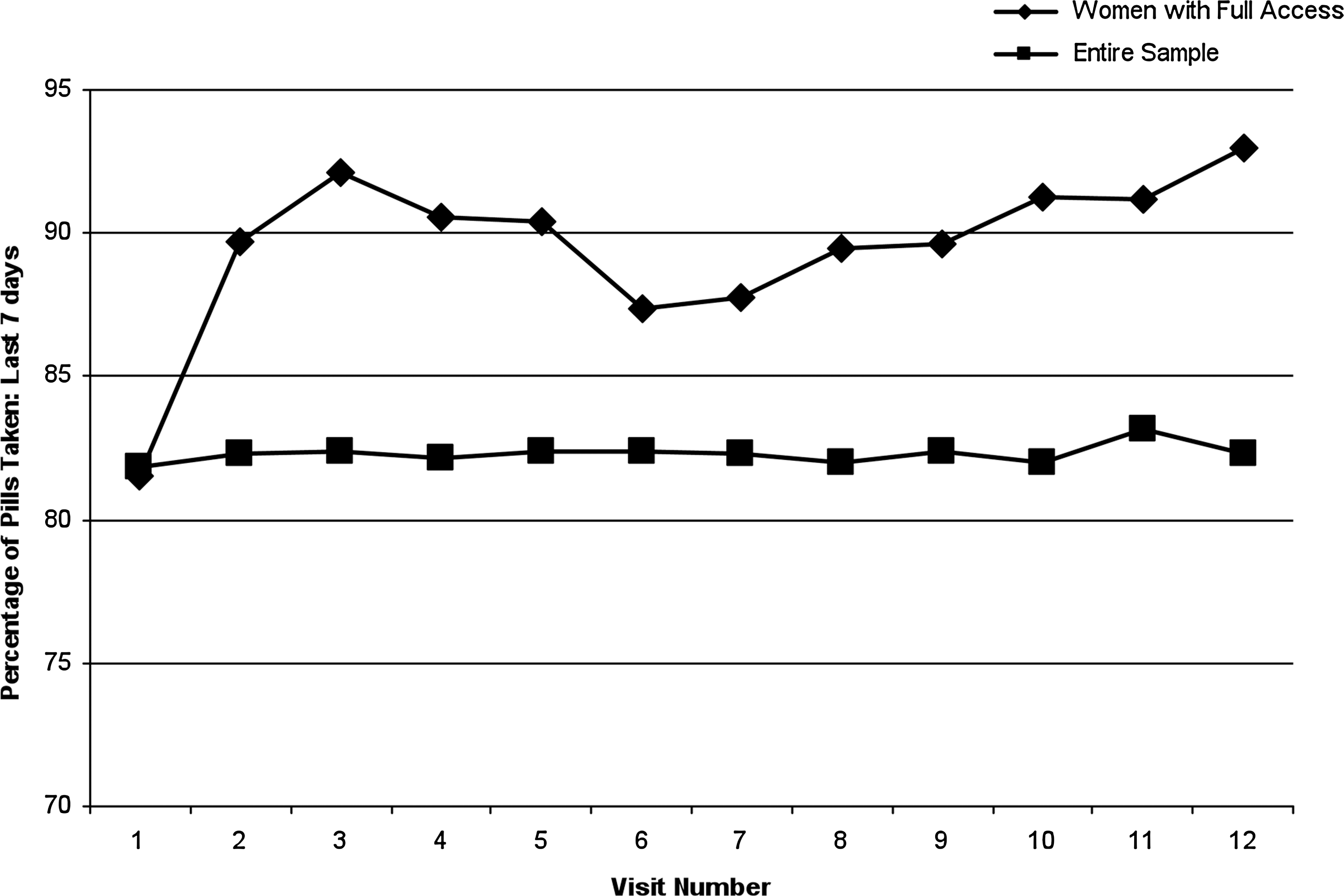
Self-reported adherence in the past 7 days: Entire sample vs. participants with full access to the pill.
The rate of adherence across visits for the entire study group was consistently >82%. Not surprisingly, adherence was greater for women with full access to the study pill, who had an average adherence rate of 88.4% (Fig. 1). GCA revealed that this change in adherence was significant over time (p < 0.01). (Note that GCA analysis describes the general change in adherence over time. It does not indicate in which direction or at which specific time points change occurs.) We tested the consecutive adherence between visits for the subset of women with full access and found that there were statistically significant changes in self-reported adherence between each month (p < 0.01) until after visit eight (note that although the differences between visits appear to be larger after visit eight than before, statistically this is not the case). As women left the trial (i.e., as attrition occurred), however, the sample size diminished each month, so this outcome may be a result of diminishing sample sizes.
The full access to pill dataset was also used for GCA comparisons that examined participant trait and assignment effects (placebo vs. TDF) on adherence rates over time. Our analysis shows that none of the participant traits tested were related to adherence. Data do show, however, that study assignment influenced adherence (p < 0.05) and that the two groups' rates of adherence changed differentially over time and diverge after visit six (p < 0.05) (Fig. 2).

Self-reported adherence in the past 7 days: Treatment vs. placebo.
Problems taking the pill
Clinical trial participants were asked to take one study pill at the same time each day. When asked about their ability to follow this study regimen across visits, 92.9% of the women reported in the structured interview that it was easy or somewhat easy. Overall, women reported few problems taking the pill. Less than a third (31%) of participants reported a problem with the pill at the month one visit in the structured questionnaire. This number decreased steadily until month six, where it leveled off near 4%. The most commonly reported problems with the pill (n = 284 total number of reported problems over the trial) were physical in nature (61%), such as gastrointestinal issues, fatigue, and dizziness. 24 Following this were forgetting to take the pill (20%), traveling (8%), and difficulty swallowing the pill (5%). Reported difficulties associated with remembering to take the pill dropped sharply after the first month in the trial, leveling off around the third month.
To see how reported problems were associated with study attrition, a survival analysis was carried out. Results from this analysis showed a marginally significant relationship between reported problems taking the pill and withdrawal from the study. Women who reported problems taking the pill were more likely to stay in the study than those who did not report problems (p = 0.06). We also conducted a bivariate correlational analysis to determine if reported problems with pill taking were associated with adherence (mean number of pills taken in the past 7 days). A significant negative correlation was identified (r = −0.23, p < 0.001), suggesting that women who reported problems took fewer pills than those who did not report a problem.
Supporting qualitative data
The qualitative data are congruent with our quantitative findings. When asked during in-depth interviews about how the drug, if it were to be found effective, may or may not benefit their community, participants were unanimously positive in their responses, saying that a preventive pill for HIV would benefit the health of their community significantly.
All 24 of the participants in the in-depth interviews said they took the pill every day, with only a few qualifying this statement by saying that on rare occasions they had forgotten to take it (often because of being intoxicated). Most of the women also reported having no problems taking the study pill. For those women who did mention having problems, almost all indicated that the problems were resolved in a relatively short amount of time. In fact, one of the most common themes that emerged from the in-depth interviews, and was espoused by 10 of the 24 women, was that taking the pill got easier over time. In contrast, no women said that a problem got worse or did not improve over time. The trend toward fewer problems, indicated in both the quantitative and qualitative data, appears to have occurred for several reasons. First, the physical effects tended to dissipate on their own over time. One woman recalled that, “Initially, I had bloated stomach. I reported it, and I was told it was nothing serious to worry about … and true to their [study clinician] word, it did stop.” (Participant 15)
Another woman described how the initial side effects decreased over time:
When I started taking the pill, I experienced some dizziness, but I was told about the side effects, so I was not bothered. I experienced it for some time and it stopped. I reported it to the doctor on my visit to the clinic, and he said it will soon stop. That experience didn't even last for 2 weeks. Now I don't experience any problem when I take the pill. (Participant 13)
In some cases, women developed behavioral strategies to cope with physical symptoms: “I normally take it at night because, sometimes, I feel dizzy when I take it. I can't take it during the daytime so I take it at midnight when I am about to sleep.” (Participant 22)
Problems associated with forgetting to take the pill were also overcome relatively quickly and easily. Women developed various strategies to help them remember. Some women, for example, used visual cues: “I have a wireless [radio], so I put it on top of the wireless, so as soon as I finish eating, and I enter the room and see it, then I take it.” (Participant 21) Others added the pill to an already established routine: “I always remember the time I take Secure [a brand of birth control pill]. I always take Secure at six o'clock in the evening, so if it's time, I easily remember this one [the study pill] too and take it.” (Participant 17) Still other women adapted pill-taking to fit their lifestyle: I took the pill every night when going to sleep, but now I have stopped taking it in the night. … I take it in the morning or afternoon because I might go out at night and get myself drunk and, perhaps, forget to take it … so I have decided to take it in the morning or afternoon. (Participant 24)
In the qualitative interviews, women did not report any problems with finding a suitable location to store or ingest the pill. The majority of women stored the pill in their handbag. Other reported storage places include drawers, shelves, and cosmetics baskets, and on top of appliances/furniture (to see and remember it) in participants' bedrooms.
Women in the in-depth interviews unanimously reported taking the pill at the same time everyday, usually with a meal. The time when women chose to take the pill, however, varied, typically in accordance with individual routines and circumstances. Most women report taking the pill while alone in their bedroom. Although privacy was not a commonly mentioned problem, a few women had to devise ways to ensure privacy, as described by one participant: I take it after having my bath, and normally there is no one there in the room and even if there is someone, I know how to take it so that no one sees me. Sometimes, if there is someone around I don't take the pill. … I normally go and buy food, and while washing my hand, I take the study pill. (Participant 19)
For some women, privacy was not an issue. Several of the 24 qualitative interview participants mentioned taking the pill in front of a boyfriend, a sister, or more commonly, friends who were also in the TDF study. A couple of participants even expressed a rather nonchalant attitude about privacy, as exemplified in the following quote: “I don't care who is around. … I just go for water and take it.” (Participant 04)
Although the behavior of taking the pill was generally a private act, most women discussed the study itself with others at some point during the trial. Data from the structured interviews show that over the course of the trial, 68% of the study participants had talked to at least one person (outside of study staff ) about the study. Across all 12 visits, 63% of the women reported speaking at least once with friends (who were sometimes in the study as well), siblings/sisters (17%), husbands and boyfriends (5%), casual sex partners (5%), and parents (2%). The qualitative data indicate that discussions largely centered on what women learned about HIV prevention, the study procedures, and perceived benefits (e.g., medical care) of being in the clinical trial. In many of these cases, participants were describing the study to their friends in the context of attempting to recruit them to the study.
Discussion
The data indicate that taking a daily pill for HIV prevention among women in an HIV prevention trial in Ghana was not problematic. Because of the study design and the travel demands and other logistical constraints of study participants, however, not all women had complete access to pills during the study. When women did have full access to the study pill, they reported higher levels of adherence. Based on this finding, it would be prudent for future similar studies and interventions to develop more effective procedures to ensure that these kinds of barriers are addressed so that participants/clients have consistent access to the product.
Related to the travel and logistical issues is the apparent discrepancy that exists between the self-reported adherence rate in this analysis and the adherence rate based on pill counts and reported in a previous TDF study analysis. 24 In the analysis presented here, average self-reported adherence in the past 7 days never went below 82% for the entire sample. In the analysis by Peterson et al., 24 however, the adherence rate in Ghana, based on pill counts, was at most 68% of all study days. This observed difference can be explained by the methods used in calculating adherence. For the Peterson et al. analysis, the total number of study days used in the denominator included some days that comprised gaps in study attendance. For example, if a woman went to her first four visits, missed three, and then completed her final five visits, the denominator in the adherence equation would have been calculated at 365 days. For the analysis presented in this article, the same woman would be included in the sample only for the 9 months that she attended the clinic and completed a questionnaire. In short, the larger denominator used by Peterson et al. encompasses adherence to the monthly study follow-up visit schedule as well as adherence to the daily pill regimen, whereas the analysis presented here focuses on adherence to the daily pill regimen.
Our analysis also included acceptability measures other than adherence, such as ease of use. The majority of women reported that taking the pill at the same time daily and according to the study regimen was easy. Problems that did arise tended to take care of themselves in the first 6 months. Most problems, such as physical symptoms, dissipated on their own. Other issues, such as forgetting to take the pill, were mitigated through behavioral strategies developed by participants. These data suggest that any future interventions should provide participants/recipients enough time to adapt to the product and include this forethought in the design of future studies and other interventions.
On the surface, it may appear that there is discordance between the quantitative and qualitative data with respect to pill taking. Quantitative trends for the entire sample do not show significant increases in adherence over time, whereas qualitative interviews indicate that pill taking got easier as the study progressed. However, adherence among the full access group was greater at every subsequent time point from baseline (month one), which may be what is reflected in the qualitative data. Further, only 24 women were administered qualitative interviews after their sixth visit. Although they were systematically sampled, the small sample size, comprising only 6% of the population, may not have captured the full extent of women's experiences taking the pill.
When examining the relationship between reported problems taking the pill and study attrition rates, results indicate that those women who reported problems were more likely to stay in the study. This may be related to the counseling efforts of the staff and their ability to discuss problems experienced by participants during study visits. It may also reflect enhanced motivation to stay in the trial for the high-quality medical care (to deal with the physical symptoms), or it could be that some women who experienced problems did not report them to study staff but instead discontinued the trial. The attrition effect observed warrants further investigation.
A difference in adherence was observed between the treatment and placebo groups. It is possible that this may be a result of cumulative physical side effects of the drug that were not reported by the women in the trial, especially after month six, when the two curves begin to diverge. It may also be that women in the treatment group reduced pill use in order to reduce side effects and, therefore, did not report side effects because they were mitigated by reduced adherence. This interpretation must be tempered with counterevident findings from a previous analysis for the TDF study and presented in another article, 24 which showed no significant differences in reported adverse events between the placebo and treatment groups. The complicated relationship among experiences with the study product, self-reported behavior, and study attrition should be examined in more detail in future studies of this kind.
Although the findings we report are promising, we acknowledge that the social and environmental context of a clinical trial is different from what would be expected outside such a setting. Our findings must, therefore, be tempered with this fact. A clinical trial provides participants with a supportive environment not typically found in regular life. Monthly (and free) medical examinations and counseling, reimbursement for time and effort to attend the clinic, access to product at no cost, and relationships developed between participants and study staff over the course of the study can all affect adherence. Likewise, the knowledge that half of the participants receive placebo combined with the unknown efficacy of the drug for HIV prevention may influence adherence. The best way to measure adherence in a more natural context is to do a phase IV study after efficacy has been demonstrated. Alternatively, smaller acceptability studies, with no biological outcome, could be conducted that closely follow adherence. Such studies could include using multiple measures to assess adherence (e.g., diaries, survey with various indicators, as well as some of the more innovative methods) and look at the social and contextual factors associated with pill use in more depth.
Given the relatively better compliance and efficacy demonstrated with transdermal delivery of oral contraception noted in the beginning of this article, it would also be interesting to determine the feasibility, pharmaceutically and behaviorally, of administering HIV chemoprophylaxis transdermally.
As the results of this study demonstrate, collecting data earlier in the process, albeit in a less natural context, can inform product rollout and development of product-related interventions. More could be learned in forthcoming studies, however. Future efficacy studies would be advised to develop better methods for documenting some of the social and structural factors that might be associated with adherence, such as social relationships, travel constraints, and other potential barriers, and incorporate them into the clinical trial protocol in the early stages of the research. As Tolley and Severy 35 observe, incorporating social/behavioral research into clinical trials early in the study design can acquire valuable information pertaining to product use and acceptability.
Conclusions
Women in the trial reported a high degree of adherence, particularly when they had full access to the pill. Women in the TDF study in Ghana easily adapted to a new routine of daily pill taking and incorporated the new behavior into their daily lives with minimal effort. If PrEP for HIV is found to be biologically efficacious and has as few physical side effects as seen in the TDF PrEP trial, our data suggest that taking a daily pill for HIV prevention within this type of population is feasible. The results presented here are not conclusive, however, and improved measures of adherence in future trials should be developed to more fully address the relationship among adherence, safety, and effectiveness. Examples of some possible techniques include electronic monitoring of pill packages, blood tests measuring serum levels of drug, and using less personal methods of data collection (such as audio computer assisted self interview (ACASI)) to minimize social desirability bias in self-reporting. Having participants keep diaries might also provide more insight into pill taking behavior. Such measures will pave the way for improved PrEP intervention planning, monitoring, and evaluation.
Footnotes
Acknowledgments
Support for this work was provided by the Bill and Melinda Gates Foundation (Oral Tenofovir for HIV Prevention, grant 19789). The contents of this publication do not necessarily reflect the views or policies of or imply endorsement by the financial supporter.
Disclosure Statement
The authors have no conflicts of interest to report.