
Abstract
Objective:
To compare health-related quality of life (HRQOL) in those with and without metabolic syndrome in a general Iranian population.
Methods:
This was a cross-sectional study of HRQOL conducted in a sample of individuals with and without metabolic syndrome using the data obtained from the Tehran Lipid and Glucose Study (TLGS) and information specifically collected for the present investigation. Metabolic syndrome was defined according to the adult treatment panel III (ATPIII) and HRQOL was assessed using the Short Form Health Survey (SF-36). Logistic regression analyses were performed for the whole sample and both sexes while adjusting for potential confounders in order to estimate odds ratios for predicting HRQOL in this population.
Results:
In all, 950 participants with (n = 361) and without (n = 589) metabolic syndrome were studied. The mean age of participants was 46.5 ± 14.4 years. In women, but not in men, metabolic syndrome had an independent role in predicting poor HRQOL. With increase in the number of metabolic syndrome components, there was a significant decreasing trend in women's physical component summary scores.
Conclusions:
The results indicate that metabolic syndrome is associated with poor HRQOL in women but not in men, and the association is formed mainly in relation to physical rather than mental health.
Introduction
The cluster of metabolic abnormalities known as the metabolic syndrome leads to increased risk for cardiovascular diseases (CVD) and diabetes type 2. 1 –4 Insulin resistance and abdominal obesity seem to be underlying risk factors for development of this syndrome. 5 Existing data show a considerable prevalence of the metabolic syndrome in both developed and developing countries. 6 –8 Its prevalence among Tehranian adults has been estimated to be >30%, which is remarkably high. 9
Health-related quality of life (HRQOL) includes the physical, mental, and social aspects of health and is an essential outcome measure that has gained much attention in recent years. HRQOL specifically focuses on an individual's perception of health and life satisfaction that may be linked with the World Health Organization (WHO) definition of health as “[the] state of complete physical, mental, and social well-being, and not merely the absence of disease and infirmity.” 10 –12
There are few studies that examine HRQOL in the metabolic syndrome. The association between the metabolic syndrome and the physical but not the mental domain of HRQOL has been shown in a large sample of an obese Italian population. 13 Metabolic syndrome seems to be associated with the functional dependence, depression, and low HRQOL in an elderly Brazilian community. 14 Some of the components of the metabolic syndrome, such as hyperglycemia, hypertension, and abdominal obesity, were associated with impaired HRQOL in postmenopausal Ecuadorian women. 15 In addition, there is evidence suggesting significant negative associations between insulin resistance and the physical domain of HRQOL in the elderly. 16 Using different HRQOL instruments, a recent study has shown that U.S adults with the metabolic syndrome have a worse HRQOL than adults without this syndrome. 17
Although previous studies have investigated the relationship between quality of life and the metabolic syndrome, they have generally focused on specific groups, and there is relatively less information available about the general populations. Moreover, little is known about the impact of the metabolic syndrome on HRQOL in Middle Eastern countries. Considering the fact that QOL takes on different meanings according to the area and culture of the population, there is a need to investigate the association between the metabolic syndrome and HRQOL in such countries. In this study, we examined the strength of association between different domains of HRQOL and the metabolic syndrome in a large sample of nondiabetic Iranian adults.
Materials and Methods
Subjects and design
The Tehran Lipid and Glucose Study (TLGS) was designed to determine risk factors for atherosclerosis in an urban population in Tehran and to develop population-based measures aiming at changing lifestyles and halting the increasing trend of diabetes and dyslipidemia. The study is divided into two phases: a cross-sectional study of the prevalence of noncommunicable diseases, such as diabetes and CVD, and their associated risk factors, and a prospective 20-year follow-up study. A multistage, stratified cluster, random sampling technique was used to select 15,005 people, aged ≥3 years, from urban district 13 of Tehran, the capital of Iran. This district is located in the center of Tehran, and the age distribution of its population is representative of the overall population of Tehran.
During sampling, a list of all households covered by the district's three healthcare centers (the official bodies responsible for vaccination programs and collection of health-related statistics in a district) was used. Then, a random sample of households, stratified according to healthcare centers to achieve a distribution similar to the original population, was chosen, and from each household, all members ≥age 3 were recruited. The study began in 1997, and the cross-sectional phase was completed in 2000; the first follow-up survey began in 2001, was completed in 2005, and was repeated every 3 years. 18
In this study, a representative sample of 1411 people participating in the TLGS between September 2005 and September 2007 were interviewed by a trained interviewer. The interview data included quality of life data, sociodemographic information, physical activity, smoking habits, and medications used. From the initial sample, 1255 participants, aged ≥20 were recruited for this study; of this 1255, 276 (15.2%) participants were diagnosed as diabetic and excluded from the study. Finally, after elimination of 30 (3.1%) participants with missing data, the information of 950 participants was analyzed (Fig. 1). All participants gave written informed consent. The study was approved by the Ethics Committee of the Obesity Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences.
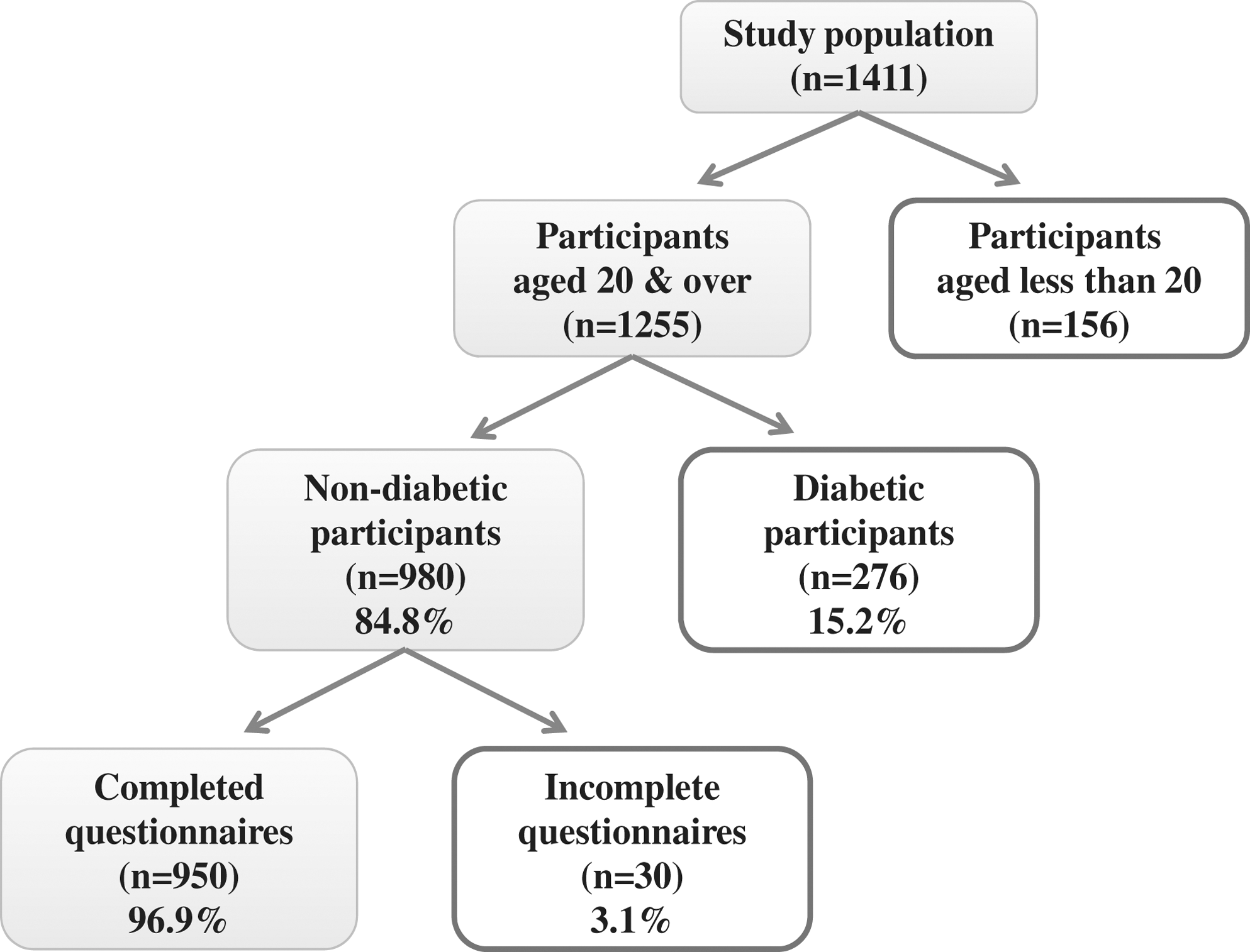
The sampling frame of study.
HRQOL measures
HRQOL was measured using the Iranian version of Short Form Health Survey (SF-36). It is a widely used questionnaire that measures eight health-related concepts, including physical functioning, role limitations due to physical health problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, and mental health, as well as a summary of physical and mental measures. 19 The psychometric properties of the Iranian version of the SF-36 are well documented. 20 For each scale, a score ranging from 0 to 100 was considered as the worst and the best health conditions, respectively. To calculate the physical component summary (PCS) and the mental component summary (MCS) scores, however, we used the Quality Metric health outcomes scoring software 2. The software uses all the 36 items to produce scores for the PCS and the MCS and applies a norm-based scoring algorithm empirically derived from the data of a US general population survey. 21
Definitions
Metabolic syndrome was diagnosed when three or more of the five following criteria were met 1 : elevated waist circumference (>102 cm in men or >88 cm in women), (2) reduced high-density lipoprotein cholesterol (HDL-C) (<40 mg/dL in men or <50 mg/dL in women) or on drug treatment for reduced HDL-C, (3) elevated triglyceride (TG) level ≥150 mg/dL or on drug treatment for elevated TG, (4) elevated blood pressure (≥130 mm Hg systolic blood pressure or ≥85 mm Hg diastolic blood pressure) or on antihypertensive drug treatment in a patient with a history of hypertension, and (5) elevated fasting glucose ≥100 mg/dL or on drug treatment for elevated glucose. Diabetes was defined based on a fasting glucose level >126 mg/dL or glucose levels 2 hours after an oral glucose tolerance test ≥200 mg/dL or receiving antidiabetes drugs. 22
Other measures
Waist circumference was measured at the umbilical level 23 over light clothing, using an unscratched tape meter, without any pressure to the body surface; measurements were recorded to the nearest 0.1 cm. Blood pressure was measured twice after participants were seated for 15 minutes using a standard mercury sphygmomanometer. There was at least a 30-second interval between these two measurements, and the mean of the two measurements was taken as the blood pressure. Twelve-hour fasting blood samples were collected in tubes containing 0.1% EDTA and were centrifuged at 4°C at 500 g for 10 minutes to separate the plasma. Blood glucose was measured on the day of blood collection by an enzymatic colorimetric method using glucose oxidase. Serum total cholesterol and TG concentrations were measured with commercially available enzymatic reagents (Pars Azmoon, Tehran, Iran) adapted to a Selectra autoanalyzer. HDL-C was measured after precipitation of the apolipoprotein B-containing lipoproteins with phosphotungstic acid. Low-density lipoprotein cholesterol (LDL-C) was calculated from serum total cholesterol, TG, and HDL-C, except when TG concentration was >400 mg/dL.
Additional information, including age, smoking status (considered in two groups, nonsmokers and ex-smokers vs. current smokers), 24 physical activity, 25 and current use of oral hypoglycemic agents, lipid-lowering agents, and antihypertensive medication, was obtained using the TLGS data.
Statistical analysis
Analysis was performed using SPSS software version 15.0 (SPSS, Chicago, IL). Data are presented as means, standard deviation (SD), percentages, and confidence intervals (CI). Continuous and categorical variables were compared using the Student t test and the chi-square, respectively. HRQOL scores between those with and without metabolic syndrome were compared using the t test. Multivariate logistic regression analysis was performed to estimate adjusted odds ratios (ORs) for poor HRQOL among the study sample. For the purpose of logistic regression analysis, PCS and the MCS were used. Relative to the mean scores, the study sample was divided into two groups: those who scored equal or greater than mean and those who scored below mean. The potentially confounding variables were entered into the models as independent variables to control for their influence on the results. In addition, similar analyses were performed separately for men and women.
Results
Nine hundred fifty participants with (n = 361) and without (n = 589) metabolic syndrome were included in the study. The mean age of the participants was 46.5 ± 14.4 years, and 64.3% (n = 611) were female. There were significant differences between those who were experiencing metabolic syndrome and those who were not, except for fasting blood sugar, physical activity, and smoking (Table 1).
Individuals who were taking hypertensive or antilipid drugs.
WC, waist circumference; FBS, fasting blood sugar; TG, triglyceride; HDL, high-density lipoprotein; definitions are based on National Cholesterol Education Program (NCEP) criteria. 1
Overall, except for the vitality (p = 0.1) and role emotional (p = 0.06) scales, there were significant differences between subgroups of the samples with and without metabolic syndrome (p < 0.01). However, gender-specific analysis showed that all of the significant differences belonged to women, in whom there were significant differences in physical functioning, bodily pain, social functioning, and the PCS and MCS scores between those with and without metabolic syndrome (p < 0.01) (Table 2). There were significant differences between prevalence of low HDL-C and high waist circumference in men and women (p < 0.001) (Table 3).
MCS, mental component summary; PCS, physical component summary.
Values indicate percentages (95% CI).
WC, waist circumference, FBS, fasting blood sugar; TG, triglyceride; HDL, high-density lipoprotein; definitions are based on National Cholesterol Education Program (NCEP) Criteria 1 .
To indicate determinant factors of poor HRQOL, multiple logistic regression analysis was performed. The results showed that age, gender, physical activity, education, and metabolic syndrome for the PCS and gender, marital status, and smoking for the MCS were significant determinants (Table 4). Further analysis for each gender, however, showed a relatively different perspective indicating that metabolic syndrome was a significant determinant of poor physical HRQOL for women but not for men (Table 5). In addition, we found that with an increase in the number of metabolic syndrome components, there was a significant decreasing trend in scores of the women's PCS (p < 0.001), which was not so in men (Fig. 2).

Physical and Mental Component Summary scores based on the number of metabolic syndrome components in men and women.
CI, confidence interval.
Discussion
This study shows that even after adjusting for potentially confounding factors, metabolic syndrome is independently associated with poor physical HRQOL in women but not in men. In women, there were significant differences between those with and without metabolic syndrome in the physical functioning, bodily pain, social functioning, PCS, and the MCS scores (p < 0.01). Except for the MCS, the other mentioned domains had a >5-point difference and were also clinically relevant. The findings of worse HRQOL among those with metabolic syndrome, extend the results obtained in two other studies conducted in Italy and in the United States. 13,17
In the present study, there were several reasons for analyzing data in men and women separately. First, the existing significant interaction between metabolic syndrome and gender; second, different distribution of risks between men and women for some variables (e.g., smoking); and third, certain gender differences in symptom presentation, management, and outcome, 26 that could affect peoples' perception of health and quality of life. Among the eight subscales of SF-36 that define physical and mental HRQOL, physical functioning, bodily pain, vitality, and social functioning showed significant ORs in women with metabolic syndrome compared with women without this syndrome. In men, however, there were no significant differences observed.
The mechanisms underlying these paradoxical gender differences in the association between HRQOL and metabolic syndrome are not clear. The mechanisms might be both biological and psychosocial. Based on our data of the five components that define metabolic syndrome, high waist circumference and low HDL were significantly more prevalent in women. Although the association between low HDL and HRQOL is less documented, the impact of obesity on HRQOL is well known. 27 –29 Ford et al. 27 showed a direct association between high body mass index (BMI) and poor HRQOL. In a discriminate analysis, Corica et al. 13 showed that among metabolic syndrome components, only BMI, blood pressure, and fasting plasma glucose were significantly correlated with poor physical HRQOL. Although Tsai et al. 30 showed an association between metabolic syndrome and physical HRQOL, that association was eliminated by controlling for BMI. There is limited information about the association between waist circumference and HRQOL. 31 In the present study, compared with men, high waist circumference was significantly more prevalent in women, and it is possible that the reduced HRQOL resulted from their greater waist circumference and not from metabolic syndrome as a whole. Despite these explanations, Oda et al. 32 reported stronger marginal correlation among cardiovascular risk factors in women than in men. According to their findings, the existence of one additional risk factor further increased the risk of CVD in women. In the present study, in women but not in men, the number of metabolic syndrome components was negatively associated with the physical domain of HRQOL, which is in line with another study conducted in Australia 33 and might reflect the cumulative effect of metabolic syndrome components on HRQOL in women. In our study, however, it was surprising that as the number of metabolic syndrome components increased, so did the scores on the PCS and the MCS in men. More studies to clarify this result seem necessary.
In addition to these biological explanations, gender psychosocial differences could be important. Compared with men, women's poorer psychosocial adjustment in relation to CVD has been reported in previous studies, which leads to different social perception, evaluation, and HRQOL in women. 26 There is limited knowledge about psychological adjustment in relation to metabolic syndrome, but as it is a precursor to CVD, the outcome would be much the same. To support this hypothesis, additional research will be needed.
This study has both strengths and limitations. We studied a large sample of nondiabetic adults in the general population, which enabled us to make direct comparisons between men and women. To our knowledge, there is no previous report on the association between HRQOL and the metabolic syndrome in Middle Eastern countries. Thus, the findings of the present study may help to better estimate the worldwide burden of this syndrome. This study was cross-sectional, and we were unable to draw conclusions about the causal association between metabolic syndrome and HRQOL. There are also too many confounders that could affect HRQOL; hence, the observed association between metabolic syndrome and HRQOL might be a result of unmeasured variables.
Conclusions
The study results show that metabolic syndrome was associated with poor physical HRQOL in women but not in men. Additional studies are required to clarify such findings.
Footnotes
Acknowledgments
This study is funded by the Obesity Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran. We acknowledge the assistance of Mrs. Niufar Shiva in preparation and editing of the manuscript and also express appreciation to the participants of the Tehran Lipid and Glucose Study.
Disclosure Statement
The authors have no conflicts of interest to report.