
Abstract
A consortium of investigator-thought leaders was convened at the Heart Institute at Cedars-Sinai Medical Center and produced the following summary points:
Introduction
Drs. Saralyn Mark and C. Noel Bairey Merz
Cardiovascular disease (CVD) is the leading killer of both women and men. Sex differences in CVD outcomes exist, yet knowledge of the mechanisms underlying sex differences in CVD, ranging from basic science inquiry to pathophysiological understanding, diagnostics, and therapeutics, is limited. A symposium of thought leaders was convened at Cedars-Sinai Medical Center to address this issue with the following three objectives: (1) to determine the current understanding of sex differences in CVD, (2) to identify important knowledge gaps in sex differences in CVD and prioritize future research areas, and (3) to identify challenges and barriers to the inclusion of evaluation of sex differences investigation in CVD.
The Institute of Medicine (IOM) in 2001 published a monograph, “Exploring Biological Contributions to Human Health: Does Sex Matter?” 1 The IOM report came up with three conclusions: (1) sex does matter and should be considered when designing and analyzing studies in all areas of health-related research, (2) the study of sex differences has been predominantly observational research, and the next step is study of mechanisms and therapies related to sex differences when present, and (3) barriers to the advancement of knowledge about sex differences in health and illness must be eliminated.
To understand sex differences research, a discussion of terminology is needed. The term “sex” refers to the biological sexual differentiation (e.g., women have ovaries, and men have testes). The term “gender” refers to the sociocultural attributes of that biological sex (e.g., women have complex social networks, and men have wives). The term “sex genotype” refers to the XX and XY chromosomes. “Sex phenotype” refers to the phenotypic expression of the genotype (e.g., ovarian development in females and testicular development in males). Phenotypic expression may vary with development and age (e.g., premenopausal women have higher estrogen levels because of ovulation compared with postmenopausal women, who do not ovulate). Both remain XX genotype but differ in phenotypic expression.
Examples of sex differences are evident in a wide variety of biomedical areas. Women have greater high-frequency nonauditory brainwave patterns when tested compared with men, whereas homosexual men are intermediate between women and heterosexual men, suggesting that this may be genotypic. 2 Women have lower thermal pain thresholds than men, which appear to be mediated by estrogen levels, suggesting that this sex difference is phenotypic. 3 Women are evaluated less often than men by physicians in response to chest discomfort, suggesting cultural sexism bias. 4
Thought leaders and representatives from the Organization for the Study of Sex Differences (OSSD), the American College of Cardiology (ACC), the American Heart Association (AHA), and the National Heart, Lung and Blood Institute (NHLBI) participated. This symposium is timely because women do not appear to be benefiting optimally from current CVD strategies. Although overall CVD has declined by 52% in men and 49% in women, more women now die annually from CVD than men, and there is an actual increase in mortality in younger middle-aged women. 5 The symposium attendees are listed in the Appendix.
Sex Differences in CVD Prevalence and Risk Factors
Dr. Leslee J. Shaw
There is a delay in the onset of CVD in women that is generally about 10 years beyond that of their male counterparts. 6 Hypoestrogenemia and hyperandrogen states can alter the prevalence and clustering of cardiac risk factors as well as cause a heightened risk of CVD at a younger age. 7 –9 Attention to sex-specific issues related to CVD has contributed to recent declines in disease-specific mortality, as reported from the CDC's National Center for Health Statistics noting 10,000 fewer annual deaths in women since 2000 (a 10% reduction) (Fig. 1). 10
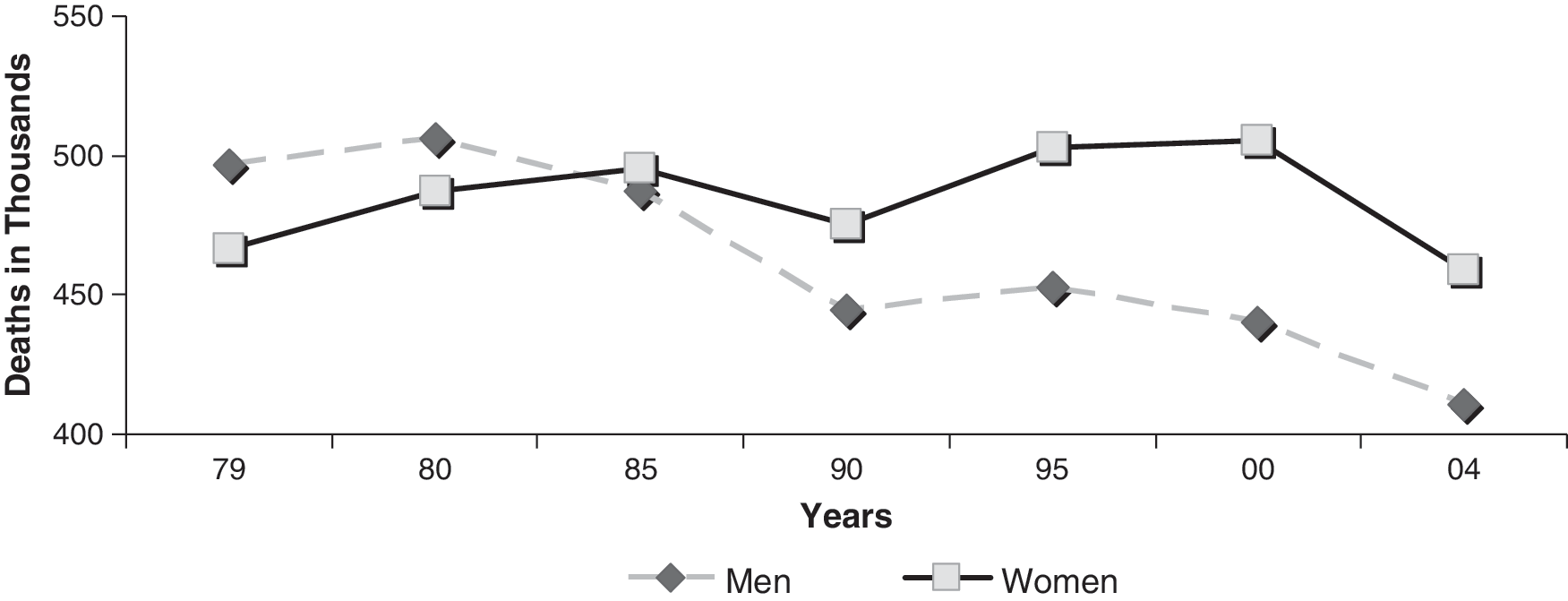
Cardiovascular Disease (CVD) mortality trends in women and men. CVD disease mortality trends, U.S. 1979–2004. Source: NCHS and NHLBI (2008).
Sex-based differences in the prevalence, clustering, and outcomes of cardiac risk factors support a unique profile that accentuates long-term risk. For women, both hypertriglyceridemia and diabetes are associated with relatively worse CVD outcomes compared with men. 6 CVD risk factors in women increase at the time of menopause, including weight gain, a mild decline in high-density lipoprotein cholesterol (HDL-C), and a rising prevalence of hypertension.
C-reactive protein (CRP) is a novel inflammatory marker that is more often elevated in women than in men 11 and may contribute to this differing plaque pathophysiology. 12 The Women's Ischemia Syndrome Evaluation (WISE) investigators and others have hypothesized that the combination of prolonged exposure to atherogenic risk factors, sex-specific proinflammatory status that includes autoimmune disease, reproductive hormonal status, positive arterial remodeling, and microvascular dysfunction leads to a more complicated course for women with established CVD compared with men. 6,13,14
Reproductive hormones also appear to be involved in CVD risk in women. Low estrogen levels due to dysruption of ovulatory cycling in premenopausal women are associated with greater obstructive coronary artery disease (CAD). 7 We have also evaluated hormonal alterations associated with polycystic ovary syndrome (PCOS), which is a risk factor for type 2 diabetes mellitus (DM) and the metabolic syndrome, which includes hyperlipidemia, central obesity, and hyperglycemia. Women who fit a PCOS phenotype that includes elevated androgen levels have elevated CVD risk in the postmenopausal period. 8 This work suggests that imbalance in endogenous sex hormones in women accelerates CVD risk.
Sex differences in direct markers of subclinical atherosclerosis, such as coronary artery calcification (CAC), also have been reported. 15,16 In a report on mortality differences by sex in 10,377 asymptomatic individuals referred for evaluation of CVD risk, 16 a higher mortality risk existed in the setting of CAC for women compared with men. In a related report, Bellasi et al. noted a higher mortality risk for women with CAC who had three or more risk factors. 15,16 Both reports support the degree to which comorbidity and clustered risk factors potentiate the atherosclerotic disease process and heighten risk in women as compared with men.
Among symptomatic patients, women have less obstructive angiographic CAD than men. In a recent multinational analysis, the prevalence of angina is greater in women as compared with men up to age 75 years, 17 supporting prior reports that CVD presentation and risk vary by age. Despite the less frequent obstructive CAD, 18 a nationwide registry of 835,827 patients, which included 459,941 acute coronary syndrome (ACS) patients, reported a consistently higher in-hospital mortality for stable chest pain and ACS for women than for men. 19 In a recent pooled analysis of data from several ACS trials, patients at highest risk included those with mild coronary disease compared with completely normal arteries 20 ; younger women in particular had higher hospital mortality compared with younger men, despite less obstructive CAD. 21 Many women with nonobstructive CAD have persistent symptoms, with nearly half complaining of chest pain through 5 years of follow-up, 22 and nearly 1 in 5 requiring hospitalization for refractory or worsening angina. Evidence of ischemia accelerates the risk for symptomatic women of all ages, 23 and symptoms with even mild CAD elevate the risk in women. 24 The limited understanding of the mechanisms of sex differences in CVD places women at elevated risk. 25
Sex Differences in Atherosclerosis and Response to Intimal Injury
Dr. Prediman K. Shah
Glagov et al. 26 observed that arteries undergo positive remodeling by enlarging outward in order to accommodate plaque and avoid luminal compromise. Proteases produced by inflammatory cells appear to have a role in adventitial remodeling through extracellular matrix (ECM) destruction, 27 suggesting that the inflammatory processes are relevant in outward remodeling. Women appear to have more diffuse atherosclerosis, less luminal stenosis, higher incidence of endothelial dysfunction, and a higher prevalence of microvascular dysfunction than men, 6,13 suggesting that women may have greater positive remodeling.
The pathoanatomic substrate for coronary thrombosis also differs between men and women. In men, 80% of coronary thrombi tend to occur because of plaque rupture, whereas in women, 20%–40% of coronary thrombi occur on an intact atherosclerotic plaque with superficial atherointimal erosion (Fig. 2). 12,28 This plaque erosion is a common finding in sudden cardiac death (SCD) in younger women who were smokers and postmenopausal women taking hormone replacement therapy (HRT).

Sex differences in atherosclerotic plaque disruption. Reprinted with permission from Burke et al. Circulation 1998;97:2110–2116. 12
Plaques that tend to rupture typically have a lipid-laden atherosclerotic core with intimal and adventitial inflammation and increased plaque neovascularity. 27 Inflammatory cells trigger death of smooth muscle cells through apoptosis and produce matrix-degrading enzymes that can induce depletion of the collagen framework, leading to loss of collagen and thinning of the fibrous cap 27 and, eventually, either rupture or erosion. Importantly, lipid-laden plaques have inflammatory cell-derived tissue factor (TF) that is a prototypical trigger for activating the clotting cascade. When a lipid-rich plaque ruptures, TF is immediately exposed to circulating blood, which, with other factors, stimulates the production of thrombin. This in turn leads to platelet-fibrin thrombus formation. 27
The mechanisms of sex differences in this process are not well understood. Enhanced endothelial apoptosis is associated with exposure of TF on the luminal side of the coronary artery. A higher prevalence of superficial endothelial erosions is associated with increased sex-specific circulating coagulability. 29,30 Also, systemic inflammatory processes increase anticardiolipin antibodies, which are more prevalent in women. TF that may be originating not from the plaque but from the circulation 31 may also create a prothrombotic state. Normally, TF remains contained within circulating leukocytes and is not available to trigger thrombosis. Under certain conditions, however circulating leukocytes can shed membrane microparticles, which have been shown by electron microscopy to be laden with TF. 31
Spontaneous coronary artery dissection is a rare clinical syndrome that is more prevalent in women than men. In fact, 80% of cases occur in women, particularly in premenopausal women, often in the peripartum setting. 32 The clinical presentation frequently is SCD and, less commonly, unstable angina, acute myocardial infarction (MI), heart failure, or shock. Reproductive hormones may contribute to this, in that matrix metalloproteinases may be induced by hormonal alterations and may promote intimal disruption and dissection; however, this has not been specifically studied.
The Tako-Tsubo syndrome, also known as stress-induced cardiomyopathy, 33,34 is also more prevalent in women, especially in older postmenopausal women. These patients have findings of an ACS, often triggered by emotional or surgical stress. Patients can be in shock, and ventricular function assessment frequently shows ballooning of the left ventricular (LV) apex and preserved or vigorous contraction of the base with no obstructive CAD, low to modest cardiac enzyme elevation, and LV recovery in 4–8 weeks. 33,34 Previously considered a rare syndrome, it appears to account for 2%–5% of patients with a clinical picture of an ACS. 33 The pathophysiology of the Tako-Tsubo syndrome has been hypothesized to be an outcome of (1) transient LV stunning induced by a sudden surge of catecholamines, (2) coronary spasm or microvascular dysfunction, and (3) coronary thrombosis followed by rapid spontaneous recanalization. Furthermore, it has more recently been hypothesized that Tako-Tsubo syndrome represents a form of myocardial stunning that differs mechanistically from postischemic stunning. 35
Inspection of the mechanisms involved in atherosclerosis and intimal response to injury, including arterial remodeling, plaque composition, destabilization, and thrombosis, as well as arterial dissection and microvascular dysfunction, contributes to understanding of the observed sex differences in CVD. 13 Atherosclerosis is qualitatively and quantitatively different in women and men; women demonstrate more plaque erosion and more diffuse plaque with less focal artery lumen intrusion. Investigation into these areas aimed at more fully understanding sex-specific mechanisms should be targeted in order to develop tailored therapies.
Sex Difference in Bone and Vascular Cellular and Tissue Engineering
Dr. Barbara D. Boyan
The study of bone tissue provides an example of sex based-differences in mechanism for CVD investigators to emulate. Sex differences in properties of bone are established in utero due to sex traits that are inherited differently in males and females and relate to vascular cellular and tissue engineering. A family of proteins called small integrin-binding N-linked glycoprotein (SIBLING) that regulate cell migration and cell attachment is encoded on the X chromosome, such that when there is a genetic change in one of these molecules, it is experienced to a greater extent in males. 36 Studies examining the response of male and female cartilage cells to estrogen show that although both sexes have receptors for estrogen, some of the estrogen actions are seen only in females. 37 In contrast, although both female and male cells have testosterone receptors, male cartilage cells exhibit responses to testosterone that are not observed in female cells. 38 Cartilage cells and bone cells make their own estrogen and their own testosterone, although this is regulated differently in the two cell types. 39,40
Huard's group 41 has demonstrated that muscle-derived, mesenchymal stem cells (MSCs) from females engraft easily into female recipients and less well into males. Male cells were even less effective in engrafting into females, and the least effective engraftment of muscle-derived MSCs is male cells into males. 41 These results suggest important sex differences in stem cells that are more than a simple male-female difference.
Bone is a tissue that is constantly remodeling, including its vascular blood supply. Studies indicate that osteoblasts are sensitive to the physical and chemical properties of the bone surface. 42 We have taken advantage of a cell culture model in which osteoblasts are grown on well-controlled titanium (Ti) substrates with specific microstructural elements. In response to estradiol, female cells produce large amounts of Transforming growth factor-β (TGF-β) on that surface compared with male cells, 43 which do not respond to estrogen exposure (Olivares-Navarrete et al., unpublished observations). This has potential important implications for attempts to resurface vascular stents, where endothelial response to the material surface and subsequent reendothelialization are a major concern.
Studies using ablation of a rat tibial bone marrow model demonstrate initiation of a sequence of events that includes formation of a hematoma within the marrow cavity (days 1–3), stimulation of rapid bone formation throughout the marrow cavity with onset of mineralization at day 6, osteoclast resorption of the newly formed bone at day 21, and restoration of marrow by day 28. Results from these studies show that when biomaterials are implanted in the marrow cavity, endosteal bone formation is affected, the restoration of the marrow is affected, and a material-specific systemic response occurs as well. Interestingly, distribution of the vascular imaging agent Technetium-99 methylene diphosphate (99Tc-MDP) is also affected by the presence of the biomaterial. 44 Growth of cells on Ti substrates with different microstructures and chemistry affects the release of angiogenic factors including vascular endothelial growth factor-A (VEGF-A), endothelial growth factor (EGF), and fibroblast growth factor-2 (FGF-2) (Raines et al., unpublished observations). Surfaces that are highly effective in promoting bone formation are also more vasculogenic, and this correlates with the differentiation of the osteoblasts. Accordingly, the growth factor cocktail that is produced by these cells on the highly osteogenic surface is in fact also highly vasculogenic. Whether this is also sex-specific is of great interest, particularly when using materials as implants in osteoporotic bone 45 or to ensure new blood vessel growth for tissue vascular supply. 46
Understanding sex differences in tissue development could have widespread implications for a variety of CVD therapies, with relevance to local micromaterials and tissue vascular supply important to device development. CVD strategies that include devices should explore differing anatomic shapes and surfaces as well as differing drug coating and eluting strategies.
Progenitor Cell and Cytokine Regulation of Cardiovascular Tissue: Implications for Repair/Restenosis
Dr. Doris Taylor
Cell-based cardiovascular repair is not only feasible but likely because virtually every organ in the body either contains tissue-specific progenitor cells (PCs) or is linked to a reservoir of cells in bone marrow that are mobilized and migrate into tissues when needed. 47 –55 Chronic disease and aging are associated with a reduced number and functional capacity of PCs. 56 –60 We believe that a major role of inflammation in the setting of chronic disease or acute injury is to recruit appropriate reparative PCs to the injury site and start an endogenous repair process. Further, if appropriate cells reach the site of injury and either deliver a small molecule (e.g., cytokine) or physically integrate, the inflammatory response decreases. 51 –55 In the absence of sufficient cell numbers or recruitment for repair, however, there is a deleterious positive feedback loop (e.g., increased inflammation) that occurs. This is characterized by a stronger proinflammatory T helper (Th)-1-type cytokine (tumor necrosis factor-α [TNF-α] and interleukin-12 [IL-12) response, and recruitment of proinflammatory cells to the injury site. 61
In preclinical models, there are sex differences in this system of repair in response to atherosclerotic disease, 62 including differences in the composition of bone marrow and responses to treatment with bone marrow-derived cells, which are reflected in differences in serum cytokines and the repair milieu. 57 For example, although bone marrow-derived CD34-positive cells (associated with vasculogenesis) decrease with age in both males and females, there are sex differences in the decrease that inversely correlate with progression of atherosclerotic disease. 52,57,63 Another cell population, vascular progenitor or CD31(+)/CD45 (low) cells, also linearly decreases with age and strongly predicts the onset of atherosclerosis 62 in females moreso than in males, suggesting that this may be a potential diagnostic marker in women. Finally, cells that are most often described as endothelial PCs (AC133(+)/CD34(+)) increase mildly at the onset of atherosclerosis and then decline, at which point atherosclerosis accelerates, 57 suggesting an imbalance between injury and repair, although further study is needed to determine if these are causally related.
These data support the hypothesis that a cell number-mediated threshold for vascular repair exists below which repair does not occur and that the threshold is increased by stress, age, or ongoing disease. 52 To test this, we delivered bone marrow cells from young mice to aging animals intravenously and demonstrated a dramatic reduction in plaque burden over time in the treated animals 52 despite no effect on serum lipids. Instead, the delivered cells differentiated into endothelial cells at the level of the atherosclerotic lesion 52 and appeared to decrease plasma markers of inflammation, including IL-6.
To determine if sex was also an important component of vascular repair, we gave male and female animals with severe atherosclerotic plaque four doses of bone marrow mononuclear cells (BMNC), once every 2 weeks, after which we assessed the plaque burden response. 57 Two observations were noteworthy between females and male animals. Females demonstrated a significantly greater increase in vascular PCs and endothelial PCs in the bone marrow compared with males, and males had a greater increase in inflammatory (CD45(+)) cells compared with females. Among the treated males and females, female cell administration decreased plaque burden in males to a much greater degree than male cell administration to males, and female cells administration to females did not perform as well (Fig. 3). Male cells administered to males or females demonstrated no improvement 62,63 and trended toward a worsening of plaque burden in females. Notably, the male recipients had low endogenous bone marrow endothelial PC numbers with a high plaque burden, and both male and female BMNC administration increased the bone marrow endothelial PC number, but only the female cell administration decreased plaque burden. Conversely, female recipients had high endogenous bone marrow endothelial cells, and administration of BMNC did not impact plaque burden, indicating that the mechanism of plaque deposition involves cells beyond endothelial PCs.
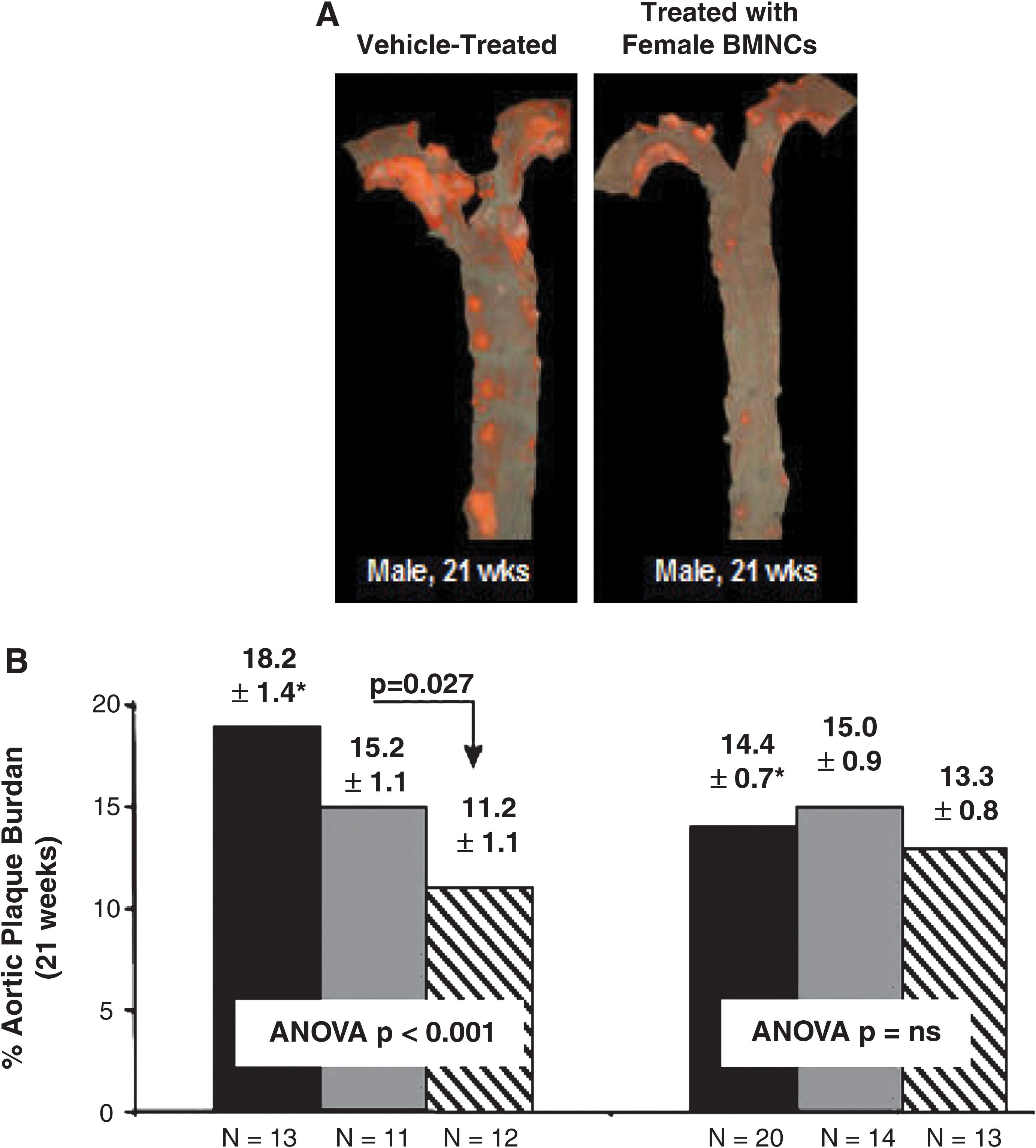
Female progenitor cells (PCs) are more beneficial for atherosclerotic plaque burden. Sex-dependent attenuation of plaque growth after treatment with bone marrow mononuclear cells (BMNCs). Reprinted with permission from Nelson et al. Circulation Research 2007;101:1319–1327. 62
To gain insights into mechanism, we also quantified serum cytokines in the male and female animals and found that the administered cells carry their sex phenotype into the recipient. The greatest predictors of the atherosclerosis plaque outcome were the regulatory cytokine IL-15 and the cell mobilizing agent granulocyte colony-stimulating factor (GCSF).
In summary, inflammation is a key mediator of endogenous repair and a critical target to maximizing cell and gene therapy. The balance between proinflammatory and anti-inflammatory responses differs between males and females, and this is exacerbated with age. Bone marrow PCs express both proinflammatory (Th-1) and anti-inflammatory (Th-2) cytokines, and this expression differs by sex. When a proinflammatory response is greater than an anti-inflammatory response, endogenous PCs associated with injury are recruited.
Understanding the PC differences in women and men with regard to endogenous repair, including genomic analyses, should be pursued. Bone marrow PCs engraft differently based on the sex of the donor cell and the sex of the recipient. PC therapeutic studies need to consider the sex of cells of the source and the recipient.
Sex Differences in Medication Response and Pharmacogenetics
Dr. C. Noel Bairey Merz
The majority of medications that are withdrawn following Food and Drug Administration (FDA) approval are withdrawn because of unanticipated adverse effects in women. 64,65 Women are consistently underrepresented in cardiovascular clinical trial enrollment, 66 resulting in an inability to document intervention efficacy in women or to evaluate post hoc sex differences. The NHLBI has mandated female-only studies, such as the WISE, 67 yet CVD medication and device intervention trials remain a problem. What do we know about medication response and pharmacogenetics in women? What sex differences have been described? What gaps exist in the fund of knowledge?
Large secondary prevention studies of aspirin that included both sexes demonstrate equal efficacy in women and men for prevention of recurrent CVD. 68 A meta-analysis of the primary prevention aspirin studies that included women and men suggests no difference in response to aspirin, although insufficient numbers of women were randomized in these studies to independently test efficacy. 69 Comparison of the all-female low-dose aspirin trial and the all-male Physician's Health Study provides an interesting paradox that alludes to a sex difference with regard to aspirin and CVD. 70 Among women, low-dose aspirin did not prevent first heart attack yet prevented first stroke, whereas, conversely, aspirin prevented first heart attack but not first stroke in men (Fig. 4). The studies documented aspirin efficacy at the trial doses used in terms of impact on platelets; thus, it does not seem likely that this sex difference is due to differences in weight-adjusted dosing or pharmacological effect.
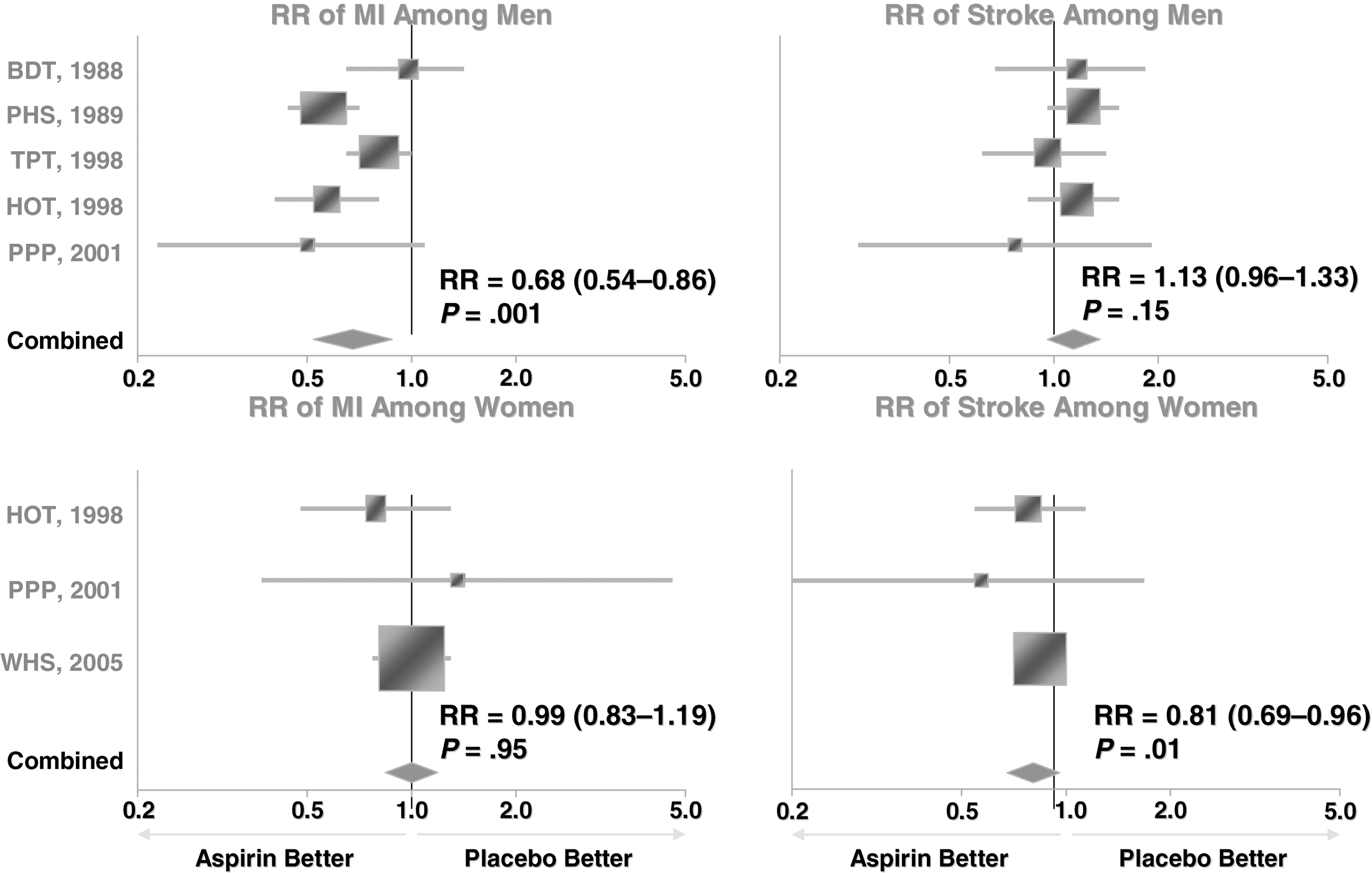
Sex differences in aspirin therapy for CVD prevention. Reprinted with permission from Redberg et al. N Engl J Med 2005;352:1293–1304. 70
This observed sex difference in aspirin medication trials calls for a reexamination of observational CVD datasets for potential explanations. Observational data demonstrate that a relatively higher percentage of CVD events in women is attributable to stroke compared with a relatively higher percentage of CVD events attributable to MI in men, suggesting that aspirin efficacy may vary according to sex differences in the pathophysiology of CVD. The size of blood vessels involved in the pathobiology of stroke (dominantly microvasculature) vs. MI (dominantly macrovasculature) suggests the hypothesis that microvascular CVD involvement may be preferentially more important in women. Future clinical trials must stratify results by sex and enroll a sufficient number of women to test efficacy and safety in both sexes.
Evaluation of secondary prevention trials of statins, cholesterol-lowering medications, similarly demonstrates that statins appear to work equally effectively in women and men with established CVD. 71 The recent large primary prevention JUPITER trial, which identified subjects without evident CVD risk but with elevated high sensitivity (hs) CRP, demonstrated a robust cardiac event reduction with statin lipid-lowering therapy in women. 72 Additional clinical trials should be performed in appropriate at-risk women with this class of medication that clearly prevents CVD, which kills more young women than does breast cancer. 73
Similar limitations in sex-specific clinical trial data are evident with regard to beta-blockers, 74,75 antiarrhythmics such as amiodarone, 76 –79 and internal cardiac defibrillator (ICD) devices, 80 demonstrating confidence intervals (CIs) among the female subgroups that are substantially wider than those of the men because of the relatively smaller sample size, resulting in insufficient statistical power to test efficacy in women. A reasonable conclusion to draw after examination of the existing datasets of clinical trials of CVD therapies in women is that of the pedestal effect, whereby women are neither tested nor treated because they are special.
Are there reasons to believe that sex differences in medication response might be real? A leading question addressed by the WISE study was to understand the pathophysiology of women with the triad of persistent symptoms, nonobstructive coronary arteries, and evidence of ischemia or MI by objective measures, such as stress testing or troponin levels, a condition dominantly observed in women. Indeed, women men are two to three times more likely than men to have an ACS or MI with open coronary arteries, 81 suggestive of an important sex difference. The WISE study demonstrated that a sizable proportion of these women have microvascular coronary dysfunction 82 that correlates with persistent chest symptoms 83 and is associated with an adverse CVD prognosis. 84 Using an estimate of a 65% prevalence of persistent symptoms from the WISE and other studies 83 in the women enrolled in a national coronary angiography database with normal or nonobstructive coronary arteries, there are a projected 90,000 new cases annually and as many as 2–3 million women in the United States with this condition. 7 Contrast this with the 6 million women in the United States living with obstructive CAD, and we gain an appreciation of the magnitude of this CVD problem in women not previously recognized.
These data in women further suggest the hypothesis that sex differences in CVD pathophysiology relative to microvascular and macrovascular dysfunction may contribute to our understanding of sex differences in response to medication. Review of the literature suggests that women have a greater vasoreactive state compared with men, 85 and little is known about possible underlying genetic contributors to this sex difference. Pepine et al. 85 have demonstrated that coronary endothelial function testing in response to acetylcholine varies according to a polymorphism at position 573 in angiotensin receptor type 1 (AT1R) in the WISE women regardless of the presence of absence of obstructive CAD. 86 This finding supports a genetic component to coronary endothelial dysfunction in women; comparative research in men is needed to identify the putative sex difference. Further investigation in this area will evaluate whether this type of genetic information can help identify patient response to medication, specifically interventions aimed at the renin-angiotensin-aldosterone system (RAAS), which modulates endothelial dysfunction, such as an angiotensin converting enzyme (ACE) or angiotensin renin blocker (ARB) or aldosterone blocker medication.
Future investigation should be aimed at exploring mechanisms of sex differences to provide a platform for optimization of sex-specific therapies, if appropriate, through incorporating genomics and pharmacogenomics. Because women and men can have differences in pharmacological responses, sex-specific pharmacogenomics should be included in pharmacological development.
Sex Differences in Thrombosis and Current Thrombolytic Strategy Response: Implications for New Local Delivery Development
Dr. Alice K. Jacobs
The importance of including women in clinical trials and of reporting sex-specific data cannot be overemphasized. Within the NHLBI percutaneous transluminal coronary angioplasty (PTCA) and Dynamic Registries, enrollment of Caucasian men was capped with each wave of the registry and resulted in an enriched sample of women and ethnic minorities. In the 1985–1986 registry, in-hospital mortality in women undergoing percutaneous coronary intervention (PCI) was 10-fold higher than in men. 87 To further explore this observation, the NHLBI reopened the registry in 1993–1994 to women only, a novel concept that resulted in a study of 583 women. 88 These strategies are models for planning clinical studies to enhance our understanding of potentially important issues specific to women with CVD.
Given the known differences in the type, treatment, and outcomes of MI in women and men, it is important to explore the basis for sex differences in thrombosis. Experimental studies reveal a difference in various components of hemostasis between women and men. 89 Several genes coding for proteins involved in hemostasis are regulated by sex hormones, suggesting a molecular mechanism 90 for the observation that estrogens increase the risk of venous thrombosis. The relevance of this finding to arterial thrombosis is not well explored. Whereas aspirin decreases platelet reactivity to a similar extent in women and men, it is not as effective in primary prevention of MI in women, in contrast to its superior efficacy in stroke prevention in women in comparison to men (Fig. 4). Further investigation of mechanisms of sex differences in clinical states of arterial thrombosis are needed.
To place the issue in perspective, it is notable that among the 1.4 million patients discharged with a diagnosis of an ACS in 2005, there were approximately 600,000 with unstable angina and over 800,000 with an MI. 91 Of the 1.2 million patients discharged with a diagnosis of new or recurrent MI, 60% were men and 40% women, at a cost of $76 billion to the nation. 91 Although the incidence of MI is higher in men overall, the risk of death following an MI for women is higher in virtually every study, including those in both the prereperfusion and postreperfusion eras. 92,93 Vaccarino et al. 21 have documented that this increase in adverse female mortality is explained by a higher death rate in the younger but not older women in comparison to men (Fig. 5). In patients treated with fibrinolytic therapy in the Thrombolysis in Myocardial Infarction (TIMI)-II trial, significantly higher rates of death and re-infarction were observed in women compared with men at 6 weeks and 1 year, even after adjustment for age and comorbidity. 92 The Enoxaparin and Thrombolysis Reperfusion for Acute Myocardial Infarction Treatment-Thrombolysis in Myocardial Infarction (ExTRACT-TIMI)-25 study demonstrated a higher incidence of death after reperfusion with fibrinolytic therapy in women (with ST-elevation MI (STEMI)) compared with men at all ages. 94 Similar findings have been reported in trials of primary PCI for STEMI. 95 However, the absolute risk reduction in mortality in patients treated with fibrinolytic therapy is similar in women and men. The impact of revascularization on mortality in patients with cardiogenic shock complicating acute MI is also similar, with both women and men benefiting from early revascularization. 11 The sex differences in mortality after reperfusion are predominantly explained by baseline differences, including advanced age and greater comorbidity in women.
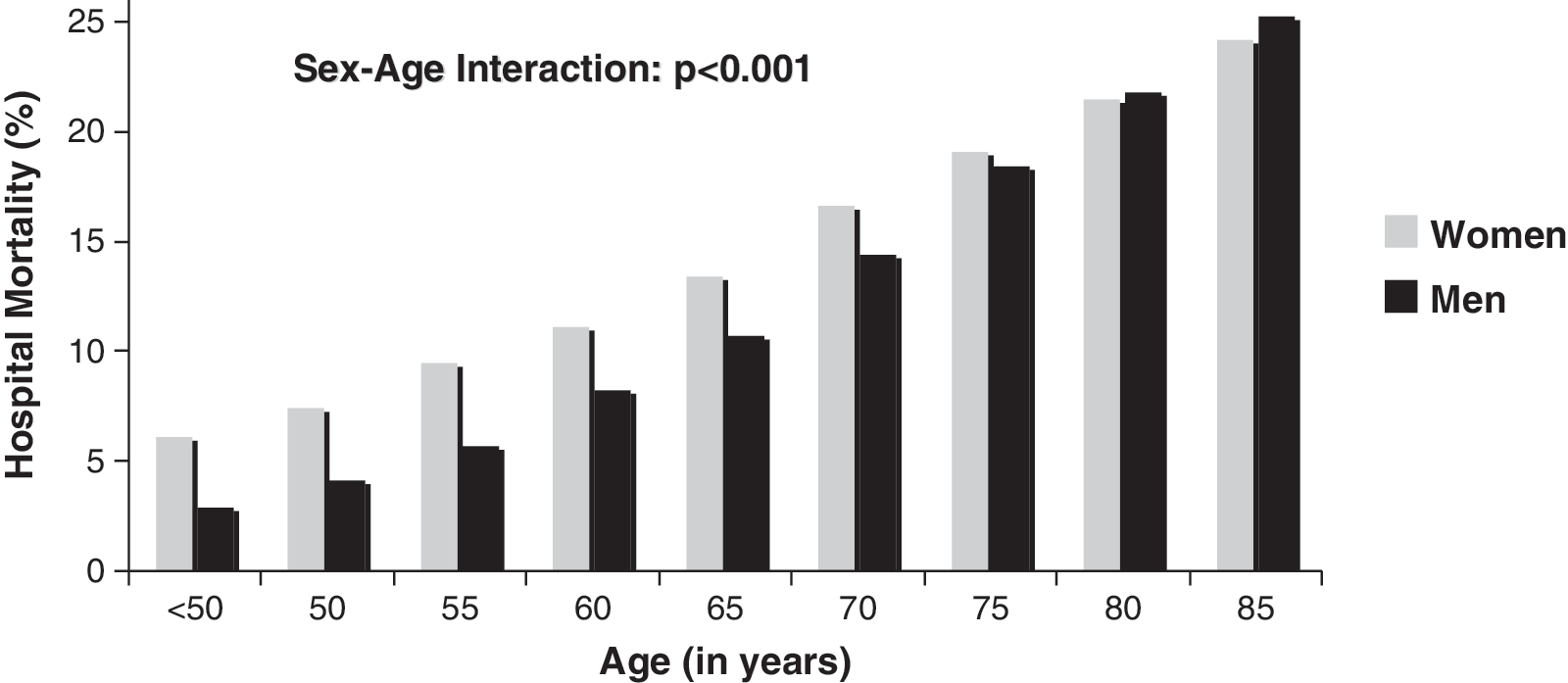
Sex differences in acute myocardial infarction outcomes. Reprinted with permission from Vaccarino et al. N Engl J Med 1999;341:217–225. 21
In patients treated with unfractionated heparin vs. enoxaparin after fibrinolysis in ExTRACT-TIMI-25, the cumulative incidence of death or nonfatal MI at 30 days was significantly lower in both men and women in the enoxaparin group. Of note, the absolute risk reduction was higher in women, 94 suggesting that sex differences may dictate a more beneficial response in women for specific therapies. For both women and men undergoing PCI, the clinical benefit of glycoprotein IIb/IIIa platelet receptor blockade with abciximab in terms of 30-day adverse events was similar, although women experienced a higher incidence of minor (but not major) bleeding. 96 In patients with ACS not undergoing early coronary angiography, there was a significant reduction in death or MI at 30 days in the group treated with IIb/IIIa receptor blockade compared with placebo. When analyzed separately for women and men, it was noted that men experienced benefit with an odds ratio (OR) of 0.81 (95% CI 0.75-0.89) compared with a suggestion of harm among women (OR 1.15, 95% CI 1.01-1.30); high-risk women, defined by an elevated troponin level, derived benefit. 69 Overall, women with ACS and STEMI appear to derive similar benefit from pharmacological therapy in comparison to men, although they are more likely to have bleeding problems. Prior studies document that women are more likely to be overtreated with antithrombotic medication compared with men, 97 leading to worse outcomes because of higher bleeding risk. More recently, in ExTRACT-TIMI-25, there was a higher incidence of bleeding with enoxaparin than with unfractionated heparin in both women and men, but a sex difference in bleeding risk was not observed likely because medication doses were adjusted for age and renal function. 94
Women are more likely to have ACS and less likely to have STEMI than men, yet 30-day mortality or reinfarction with STEMI is higher in women than in men. 98 Notably, within non-STEMI patients, there is no sex difference in mortality, and within patients with unstable angina, mortality is lower among women. 98 Although prior studies have observed higher rates of plaque erosion compared with rupture in women, 12 they should be interpreted with caution because women with STEMI tend to be excluded from trials of fibrinolytic therapy based on their advanced age. In fact, the TACTICS TIMI-18 investigators evaluated biomarkers in patients with ACS and reported a higher prevalence of such markers as CRP and brain naturetic peptide (BNP), that is, markers of inflammation and heart failure, 24 whereas men had a higher prevalence of troponin and creatine kinase, suggesting that MI in men was caused by plaque rupture.
How do these sex differences impact our therapy? Overall, in patients with ACS, treatment with a routine invasive compared with a selective invasive strategy results in a lower risk of death or MI (OR 0.82, 95% CI 0.72-0.93). In the studies that separated results by sex, however, the benefit of the routine invasive strategy was seen only in men and high-risk women. 99,100 Moreover, in both women and men, the routine invasive strategy was of benefit in the presence of at least one positive biomarker. In women without a positive marker, however, the invasive strategy was actually harmful, 24 whereas among men, there was no difference between the invasive and conservative strategies in the absence of a positive marker.
These data have resulted in the new sex-specific recommendations in the ACC/AHA practice guidelines for management of unstable angina and NSTEMI. 101 For women with high-risk features, recommendations for the invasive strategy are similar to those in men, but for women with low-risk features, an initial noninvasive strategy is recommended. Numerous studies of patients undergoing PCI have reported a higher in-hospital mortality in women in comparison to men, and it has been shown that the sex difference in mortality persists in patients with or without STEMI undergoing PCI with stents. 102 It has also been shown that women treated with drug-eluting stents derive similar benefit as men, with a decreased incidence of repeat revascularization compared with patients treated with bare metal stents. 103
In summary, the sex differences in thrombosis and outcomes in women with MI and ACS support further investigation of sex-specific therapeutic strategies. Several studies evaluating intracoronary delivery of IIb/IIIa platelet receptor antagonists with both abciximab and eptifibatide have shown some benefit with respect to decreased bleeding risk in women. 104 Stent delivery of pharmacological agents, coating of stents, and bioabsorbable stents are potential areas of investigation of relevance to women. Finally, developing systems of care that increase the number of patients with timely access to primary PCI may be of particular benefit in women, as they have an increased incidence of stroke following treatment with fibrinolytic therapy. 105
Targeting these issues in women provides a unique opportunity for sex-specific innovation. Because women have a greater risk than men of thrombosis related to estrogen, as well as more bleeding complications related to anticoagulant treatment, thrombosis management with CVD strategies that include devices should be preferentially evaluated in women.
Sex Differences in Stem Cell Therapy for CVD
Dr. Eduardo Marbán
The area of sex differences in health and disease is ripe for exploration. Scientifically, it is an area that is exploding and may be of particular importance for stem cell therapy. A list of sex differences gleaned from the literature is shown in Table 1. 106 –109 Additional preclinical work conducted by Taylor's group 62,63 demonstrates important sex differences in endogenous and exogenous PC function that suggest that female PCs promote cardiovascular repair. Prospective human clinical study design can take direction from these preclinical studies to maximize regenerative strategy success at this early stage.
Stem cells that are being investigated for use in regenerative medicine are primitive self-renewing multipotent cells, with multipotent meaning that the cells have multilineage potential. The types of cells that have been considered for regenerative therapy include embryonic stem cells, which have the advantage of being totipotent (e.g., they can actually evolve into all different types of tissues). Nevertheless, there are concerns, such as the potential of cells to develop into other tissues, immune rejection, and ethical dilemmas involving the destruction of the blastocyst. Therapeutic cloning, that is, the production of genetically identical individuals solely for the purpose of generating their stem cells, is probably the only tangible way of using an embryonic stem cell without involving immune reactions. The recent creation of genetically engineered somatic cells, such as fibroblasts, which then acquire embryonic stem cell characteristics (so-called induced pluripotent stem cells, commonly abbreviated as iPS cells), is an exciting new development 110 but comes with all the risks associated with genetically manipulated cells.
Currently, bone marrow stem cells (allogenieic cells and autologous cells) have been used in over 3000 heart patients worldwide and are derived either from the peripheral blood or from resident bone marrow cells. An initial clinical trial using BMNCs yielded modest improvements in LV ejection fraction in post-MI patients, with a good safety profile and an overall decrease in serious adverse events. 111 These results are sufficiently encouraging in that they prompt the search for the best delivery method, the best patient population, and the best cell type. In terms of mechanism of benefit, it is questionable whether the cells actually make new heart tissue vs. initiating paracrine mobilization of endogenous repair mechanisms.
In the area of organ-specific stem cells, skeletal myoblasts or, more recently, endogenous cardiac stem cells have been used. Evaluation of endothelial PCs has demonstrated that the number of colony-forming units (CFUs), as well as a migratory assay in vitro, is significantly (50%–100%) higher in women than in men. 106 The study of MSCs has suggested that male cells produce more TNF and less VEGF than do female cells. 108 Postischemic rat hearts injected with female MSCs had a higher functional recovery than did those injected with male MSCs. 107 We studied 80 biopsies from patients of both sexes and found no differences in proliferative capacity; however, the study was not designed to elicit such differences. 109
Future work needs to move to exploration of mechanisms to explain these stem cell differences. Females have higher circulating levels of PCs, with greater migratory capacity and higher rates of tissue repair. CVD tissue repair strategies should ideally be tested first in females to have the best chance of success for proof-of-concept, followed by testing in the more challenging male models.
Discussion
CVD is the leading killer of both women and men. A substantial amount of observational data documents that sex differences in CVD exist, yet mechanistic knowledge, ranging from basic science inquiry to pathophysiological understanding, diagnostics, and therapeutics, is limited. The available data implicate a variety of mechanisms to explain why CVD is qualitatively and quantitatively different in women and men. Future research should continue to move from observational studies to examination of sex-specific mechanisms in order to develop novel sex-specific therapies, including new devices, tissue engineering, thrombotic strategies, pharmacogenomics, and stem cells, to improve outcomes for women and men.
Footnotes
Acknowledgments
This work was supported by contracts from the National Heart, Lung and Blood Institutes Nos. N01-HV-68161, N01-HV-68162, N01-HV-68163, N01-HV-68164, R01 HL090957-01A1, and R03 AG032631-01; a GCRC grant MO1-RR00425 from the National Center for Research Resources; and grants from the Gustavus and Louis Pfeiffer Research Foundation, Denville, New Jersey; The Women's Guild of Cedars-Sinai Medical Center, Los Angeles, California; The Ladies Hospital Aid Society of Western Pennsylvania, Pittsburgh, Pennsylvania; the Edye L. Broad Endowment in Women's Heart Research, Cedars-Sinai Medical Center, Los Angeles, California; and the Barbra Streisand Women's Heart Disease Research and Education Program. The symposium meeting was sponsored by an unrestricted medical education grant by Cook Inc.
We thank Shivani Dhawan for writing assistance in preparing this article.
Disclosure Statement
A.K.J. has stock options at Wyeth and is a research site PI at Abiomed Abbot Vascular Accumetrics. S.M. serves as a part-time consultant in the capacity of senior policy advisor to the Cook Group, Inc.
The authors have no conflicts of interest to report.