
Abstract
Aims:
Urinary incontinence (UI) is common among women in the United States and worldwide. Although the biomedical model for female UI has been thoroughly examined, the cultural model women living with UI ascribe to has been less well described. The purpose of this study was to elicit salient features of a cultural model for long-term (>5 years) female UI and, in so doing, increase understanding of the conceptualization of female UI from an emic (patient-derived) perspective. Cultural models theory provided the overall framework for the study.
Methods:
Freelist (n = 25) and pilesort (n = 13) exercises were completed by community-dwelling women with long-term UI. In the freelist exercise, participants listed 81 unique terms in response to the request: Please list all the terms you think of when you hear the phrase urinary incontinence. The most salient terms included: wet, embarrassed, diapers/pads, leakage, old age, urinate, annoyance, inconvenience. We then used the most culturally salient items from the freelist in three pilesort tasks.
Results:
Results of the pilesort exercises suggest that some aspects of the cultural model are shared, whereas others are highly heterogeneous.
Conclusions:
A small core of salient emic terms reflects a shared cultural understanding of female UI. The cultural model includes emotional and physical elements. These findings are important in reframing and reexamining our understanding of female UI. Next steps include testing the cultural model by including salient terms used by women living with long-term UI in focus groups and clinical encounters.
Introduction
Female urinary incontinence (UI) is highly prevalent in the United States and worldwide. 1 –4 UI increases the risk of institutionalization, has a negative impact on quality of life (QOL), and is also one of the most costly health conditions in terms of the financial burden it imposes on individuals and society. 4 –7 Risk factors and common etiologies have been identified, and numerous behavioral, medical, and surgical options have been tested and found effective for management and treatment of female UI. 8
The emic, or insider, patient perspective for female UI, however, has not been as thoroughly discussed; moreover, quantitative studies focused primarily on treatment options may not be able to fully address women's issues and needs regarding UI. For example, despite a wide variety of effective therapies for overactive bladder (OAB), stress UI, and urge UI, less than half of community-dwelling women seek professional care. 9,10 Although some factors thought to influence care-seeking behaviors have been identified (e.g., the degree of bother, embarrassment, belief that UI is normal for women 10 –13 ), this topic continues to concern and be of interest to researchers and healthcare providers.
This study was designed as a beginning step in increasing appreciation and understanding of female UI from an emic perspective. Further clarification of the cultural model women living with UI ascribe to may, in turn, lead to further development of sensitive and useful treatment strategies for this common and often devastating condition.
Cultural models and female UI
A search of the years 2000–2008 in Medline, PubMed, and CINAHL using the terms “female urinary incontinence,” “cultural models,” “patient perspective,” and “explanatory models” identified one reference regarding women's beliefs about UI. 14 Findings suggest that knowledge and beliefs about UI affect care seeking and, in the United States, often lead women to self-care therapies (e.g., purchasing and using absorbent products, devising timed fluid intake and voiding patterns) as a primary management strategy. 14 Women (mean age 47) in this study also reported a belief that UI is a normal consequence of aging and childbirth and that UI poses a problem for most women. 14
Two recent articles focusing specifically on female UI and cultural models 8,15 were identified in the literature search. Before these studies, Mitteness and Barker 16 described a cultural model for UI in older men and women. In this model, lay beliefs and biomedical knowledge form a shared model of what everyone knows about geriatric UI. It seems, however, that the cultural model constructed by laywomen living with UI is significantly different from the model to which most healthcare providers ascribe. 8 Components of the lay model include a lack of authority (or agency) where UI is understood as an inevitable female condition. This is in direct contrast to the professional, biomedical model in which healthcare providers and advertised UI treatments are represented as having the ability, power, and authority to fix UI. 8
Middle-aged women have also described a shared cultural model where UI requires concealment to preserve self-identity, is normalized, and, thus, is seen as part of the “biography of a woman's body.” 15 Finally, studies have examined the lived experience of female UI by exploring areas including women's beliefs about the etiology of UI 11 ; the impact of UI on QOL 17 ; the meaning of female UI in community settings, 18 in long-term care settings, 19 and for older women living with UI 20 ; and the experience of UI complicated by other chronic health disorders, such as multiple sclerosis. 21 Together, these studies provide a beginning examination of cultural models and the emic experience of living with female UI.
Study aims
Specific aims of this study were to (1) elicit and analyze the features of a cultural model for long-term (defined as >5 years' duration) female UI by identifying both the salient features of UI and how women categorize those features and, in so doing (2) increase understanding of female UI from the point of view of women who experience UI.
Theoretical framework
Cultural models theory, derived from the field of cognitive anthropology (CA), provided the overall framework for the study. In cultural models theory, cognitive schemas are learned by individuals as a result of exposure to external and interpersonal stimuli and are affected by life experiences and memories. 22 Cultural models are shared cultural schemas and are implicitly understood by members of the community. They rest upon a definition of culture as information that people need to know to get along as a member of a community. 23 Cultural models theory is relevant for this study, as women are likely to have both individual and shared experiences as a result of and associated with long-term UI. Thus, cultural models theory and CA provided a framework for answering questions about how individuals, in this case women with long-term UI, construct models that inform their lives. 24,25
Materials and Methods
Study overview
We used freelisting and pilesorting to identify shared common beliefs about UI among women experiencing UI in order to describe the features of a cultural model for long-term female UI. Freelisting and pilesorting are formal methods that can be used to identify the shared elements that comprise a cultural model for a given domain. 26,27 Anthropologists commonly define culture as those ways of acting in and thinking about the world that are socially shared and transmitted within a group of people. 26 Freelisting and pilesorting provide systematic methods for identifying which ideas are shared among a group of people with similar experiences.
Freelisting is a technique in which informants are asked to compile a list of items defining the cultural domain. 28 The information derived is particularly important because it reveals an emic, insider view of the cultural domain and allows researchers to identify culturally relevant information and determine saliency, importance, and familiarity of the specific items elicited. 29 These items jointly refer to a conceptual entity (i.e., a cultural domain) and, as such, may help in identifying components of a cultural model. 28 –30 As freelisting elicits information about the cultural domain from multiple people, it reveals individual as well as shared perceptions; it is possible to identify coherent domains with a sample of at least 20–30 informants. 28,31 Pilesorting can be used to extend the results of freelisting to identify how people categorize items within the identified cultural domain. The culturally salient items generated in the freelist exercise are written onto cards that participants are asked to sort into piles of similar items. Sorting is based on the similarity or dissimilarity of items on the cards, which in turn, identifies the socially shared structure of the cultural domain defined through freelists. 28,29
This study was reviewed and approved by the University of Pennsylvania Institutional Review Board. Study aims, methods, risks, and benefits were thoroughly explained to potential participants before study enrollment. Signed informed consent was obtained from each participant.
Study sample
Recruitment strategies for both the freelist and pilesort exercises included distributing fliers at a variety of target sites (e.g., outpatient primary care and specialty care clinical offices, churches, senior centers, women's centers) inviting women to contact the investigator and, if eligible and willing, to participate in the study. Inclusion criteria for both the freelist and pilesort exercises were long-term UI, residence in the city or immediate suburbs in which the study was being carried out, English as a first language, and commitment to the project until completion. 32,33
Freelist data were collected over a 9-month period. A total of 28 women responded to recruitment efforts; 2 were excluded because they did not speak English as a first language, and 1 decided not to participate after learning more details of the study. The final sample for the freelist exercise consisted of 25 women. Once freelist data collection was completed, participants were subsequently recruited for the pilesort exercise between January and December 2006. Although it is not necessary to have the same participants for both exercises, 28,29,34 –36 an effort was made to use as many of the same women for both exercises if they were available and willing to do so; therefore, 7 of the participants completed both the freelist and pilesort exercises. In total, 15 women were screened for the pilesort exercise; 1 did not meet inclusion criteria because she was acutely ill and unable to complete the study, and another declined participation because she did not want the investigator to interview her at home and did not have access to transportation to meet at an alternate location. Each participant who completed a freelist or pilesort exercise received a $20 thank you honorarium.
Data collection
After consenting to participate and completing descriptive data, individual freelist participants (n = 25) met one-on-one with the investigator in a convenient location (in most cases, the participant's own home) and were instructed to recall and write down all words that came to mind when hearing the phrase “urinary incontinence.” The choice of the phrase “urinary incontinence” was deliberate because this is a term often used by healthcare providers and found in media representations of female UI. 8 Our aim in choosing this term was to examine how the study participants responded to this phrase and to identify the lay terms participants associated with urinary incontinence. For each participant, the elicited terms were documented individually in order of occurrence, as the order in which terms appear is important for analysis. 28,37 Results from the freelist exercise were completed and analyzed before initiation of the pilesort exercise.
Next, the 22 most salient items from the freelisting exercise were recorded on individual index cards. Women who consented to participate in the pilesort exercise (n = 13) also met with the investigator individually in a convenient location (e.g., their own home, a local library quiet room, a neighborhood coffee shop). Cards were shuffled and given to each pilesort participant with the terms face up. Participants were asked to sort the cards according to three different prompts: (1) Sort these terms into 4 piles of items that you think go together, (2) Sort these terms into two piles, one with words that describe your own UI and a second pile with words that you would not use to describe your own UI, and (3) Sort these terms according to how much (some, a lot, not at all) your UI bothers you. The pilesort exercise took approximately 30 minutes to complete, and the content of each pile was individually recorded on paper. In addition, because pilesort exercises tend to foster conversation about informants' choices in sorting the information, 29 conversation during the pilesort exercise was audiotaped (with permission) for subsequent analysis.
Data analysis
We cleaned the freelists so that multiple words with very similar meaning appeared as the same word (e.g., annoyance and nuisance were both entered as annoyance) and entered them into Anthropac© 4.0 software,
35
then used Anthropac to calculate a salience index (Smith's S) for each item mentioned by participants, indicating how salient that item was to the group of participants (cultural saliency). For each word, Anthropac calculates a Smith's S using the formula:
where L = the length of each list, Rj is the rank of item J in the list, and N = the number of lists in the sample. 28 Items mentioned by more people and earlier on their lists are considered more culturally salient. Using a previously published approach, words from each list were sorted from high to low salience, and a scree plot was generated with salience scores on the y axis. 31,38,39 The plots were then inspected to select a natural breaking point, indicated by a flattening of the slope as words became less frequent. Terms that fell above the breaking point were retained as salient.
Pilesort responses were also analyzed using Anthropac to determine, as a group, how participants tend to divide up the domain of UI, using words suggested in the freelists. First, we used a standard measure of similarity 35 to create an item-by-item proximity matrix in which the proximity (similarity) of each pair of items is calculated based on the proportion of participants who sorted them into the same pile. 35,40 By measuring the frequencies with which participants sorted pairs of items together, we sought to discover whether or not women's evaluations of items were patterned by shared categories of UI characteristics. Next, to identify patterns in how participants sorted items, we created a graphic depiction of the proximity matrix by using the nonmetric multidimensional scaling (MDS) function in Anthropac. 35,37 MDS is a method of analysis used to graphically depict the ways participants classify items within a domain; items closer together in two-dimensional space were grouped together by more people than items further apart on the graph. 41
MDS graphs were generated to find an optimal configuration of points in a two-dimensional space. 41 Goodness-of-fit of each MDS graph to the data was established by stress levels below the acceptable cutoff. A stress level of ≤0.293 (measured in Anthropac) is considered acceptable fit for 22 items in two dimensions because this stress level occurs only 1% of the time for random matrices. 42 Thus, the lower the stress level, the better fit for the data and the less likely the results occurred by chance.
Results
Sample characteristics
Demographic and continence characteristics of the freelist and pilesort participants are shown in Tables 1 and 2. Two participants who completed the freelist exercise reported UI for 4 years; all other participants in both the freelist and pilesort exercises reported ≥5 years of living with UI. In general, most participants were middle to older aged and self-reported their race as white (particularly those who completed the pilesort exercise). We noted a wide range of responses to background UI data, such as the number of episodes of UI per week, the number of years with UI, and past or current UI treatments.
AA, African American; PME, pelvic muscle exercises; SD, standard deviation; UI, urinary incontinence; W, white.
Salient terms related to UI
All 25 freelist participants were able to respond to the question: Please list all the terms you think of when you hear the phrase urinary incontinence by writing down a list of terms they equated with UI. In total, participants listed 81 unique terms. The 22 most salient terms (from most to least salient) are listed in Table 3. Wet was a highly salient concept for the women who participated in the freelist exercise; other salient terms included embarrassed, diapers/pads, leakage, old age, urinate, annoyance, and inconvenience.
Percent of respondents mentioning the term on their freelist.
Smith's salience score, calculated by Anthropac using the formula: S = ((Σ(L − Rj + 1))/L)/N, where L = the length of each list, Rj is the rank of item J in the list, and N = the number of lists in the sample.
Similarities and differences among items in the cultural domain of UI
Task 1: Description and structure of UI domain
In pilesort task 1, in which participants were asked to sort the terms into piles that go together, two distinct clusters emerged (along the right and left sides of the graph) (Fig. 1) located in close proximity but with no overlap. Inconvenience, annoyance, uncomfortable, frustration, wish I didn't have it, embarrassed, and shame cluster together and seem to represent the embodied or emotional effects of UI as experienced by women living with it. Interestingly, the terms within this cluster were also grouped in a top to bottom fashion, with those that might be considered minor (e.g., inconvenience) before more major items, such as embarrassed and shame. In contrast, run to bathroom, frequency, bathroom, urinate, coughing, more wash, no control, leakage, and odor seem to be better characterized as one participant noted, by the “physical things I deal with.” No control is located almost equidistant between what seem to be physical and emotional aspects of female UI. The MDS graph for this task (Fig. 1) again appears to be an accurate representation of how participants sorted the 22 items, as a stress level of 0.188 was achieved for this task.
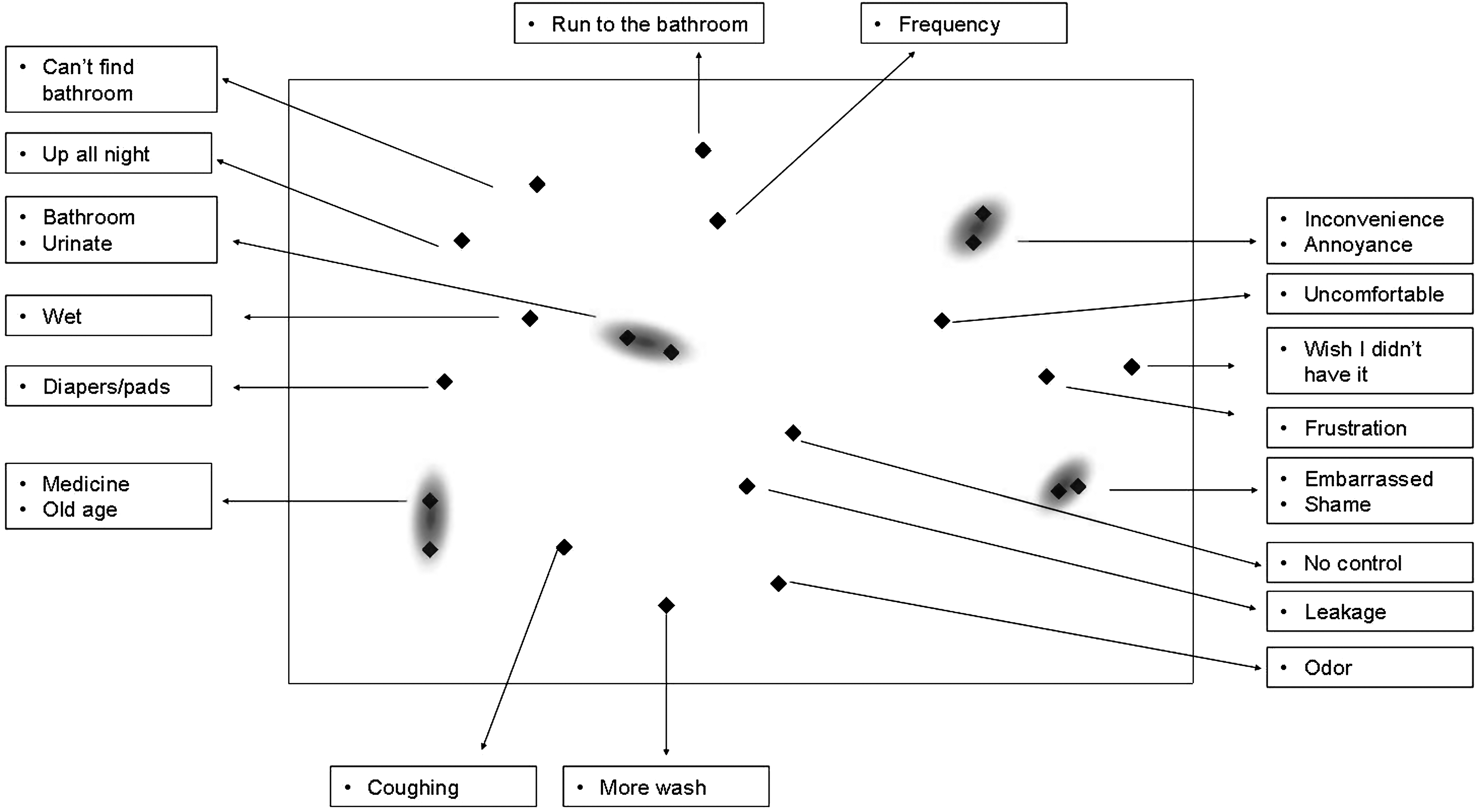
Description and structure of urinary incontince (UI) domain. During the first pilesort task, participants were asked to sort words into four piles of items that go together. The layout of the words represents the lay categorization of the UI domain. The items appear classified roughly into emotional features (right) and physical features (left).
Task 2: Terms that describe your UI
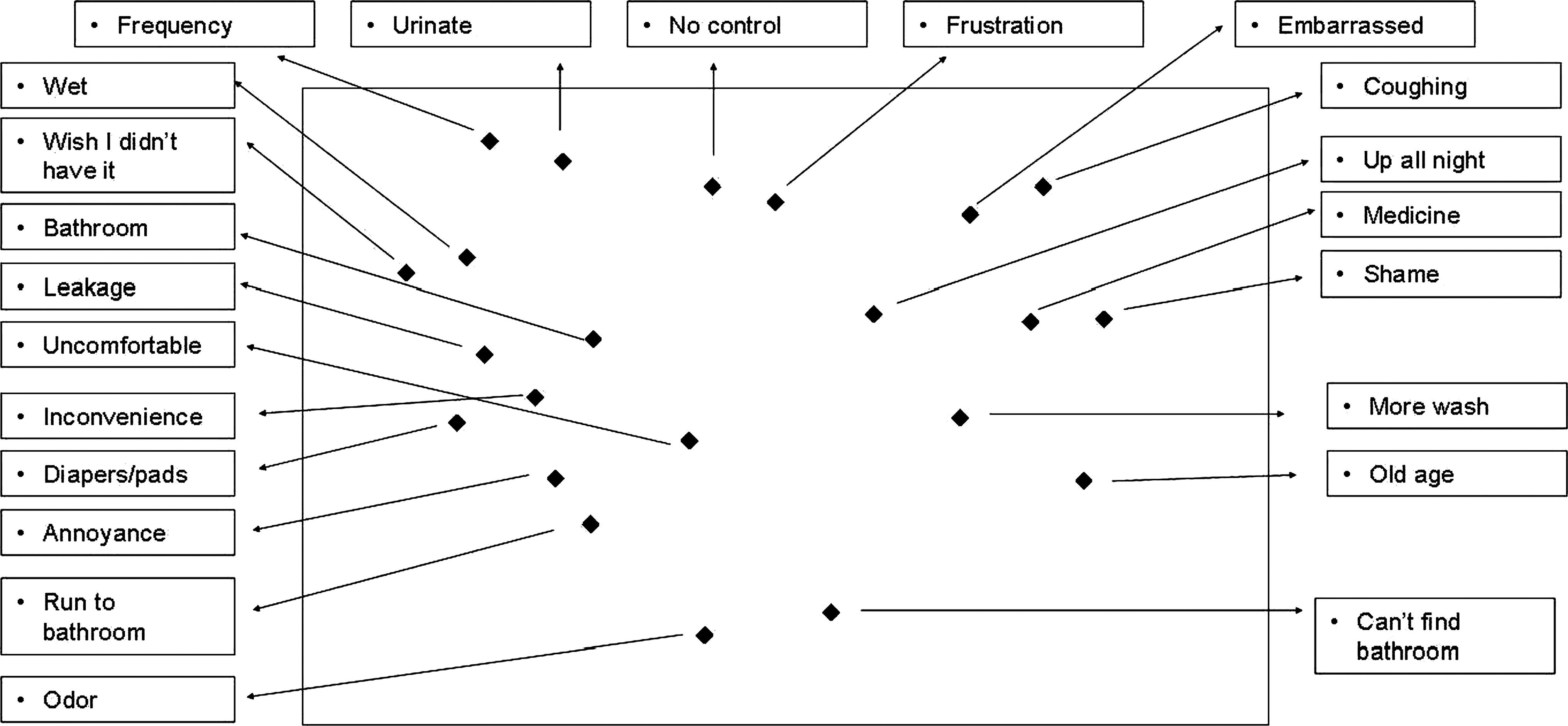
For the second pilesort task, participants were asked to separate items into two piles: words that describe their experience of UI and words that do not describe their UI. Three distinct clusters suggest that the cultural domain of long-term female UI experience consists of three major groupings of the terms elicited from the freelists (Fig. 2): (A) embarrassed, odor, and no control, (B) leakage, more wash, and uncomfortable, (C) wet, urinate, annoyance, inconvenience, wish I didn't have it, bathroom, run to bathroom, and frequency. Although coughing and shame are close to cluster A, it is not clear that they are part of the group. Additional terms depicted in Figure 2 (can't find bathroom, up all night, old age, medicine, diapers/pads) are located much further on the outskirts of the graph and likely represent conditions that are not universal or folded into the mainstream cultural model for long-term female UI. The MDS achieved a stress level of 0.138, well under the ideal of 0.293; thus, we believe Figure 2 accurately depicts how participants sorted the 22 most salient freelist terms for this task.

Terms that describe your UI. During the second pilesort task, participants were asked to sort words into two piles: words that describe their UI and words that do not describe their UI. Three primary clusters of items emerged through multidimensional scaling. The scattered items on the left side of the graph are located on the outskirts of the main clusters and likely represent conditions that are not universal or folded into the mainstream cultural model for long-term female UI.
Task 3: Degree of UI bother
In the third and final task, participants were instructed to sort the 22 most salient freelist items into three piles based on the degree of bother associated with each particular item. Figure 3 provides a graphic representation of participants' responses. Terms were scattered all over the MDS graph, with no clear clustering of the items. The stress level for pilesort task 3 was 0.149, again well below the ideal of 0.293. These results suggest that for women living with UI, there is very little degree of uniformity or agreement on just how much UI bothers them. For example, as one woman was completing this task, she commented that this bother issue reminds her of questions she is often asked at a variety of her health provider visits. She went on to cite an example of a recent ophthalmology appointment where she was asked: What is bothering you? However, as she is not a person who is bothered, the question does not make sense to her. She would much prefer that specific terms are used, for example: Does she have itching or blurred vision. She concluded by saying: If they [providers] do not use terms that make sense [to me], then I will not be able to tell them I have a problem!
Degree of bother associated with aspects of UI. During the third pilesort task, participants were asked to sort words according to the degree to which each aspect of UI bothered them (some, a lot, not at all). The scattered arrangement of items suggests that for women living with UI, there is very little degree of uniformity or agreement on just how much UI bothers them.
Study limitations
Even with our best efforts at achieving a diverse sample and a fair degree of success for the freelist task, participants who completed the pilesorts were heterogeneous in terms of their age, number of episodes of UI per week, number of years living with UI, and previous or current UI treatments but not in terms of their reported race or ethnicity. This limits the usefulness of these results for nonwhite women and should be addressed in future studies. Moreover, because of the relatively low sample size, particularly for the pilesort task, and the limitation that participants speak English as a first language, future studies should include a larger and more diverse sample. Despite these limitations, our findings provide a first step in developing and testing additional theories focused on cultural models for long-term female UI.
Discussion
This study demonstrates the relevance of freelisting and pilesorts to explore salient features of a cultural model for long-term female UI. Study findings also confirm key elements of previous research and add a new dimension, particularly to our understanding of an emic view of female UI. First, findings from the freelists suggest that a coherent shared cultural model of long-term UI exists among women with UI. Significant elements of the model include the terms wet, embarrassed, diapers/pads, leakage, old age, urinate, annoyance, and inconvenience. These findings build on and can be examined in light of previous research suggesting that women living with UI ascribe to a cultural model that is significantly different from the model healthcare providers identify with. 8 For example, other than urinate, salient terms identified by study participants reflect a lay understanding of UI rather than a biomedical perspective. Although this is not surprising, it is consistent with research examining other health conditions (e.g., colorectal cancer, human immunodeficiency virus) where participants found it difficult to understand or failed to include biomedical terms used routinely in clinical practice. 43,44 To address these concerns, salient elements of the cultural model should be considered for inclusion in UI screening tools or other instruments used to routinely obtain historical patient data. Moreover, office-based practices and continence programs in other settings need to be informed by and adapted to the cultural values of the women they serve. Finally, we recommend future studies comparing lay perspectives with terms generated by biomedical experts.
Interestingly, although old age appears to be a highly salient element of the cultural model of UI (Table 3), the terms normal or part of aging were not listed by study participants, and during the second pilesort task, the term old age did not cluster with any others when participants were asked to sort the piles in response to the question: Which words would you use to describe your urinary incontinence? It may be that many women, even those who might be categorized as old chronologically, do not see this term as one that applies to or describes their own personal experience with UI. Moreover, it is unclear if our findings reflect the significant amount of outreach completed over the course of many years to help providers and patients understand that UI is not a consequence of normal aging 45,46 or is a result of other factors, such as age differences of the respondents. Although our study design did not allow for comparisons based on participants' ages, future studies could incorporate such items in a design using freelists to compare younger vs. older women. 31 It might also be that differences in how our study participants responded were based on other demographic or continence characteristics, such as the number of years with UI or the number of episodes of UI per week. Our study design did not allow for collection of additional quantitative data about these characteristics or analyses comparing specific continence characteristics to freelist or pilesort responses. Describing how or if the cultural model relates to specific continence characteristics is another possible area for future investigation.
Another important dimension of the cultural model suggests that UI is both a physical and an emotional condition and that emotional aspects are further differentiated as minor or major issues by women. This supports previous research regarding the multifactorial nature of female UI in terms of both the etiologies and the impact on women's lives. 11,47 Additional physical elements of the model, such as up all night and can't find the bathroom, are also consistent with more extreme conditions or those occurring for only a subset of women, such as those with primary or isolated OAB. Clinicians need to recognize that their own cultural knowledge and values, as well as the terminology they use, often differ significantly from those of the patients they care for. 48,49 This, in turn, may compound other reasons why women are reluctant to discuss UI with others, such as embarrassment, the idea that UI is normal, or a perceived lack of providers' priority for evaluating or treating UI. 9,50,51 Freelists have been used to examine these types of cultural differences among patients, faculty, and medical residents 48 ; we believe this is a promising area for future research focused on women with long-term UI and the healthcare providers they are most likely to encounter, including primary and specialty care clinicians.
Finally, based on our findings, bother appears to be a very heterogeneous and individual aspect of long-term UI for women. In the third pilesort task, no uniformity or agreement about the degree of bother associated with salient terms identified in the freelist exercise occurred. Thus, it seems that not all women are bothered by the same elements of the cultural model. This may be another area where participants' responses were affected by other continence characteristics, such as the type of UI; therefore, we recommend this as an additional area for further investigation. Our finding regarding the heterogeneity of bother is not surprising based on our clinical experiences where, for example, women with very similar objective findings (e.g., results of bladder diaries, pad tests, or urodynamic studies) have diverse subjective complaints and when specifically questioned about how bothersome their UI is, describe a wide range of responses. Although reliable and valid quantitative instruments have been developed to accurately measure the degree of bother associated with female UI, 52 –54 we suggest exercising caution in using these instruments. Some women, such as those whose cultural model does not include bother as a salient element of their life experience with UI, may fall through the cracks and, in turn, not be referred for evaluation and care or seek advice from healthcare providers unless alternative or complementary methods are used to assess continence care needs. Moreover, these women may experience negative consequences that are not captured by existing scales that primarily seek to quantify QOL or the degree of bother. The addition of an open-ended question to identify an emic description of how UI affects an individual woman or including a list of salient elements based on the female cultural model for long-term UI in instruments that assess QOL and bother may provide essential data for clinicians as well as in future research.
Conclusions
This study shows that freelisting and pilesorting are useful methods for exploring women's experiences with long-term UI from the perspective of women who are experiencing the condition. In general, the shared model includes emotional and physical aspects. Although some of the specific elements of the model are shared, other elements are highly heterogeneous. Further testing of the cultural model should include using the salient terms identified here in focus groups with patients as well as with healthcare providers and in comparison with existing quantitative instruments commonly used in research and practice settings.
Footnotes
Acknowledgments
This work was funded by the John A. Hartford Foundation. The authors thank all the participants who generously shared their time and ideas, as well as Carolyn Sampselle, Ph.D., R.N.C., FAAN, for her careful manuscript review.
Disclosure Statement
The authors have no conflicts of interest to report.