
Abstract
Interstitial cystitis/painful bladder syndrome (IC/PBS) is a chronic bladder disorder characterized by pelvic pain and irritative voiding symptoms. The symptoms of IC/PBS can overlap with such conditions as endometriosis, recurrent urinary tract infection, chronic pelvic pain, overactive bladder, and vulvodynia. The etiology of IC/PBS is likely multifactorial and may involve a defective urothelium, neurogenic upregulation, and mast cell activation. A thorough patient history and physical examination are critical in the differential diagnosis of IC/PBS. Frequent follow-up and patient education are important components of treatment once a condition is diagnosed. A multimodal approach to therapy can provide optimal relief for patients with IC/PBS.
Introduction
Interstitial cystitis/painful bladder syndrome (IC/PBS) is a chronic bladder disorder with symptoms of pelvic pain and irritative voiding symptoms, such as urinary urge and frequency. 1,2 Pelvic pain often is the chief complaint of patients with IC/PBS. 3 Patients with IC/PBS often have multiple pain generators, including the bladder, the bowel, the reproductive tract, and the pelvic floor musculature. Many experts thinks that IC/PBS should, therefore, be considered part of a visceral pain syndrome. These other pain generators may be the primary source of pain, with bladder symptoms resulting from neurogenic inflammation, which is a major component of visceral pain syndromes. 4 –6
IC/PBS can be difficult to diagnose, as the symptoms overlap with a variety of other disorders, including endometriosis, urinary tract infection (UTI), chronic pelvic pain (CPP), overactive bladder (OAB), and vulvodynia. 7,8 Because there is no definitive diagnostic test, IC/PBS remains a diagnosis of exclusion. 2 The presence of additional symptoms caused by other pain generators can confuse the diagnosis even further. Patients may not receive an accurate diagnosis for years. The median time between the development of IC/PBS symptoms and the diagnosis is approximately 5 years. 9
Professionals in women's healthcare have the opportunity to diagnose IC/PBS early in the course of the disease and to initiate treatment. 10 Earlier treatment may result in better outcomes. A study of 128 patients with IC/PBS found that those who initiated therapy ≤6 months after diagnosis had significant symptom improvement compared with patients who began therapy ≥24 months after diagnosis. 11 Clinicians should maintain a high level of suspicion of IC/PBS in women who experience urinary urgency or frequency. 12
Pathophysiology of IC/PBS
The pathophysiology of IC/PBS may be multifactorial (Fig. 1). 13 –15 Some symptoms of IC/PBS may arise from a defective urothelium lining. 16,17 The bladder epithelium is normally highly impermeable to urinary solutes and irritants, such as urea, ammonia, and protons. 18 Deficiency of the glycosaminoglycan (GAG) layer on the bladder surface (resulting in increased permeability of the urothelium) may allow irritating solutes, such as potassium, to leak from the urine into the bladder tissue. 4,19 –22 The compromise of this protective layer plays a major role in the symptoms of IC/PBS, such as pelvic pain and irritative voiding symptoms. 15,23 Additionally, cross-sensitization or visceral cross-talk with other pain generators in the pelvis may be able to induce IC/PBS via neurogenic inflammation. 24 Increased numbers of nerve fibers have been found in the bladders of patients with IC/PBS. 2,25 Immune response, in the form of mast cell proliferation, may also be involved. 26 Some studies have suggested that subepithelial mast cell activation is increased in IC/PBS and may lead to more mast cell upregulation, inflammation of the bladder wall and injury to the GAG layer, and eventual fibrotic changes. 15,27
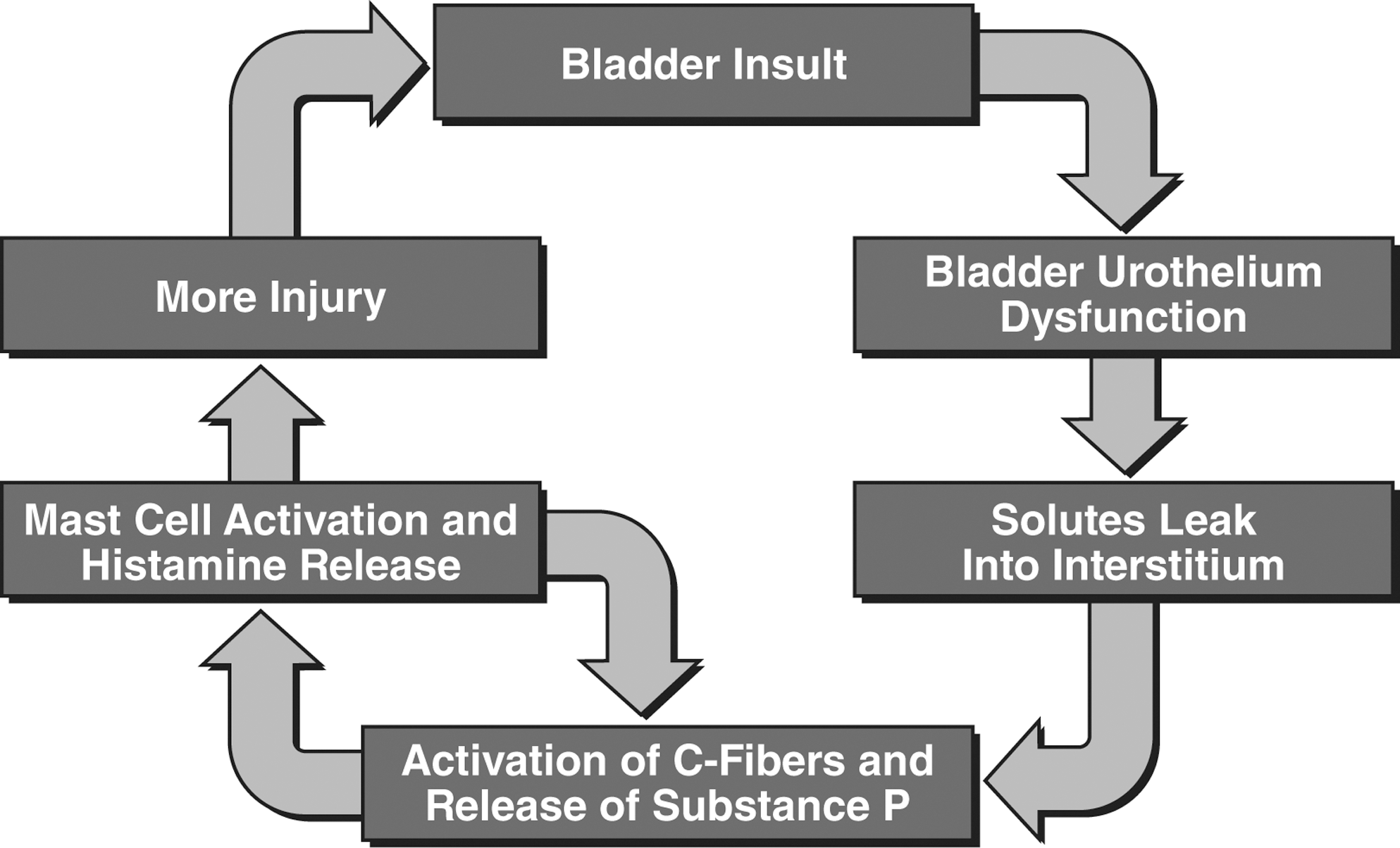
Proposed model for the pathogenesis of interstitial cystitis/painful bladder syndrome (IC/PBS). Adapted with permission from Evans. Rev. Urol. 2002;4:S16–S20. 15
Antiproliferative factor and Tamm-Horsfall protein (THP) are potential markers for IC/PBS. Antiproliferative factor, a protein that is secreted by bladder cells from patients with IC/PBS, has been shown to inhibit bladder cell proliferation. 28,29 Decreased protective effects of THP have been associated with uropathology. 30 These results suggest a causal relationship between decreased THP levels and IC/PBS. 31
Evaluation of Suspected IC/PBS
A thorough patient history is the first step in evaluating patients suspected to have IC/PBS. 32,33 It is important to characterize pain—which typically worsens with increasing bladder volume—as well as urgency, voiding history, nocturia, and sexual symptoms. Flares with seasonal allergies and sexual intercourse should be noted, as these can be part of the clinical presentation of IC/PBS. 34 Voiding typically relieves pain, 35 and patients may void frequently to relieve pain as the bladder fills. Voided volumes of <120 mL are common.
Several diseases and conditions occur more often in patients with IC/PBS than in the general population. Compared with control subjects, patients with IC/PBS are significantly more likely to be diagnosed with irritable bowel syndrome (IBS), 36 –38 inflammatory bowel disease (IBD), allergies, fibromyalgia, and systemic lupus erythematosus (SLE). 36 Patients with IC/PBS are also more likely to have depression. 38 A history of sexual abuse may be more common among patients with IC/PBS: in a cohort of 87 patients with IC/PBS referred to a pelvic pain center, nearly 60% had a history of sexual abuse. 39 IC/PBS patients should be screened, and if any of these conditions are present, patients should be treated or referred to the appropriate specialist.
Questionnaires can be helpful in screening for IC/PBS. The most commonly used screening tools are the Pelvic Pain and Urgency/Frequency (PUF) Patient Symptom Scale (Fig. 2) and the O'Leary-Sant (OLS) Interstitial Cystitis Symptom and Problem Index (Fig. 3). 40,41 Both surveys include questions about pain, urinary urgency, frequency, and nocturia and how these symptoms affect daily life. These tools can also be used to assess treatment efficacy. The PUF includes additional specific questions about dyspareunia. The PUF is scored from 0 (no symptoms) to 35 (severe symptoms and bother). Higher scores on the PUF are associated with a greater likelihood of having a positive potassium sensitivity test (PST). 40 Any PUF score >10 warrants further evaluation for possible IC/PBS. Scores >15 are common among patients with IC/PBS.

The Pelvic Pain and Urgency/Frequency (PUF) Patient Symptom Scale. ©2000. Adapted with permission from Parsons et al. Urology 2002;60:573–578. 40
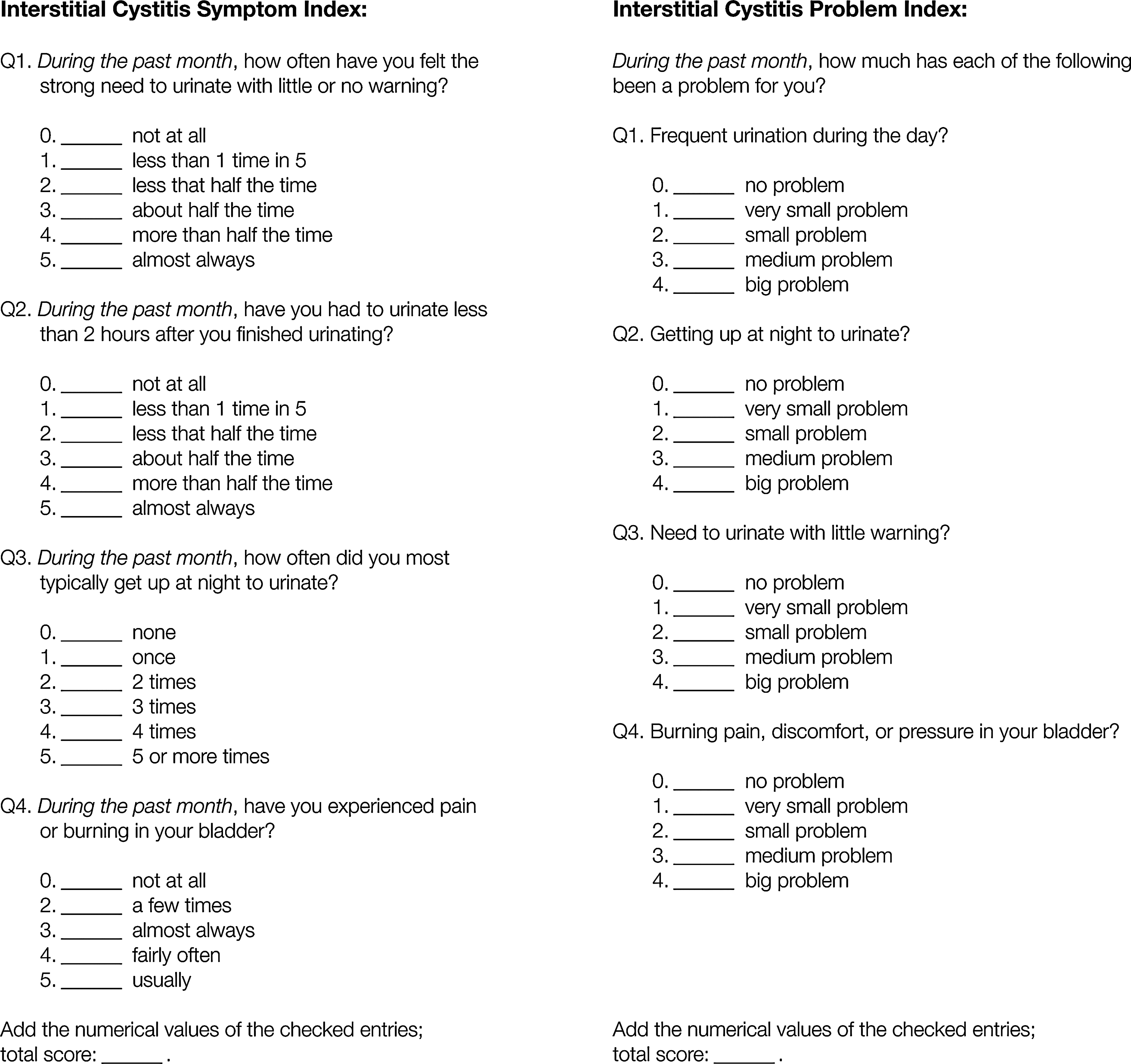
O'Leary-Sant (OLS) Symptom Screener. Adapted with permission from O'Leary et al. Urology 1997;49:58–63. 41
Physical examinations are critical components of diagnosing IC/PBS. The physical examination in IC/PBS patients can be emotionally distressing because of pain, so it is important that the physician proceed slowly and carefully. 8,42 Because the bladder is a pain generator in IC/PBS, 2 tenderness with single-digit examination of the trigonal area (bladder base or urethra) can help establish a diagnosis of IC/PBS, 42 as can pain in the pelvic floor or levator ani. 8 Patients with IC/PBS tend to have urethral or bladder tenderness, whereas those with vestibulodynia have vestibular tenderness. 43 Tenderness with single-digit examination of the vaginal fornices can help distinguish endometriosis from IC/PBS. 42
Laboratory studies also can help distinguish IC/PBS from other conditions. 2 Urinalysis can rule out hematuria, and urine culture is required to identify bladder infection. 24,44 Cytology and CT scan with double contrast when indicated (hematuria, history of smoking, age >40 years) can help rule out urinary tract malignancies. 45 Patients with results that suggest a malignancy should be referred to a urologist. Several optional diagnostic tests can help diagnose IC/PBS. The presence of glomerulations seen on cystoscopy with hydrodistention may aid in the diagnosis of IC/PBS. Cystoscopy should be performed routinely in patients with gross hematuria or significant microhematuria, especially in patients with a history of smoking. 13 A negative cystoscopic evaluation should never be used to rule out IC/PBS because many patients with early IC/PBS will not have glomerulations. 46 The PST may indicate a defective bladder lining. The PST involves intravesical instillation of a potassium solution, which triggers symptoms of pain and urgency in patients with abnormal bladder surface permeability. 47 Intravesical instillation of an anesthetic cocktail can be used as a diagnostic tool as well as a treatment. Known as the “anesthetic bladder challenge,” this test can help localize pain to the bladder. 48 –50
Conditions with Symptoms That Mimic IC/PBS
Symptoms of IC/PBS overlap with many other common urological and gynecological disorders, which may complicate the diagnosis of IC/PBS. Among 134 consecutive patients with pelvic pain in general gynecological practices, 85% had a positive PST and 75% reported urological symptoms, indicating that the bladder was a potential source of symptoms. 51 However, only 3.0% of patients were given a clinical diagnosis of IC/PBS based on their chief symptomatic complaint. The rest were given a clinical diagnosis of pelvic pain (37.3%), vulvodynia (24.6%), endometriosis (10.4%), dyspareunia (8.2%), UTI (7.5%), yeast infection (4.5%), or other conditions. 51 These results suggest that clinicians should consider the bladder a potential source of pelvic pain in all patients with CPP.
Here, we briefly describe some of the conditions that may mimic or coexist with IC/PBS. We also discuss their presentations and etiologies and how IC/PBS can be distinguished from these conditions. A summary is shown in Table 1.
IC/PBS, interstitial cystitis/painful bladder syndrome; rUTI, recurrent urinary tract infection; CPP, chronic pelvic pain; OAB, overactive bladder.
Endometriosis is characterized by the presence of endometrial-like glands and stroma outside of the uterine cavity. 52 –54 Symptoms include pain in the lower abdomen, dysmenorrhea, and dyspareunia and can also include such voiding symptoms as dysuria and frequency. 54,55 The etiology of endometriosis is unclear but may include retrograde menses, transport of endometrial tissue through the bloodstream or lymph, or cellular metaplasia. Endometriosis occurs in 1%–10% of women of reproductive age and in 25%–35% of infertile women, it is reported. 52,56 Endometriosis is definitively diagnosed by histologic study. Visual diagnosis alone is accurate in only 50% of cases. 54 Endometriosis and IC/PBS frequently coexist in the same patient. 57 –59 In one study of women with CPP and bladder tenderness on examination, >70% had both endometriosis and IC/PBS. 58 Although rare, bladder endometriosis can mimic the symptoms of IC/PBS. 7 Combining diagnostic laparoscopy and cystoscopy with hydrodistention may allow histological confirmation of endometriosis as well as glomerulations due to IC/PBS. 7,59
Symptoms of recurrent UTI (rUTI) include urgency, frequency, nocturia, and pelvic pain. 60 Diagnosis is established by a positive urine culture. 61 If patients have rUTI but urine cultures are negative, other conditions, such as IC/PBS, should be considered. Physicians should also recognize that patients with IC/PBS may have a concurrent UTI. This possibility should be ruled out in all patients with IC/PBS who experience symptom flares. 35
CPP is pain ≥6 months in duration that is severe enough to affect daily functioning or that requires medical care. 8 The specific etiology of CPP is often unknown and may be multifactorial. 1,8 Gynecological conditions that can cause CPP include endometriosis, adhesions, pelvic inflammatory disease (PID), cysts, and polyps. 1 However, a retrospective cohort analysis of a large primary care database in the United Kingdom found that only 20.2% of all cases of CPP had a gynecological etiology. 62 Gastrointestinal diagnoses represented 37.7% of cases, with IBS accounting for 29.1%. Cystitis accounted for 30.8% of diagnoses in this population of women with noncyclic pain lasting for ≥6 months. Up to half of women in primary care practices who have CPP may have more than one diagnosis for their pain. As described previously, it is common for a patient with CPP to have both endometriosis and IC/PBS. 1 Chung et al. 58 reported that in a patient with CPP and bladder symptoms, there is a 96% likelihood that IC/PBS is also present.
A detailed medical history and physical examination are the basis for diagnosing the cause of CPP. 1 The use of questionnaires, such as the PUF or OLS indices, may elicit information about urinary symptoms. Tenderness of the bladder base on pelvic examination is a characteristic feature of IC/PBS that may help to distinguish it from other causes of CPP. 42 Optional tests, including laparoscopy and diagnostic imaging, may also be helpful. 1,8 Additional useful information may be gained from the PST or intravesical anesthetic challenge.
OAB is characterized by urgency, with or without urge incontinence, and usually includes frequency and nocturia. 63 The key symptom is urgency. 64 OAB and IC/PBS can coexist in the same patient. 65 It can be caused by detrusor overactivity, which usually can be demonstrated through urodynamic testing. 63 Urodynamic findings that suggest IC/PBS include painful sensory urgency and reduced bladder capacity. 66 –68 OAB may also be caused by various pathologic conditions that increase afferent nerve activity, such as IC/PBS. Urgency is a common symptom of both OAB and IC/PBS, although the cause differs. In patients with OAB, urgency results in a strong desire to avoid leakage, whereas in patients with IC/PBS, urgency results in a strong need to void to relieve pain caused by bladder fullness. 69
Vulvodynia is characterized by vulvar discomfort, often reported as burning pain. Pain can occur during intercourse or vigorous activity or even at rest. 70 The etiology of vulvodynia is unknown, and diagnosis is one of exclusion, but its histological characteristics include a pattern of neuropathic upregulation. 4,71 Previous estimates of the prevalence of vulvodynia ranged from 150,000 to 200,000 women in the United States (based on estimates of a small number of healthcare providers and the average number of vulvodynia patients each was seeing). 72 However, the incidence could be as high as 15% of patients in general gynecology practice. 73 Vulvodynia symptoms that overlap those of IC/PBS include pain and dyspareunia, but lack of frequency and nocturia can help distinguish vulvodynia from IC/PBS. It is also possible to see patients with both IC/PBS and vulvodynia. 7,74 Patient history and physical examination are important in diagnosing vulvodynia. A history of chronic pain at the vestibule lasting >3 months can lead to suspicion of vulvodynia. 72 Infectious causes may include viral, bacterial, or fungal organisms, so these must be ruled out as causes of vulvar pain. Vulvar dermatoses may also account for vulvar symptoms. 75 Tenderness to pressure with a cotton swab at the vestibule is a hallmark of vulvodynia, 72 whereas bladder base tenderness is typical of IC/PBS. 43
Interstitial Cystitis Treatment
Regardless of the initial insult, the pathophysiology of IC/PBS involves a neuroimmune cascade of events that causes symptoms of bladder pain and urinary urgency and frequency. Multimodal therapy allows the clinician to target multiple steps in this cascade (Fig. 4). 15 Treatment should consist of education and other nonpharmacological interventions, oral medications, intravesical instillations, or a combination of these therapies tailored to the individual patient.

Multimodal therapy to target multifactorial etiology. Adapted with permission from Evans. Rev. Urol. 2002;4:S16–S20. 15
Education of patients with IC/PBS helps empower them to control their symptoms and to be active participants in their own therapy. Patients should be counseled to avoid triggers that lead to increased IC/PBS symptoms. They should also be encouraged to reduce stress and use support groups to deal with the impact IC/PBS has on their daily lives. 76 Dietary changes can provide symptom relief. 77 A study showed that IC/PBS patients can identify foods and drinks that aggravate their symptoms in 51%–62% of cases. Avoiding certain foods, such as those with a high acid content (e.g., alcoholic beverages, carbonated citrus-based drinks, citrus fruits, tomatoes), can minimize or prevent IC/PBS flares in some patients. 78 Consuming foods, such as pasta with nontomato sauces or fruits with low acid content (e.g., watermelon), can reduce IC/PBS symptoms. 79
Pentosan polysulfate sodium (PPS) is a heparinoid compound 80 that is thought to replenish the defective bladder lining. 33 This drug is the only Food and Drug Administration (FDA)-approved oral treatment for the symptoms of IC/PBS. 80 PPS is also available in the United Kingdom, Germany, and Italy. It also has an antihistaminic effect. 81 Patients should be assessed after 3 months of treatment with PPS. Based on levels of improvement and side effects, treatment can be continued for another 3 months and then continued as needed. 24,82
Tricyclic antidepressants, such as amitriptyline, have been used to treat IC/PBS symptoms. 3,24,83 The anticholinergic effect of these drugs can reduce symptoms of urgency. Tricyclics are commonly used in multiple pain disorders, such as fibromyalgia and IBS, with promising results. 84,85 They provide significant improvement of symptoms in IC/PBS. 83 Antihistamines, such as hydroxyzine, have been used for their efficacy in decreasing mast cell activation and reducing inflammation. 44,86,87
Immunosuppressive agents may be used as second-line therapy in IC/PBS. Prednisone has shown efficacy for severe treatment-refractory IC/PBS in a small clinical trial. 88 Thirty patients with Hunner's ulcer subtype IC/PBS showed considerable improvement following endoscopic submucosal injection of triamcinolone. 89 Cyclosporine has been shown in clinical trials to relieve the symptoms of severe IC/PBS. 90,91 Symptoms generally recur after treatment is discontinued. Patients taking cyclosporine should be monitored for renal toxicity and hypertension.
Intravesical therapy can be used for flare management. 92 Dimethylsulfoxide is the only FDA-approved intravesical IC/PBS treatment. 14,93,94 Intravesical anesthetic instillations can bring immediate relief. A study of patients with IC/PBS receiving intravesical instillations of heparin and alkalinized lidocaine showed that this treatment provided immediate and sustained relief of pain and urgency. 50,95
Physical therapy techniques include biofeedback to control pelvic floor dysfunction, 78 soft tissue massage including myofascial release, and bladder retraining, which is most often used in patients with little or no pain. 79,96 Physical therapy is intensive at the outset and then should be repeated at least once a year to maintain the benefit.
Anticonvulsants, such as gabapentin, often are prescribed for neuropathic pain. 97,98 These drugs can be used to treat patients with refractory IC/PBS who have failed more conventional treatments. 24
Sacral nerve stimulation can be beneficial for alleviating symptoms in refractory IC/PBS, especially for urinary frequency, urgency, and voiding dysfunction. 99
Management Guidelines
Because patients with IC/PBS have a wide range of symptoms, management must be individualized. Frequent follow-up and patient counseling about disease state and expectations play an important role in the management of IC/PBS, to actively involve the patient in her treatment, monitor her progress, and set realistic expectations. 82,86 Management requires identification and treatment of all pain generators, including associated endometriosis, IBS, fibromyalgia, and vulvodynia. 24,100 Therapy may take weeks or months to achieve optimal relief, so patients should be counseled to expect therapy to take time. The duration of symptoms before initiation of therapy seems to be directly related to the time needed to achieve symptom relief. 11,101,102 Follow-up visits at regular intervals to monitor patients and address their concerns are important for optimal outcomes. Treatment plans can be modified based on patient response to therapy.
Conclusions
IC is a chronic bladder disorder with symptoms of urinary frequency, urgency, and pelvic pain. IC/PBS is often a visceral pain syndrome with multiple pain generators, which can make the diagnosis of IC/PBS difficult. Patients with a history of rUTIs that are culture negative, those with endometriosis and significant bladder symptoms, those with OAB who respond poorly to therapy, and those with vulvodynia or CPP are all likely to have untreated IC/PBS. The primary providers of care for women with pelvic pain must consider the bladder as a very important and common source of pain. The earlier the diagnosis is made and therapy is begun, the faster patients with IC/PBS will experience improvement of their symptoms.
Footnotes
Acknowledgments
We thank Sumathi Jagger, M.D., and Barbara Leeper, Ph.D., for writing assistance and Charmaine Clarke for editorial assistance.
Disclosure Statement
C.W.B. has received grant/research support from Ortho-McNeil Pharmaceutical, Inc. and is a member of the speakers' bureau for Ortho-McNeil, Astellas, and Novartis. F.M.H. is a consultant for Ortho-McNeil and Ethicon and is a member of the speakers' bureau for Abbott Pharmaceutical. P.K.S. is a consultant and member of the speakers' bureau for Ortho-McNeil Pharmaceutical, Inc.