
Abstract
Objective:
To identify and recruit an unknown and presumably small subgroup of survivors, that is, lesbian or bisexual women with breast cancer.
Methods:
This report describes our multistep approach to recruit a representative sample of heterosexual and sexual minority breast cancer survivors. We used census data to identify geographic areas with a greater prevalence of sexual minority women (SMW), that is, lesbian and bisexual women. We then obtained the breast cancer cases from a cancer registry for these geographic areas. In the absence of sexual orientation data in cancer registries, all potentially eligible women with breast cancer needed to be contacted by telephone to determine their sexual orientation.
Results:
Among the 1341 women screened who answered the question about sexual orientation, 6.3% were SMW. Overall, we processed 4143 cases to obtain completed data on 69 SMW and 257 heterosexual women with breast cancer.
Conclusions:
Our findings suggest that it is resource intensive but feasible to recruit a representative sample of breast cancer survivors of different sexual orientations. Our findings can inform future studies that seek to recruit sexual minority populations from cancer registries about some of the limitations to this approach.
Introduction
There are over 2.5
If one assumes the number of SMW among breast cancer survivors is equivalent to the number of SMW in the general population, recruiting a representative subset of breast cancer survivors who are SMW will be extremely difficult. This exacerbates the already well-recognized recruitment challenges of cancer survivors, who are difficult to identify and recruit for research. 6 Cancer survivorship research, including on SMW, has often relied on convenience samples. However, convenience samples are not well positioned to confidently assess disparities in survivorship due to sexual orientation. Only population-based cancer registry data will allow scientists to accurately determine the extent to which there are disparities in survivorship by sexual orientation.
The use of cancer registry data for recruitment of survivors is recognized as the gold standard because it avoids selection biases that may arise when individuals are recruited from the community or a single treatment site. Instead, a representative sample recruited from a registry allows for generalization to the larger population. A registry-based study design is a necessary first step toward the identification and understanding of assumed disparities due to sexual orientation. 2,3 We used this study design to recruit a representative sample of sexual minority and heterosexual breast cancer survivors. Here we document the recruitment yield and highlight the challenges we encountered.
Materials and Methods
All aspects of the study were approved by both the Boston University and the Massachusetts Department of Public Health Institutional Review Board (IRB).
Study setting
We used Census 2000 data about female same-sex partnered households, a frequently used proxy for sexual orientation. 7 Census data provide information on the geographic locations of female same-sex partnered households. Massachusetts is the state with the fourth highest concentration of female same-sex partnered households in the United States. 7 Despite this concentration, the overall prevalence is still low, in that only 0.56% of women in Massachusetts live in such a household. The density of same-sex partnered households varies considerably, from some cities or towns reporting 0 female same-sex partnered households to a high of >1000 households in Massachusetts' largest city, Boston. We restricted recruitment to 146 cities and towns in Massachusetts that had a high density of SMW, which we defined as 0.50% or more of the female population residing in a female same-sex household. Forty-four percent of the state's female population lives in these geographic areas, and these areas comprise roughly 39% of the annual breast cancer cases in Massachusetts.
Registry data
From the Massachusetts Cancer Registry (MCR), we requested breast cancer cases diagnosed in women between January 1, 2000, and December 31, 2005, in the specified 146 cities and towns. We restricted cases to primary diagnoses of breast cancer staged as ductal carcinoma in situ (DCIS) or stages I–III and those assumed to be alive, according to a review of the death index. The MCR provided us with names and addresses as recorded at the time of diagnosis. The registry does not have telephone numbers and does not update contact information after diagnosis.
Similar to all registries that obtain data from patients' medical records, the MCR has no information on sexual orientation, which required us to collect primary data on sexual orientation. Because we expected fewer SMW than heterosexual women among the available cases, we developed a protocol to collect data from a maximum of 250 heterosexual women yet continue recruitment of SMW until we either exhausted all available cases or collected data from 250 SMW. To minimize the possibility of selection bias, all cases in the study sample were assigned a random number and then processed in the specified random order.
Recruitment process
Per MCR guidelines, we notified physicians listed in the registry of our intention to contact their patients about participating in a research study. Passive physician consent was assumed if a physician did not notify us within 2 weeks of any objections to contacting the patient. Only cases without a recorded physician or cases for which a physician's contact information could not be found were contacted for recruitment without prior passive physician consent.
We searched for cases' phone numbers and updated addresses in phone books and electronic databases. If we were unable to locate a phone number, we sent a letter to the address available from the registry explaining the study and inviting the woman to contact us about study participation. We sent a recruitment letter to all women for whom a telephone number was available that explained the purpose of the study, provided information about the means to opt out of the study, and announced that a member of the study team would call to screen for eligibility. One week after sending the letter, we initiated the first of a maximum of 10 call attempts, including three voice mail messages, to screen for eligibility.
The telephone screening occurred in a 5-minute phone call, during which we asked questions about cancer history and sexual orientation. Because the goal of this study was to assess quality of life in cancer survivors, we excluded women who reported a cancer recurrence or were currently receiving active cancer treatment, defined as surgery, radiation, and chemotherapy, because this likely would affect their current reports about quality of life. All survivors were asked about their sexual orientation using at least one of two questions. First, we asked about sexual identity, providing lesbian, heterosexual, bisexual, or other as answer choices. Only the 8.4% of women who could not be classified as heterosexual or sexual minority or those who refused to answer were asked a second question about their preferred gender for a sexual partner, providing the answer choices, men, women, or either. Women who refused to answer both questions or for whom a sexual orientation could not be determined
Eligible heterosexual women and SMW were invited to participate in a 35-minute telephone survey. Participants had the option to complete the survey immediately after the screening or to schedule the survey at a later time. We made up to five call attempts to complete the survey with participants.
Second recruitment strategy
To increase our sample size and for the purpose of understanding differences in a volunteer sample compared with a population-based sample, we explained at the end of the registry respondents' participation in the survey our interest in finding additional women for this study. Participants were asked if they knew other Massachusetts breast cancer survivors who may be interested in the study. SMW participants were explicitly asked about other SMW survivors. Each participant was asked to get permission before providing the study team with the contact information of potential participants. One week after the survey, we placed up to three phone calls to study participants to obtain the contact information for any breast cancer survivors suitable for the study.
Data collection
Data collection occurred in three phases. During the first phase from August 2007 to February 2008, we completed the predetermined maximum number of surveys with heterosexual women after processing 1222 cases. To conserve resources yet continue recruitment of SMW, we changed our invitation letter to state that we needed to screen all women, but only SMW would be invited to participate in the survey. Second, we decided to no longer send a recruitment letter to women whose marital status was recorded in the MCR as married or widowed. We decided against contacting married and widowed women to conserve resources, reasoning that we would not likely find SMW among them. This decision was supported by analyses of the data already collected. However, as of May 17, 2004, same-sex marriage was legalized in Massachusetts, and our sample included diagnoses from 2004 and 2005. To account for this, we identified 1417 married women whose diagnosis of breast cancer occurred on May 17, 2004, or later and compared the names and dates of birth to Massachusetts same-sex marriage records from May 17, 2004, to December 31, 2005. This review resulted in the identification of 4 women who had a recorded same-sex marriage. These 4 cases were processed for recruitment into the study. The second phase of data collection was from June 2008 to August 2008, during which time we processed 2595 cases. By August 2008, 15 complaints had been made about this study to the MCR, the Boston University IRB, or the study principal investigator (PI). Because of these complaints, the Boston University IRB required us to temporarily suspend our study activities, allowing us only to follow up with 46 women who had already consented to the survey. The third and final recruitment phase was from October 2008, when the IRB suspension was lifted, through November 2008. During this final phase, we processed all 404 remaining cases in the sample.
Measures
Demographic and clinical data were obtained from the MCR, which cancer registrars derived from patients' medical records. We used age at diagnosis; race/ethnicity categorized into white, black, Latino, and other; and marital status categorized into married, never married, separated or divorced, widowed, and unknown status. The clinical information consisted of year of diagnosis and tumor stage. Contact attempts reflected the number of phone contact attempts until disposition of each case was determined.
Analysis
We calculated descriptive statistics on the telephone calls we placed to each subset of the population. We tested for differences in demographic and clinical characteristics, using t tests and chi-square tests. These analyses involved comparing subsets of women to the remaining women in the population.
Results
Figure 1 indicates that our population consisted of 11,112 cases from the MCR that were identified for this study. As explained, once we reached our recruitment goal of heterosexual women, we did not attempt to recruit (n = 6,842) married and widowed women, presuming that, if asked, they would report being heterosexual. In addition, 36 women were ineligible because the physician refused consent, and 91 were deceased. This resulted in 4,143 available cases for recruitment. We were unable to contact 40.1%; this included women whose recruitment letters were returned, women for whom we had no or a nonworking phone number; and nonresponders to a follow-up letter requesting they contact us. Eleven percent could not be reached after 10 call attempts, and 4.9% made use of the opt-out option provided in our recruitment letter. Upon contact, 10.5% refused to be screened for the study. We screened 33.1% for eligibility, of whom 6.0% screened ineligible. Among those who screened eligible, 1.6% subsequently refused the survey, and 0.7% refused to answer the questions about sexual orientation or it could not be assessed. This reduced our sample to 24.8% of those screened for eligibility. Among those eligible, our attempts to administer the survey resulted in 0.5% who exceeded the number of calls for interview completion. Per the study protocol, we did not attempt to complete an interview with 16.5% eligible participants because they self-reported as heterosexual after we had already enrolled sufficient numbers of heterosexual women. As a result, we completed 326 of the 345 (94.5%) interviews attempted. Therefore, we had an overall American Association for Public Opinion Research (AAPOR 1) response rate of 25.9%, a contact rate of 28.3%, and a cooperation rate of 91.4%. However, our approach resulted in completed interviews with only 7.9% of the 4,143 cases available for recruitment, 6.2% with heterosexual women and 1.7% with SMW.
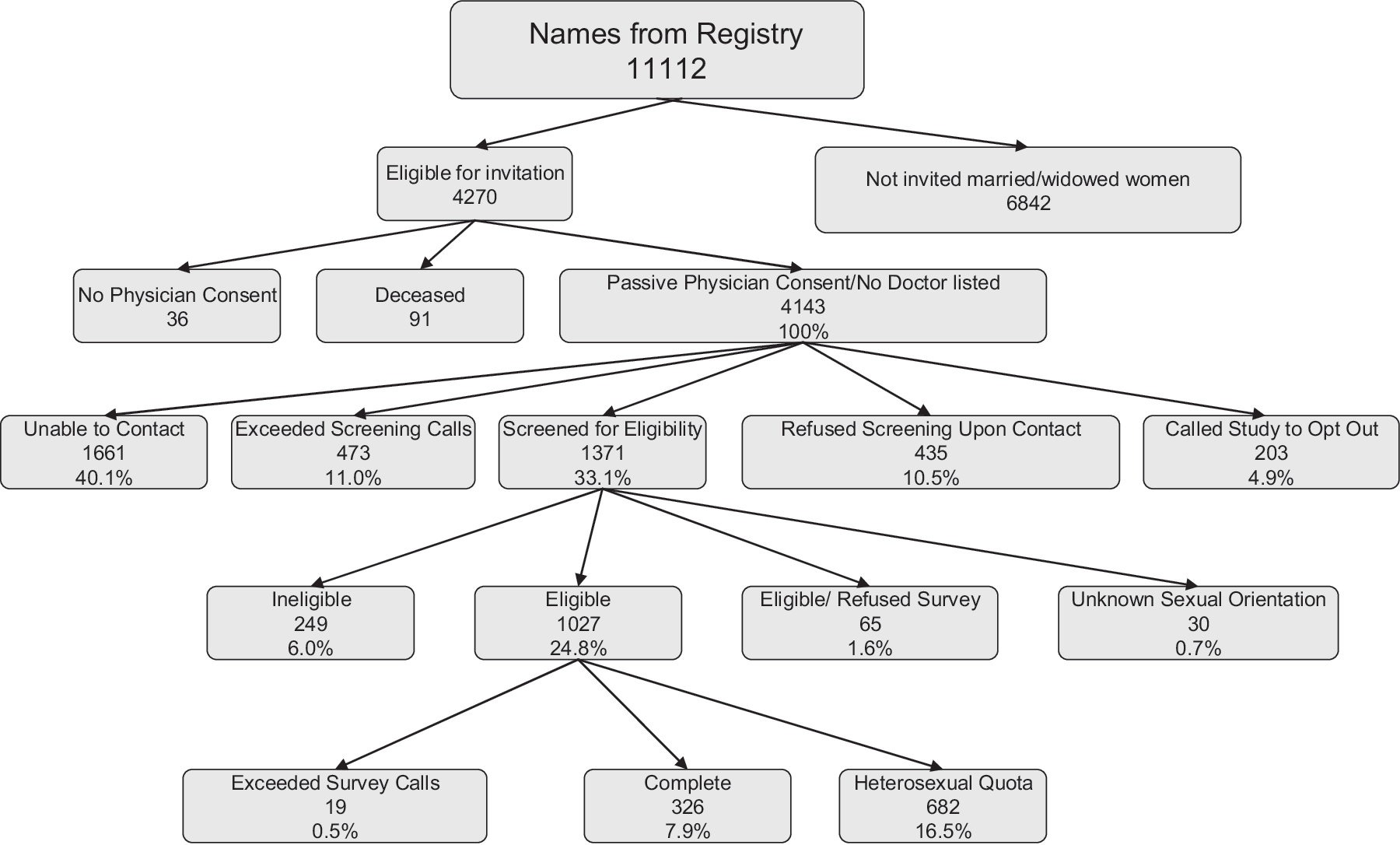
Recruitment of breast cancer survivors using cancer registry data.
Table 1 indicates the median, mean, and confidence intervals (CIs) for the telephone calls by disposition of cases. The number of calls is an indication of the resources spent. Until eligibility had been determined through screening, we placed up to an average of 4.1 calls per case. It is noteworthy that we needed to place significantly more calls to complete the survey with eligible SMW than with heterosexual women.
CI, confidence interval.
Table 2 shows the demographic and clinical characteristics of the entire population of 11,112 cases and the characteristics for each stratum in our recruitment process. As shown in column 2, on average, the population was almost 60 years old, 87% were white, and more than half were married. The population was evenly distributed across the six diagnosis years, and two thirds of the population was diagnosed with DCIS or stage I. We then compared each subset to the overall population to identify differences with respect to age, race/ethnicity, marital status, and the year and the stage at diagnosis. Because marital status was the determining criterion for being classified as having reached quota (column 3), these women significantly differed from the population on this aspect. Women who were not invited to participate were also older, more were white, and fewer were diagnosed with stage II. Compared with the population of cases, women who were unable to be contacted (column 4), were significantly younger, more likely to be black or Latina, more likely to be single, separated or divorced, and had a later stage at diagnosis. The women whom we were unable to screen because they exceeded the number of calls (column 5) were significantly younger, more likely to be black, and more likely to be single or separated compared with the overall population. Women who opted out of the study (column 6) differed from the population only on age and marital status; they were significantly older and fewer were married. Those who refused our invitation to be screened (column 7) were older, more likely to be white, and more likely to be single or separated. The women we did screen (last column) were younger and more likely to be white, and fewer were married compared with the population.
Each p value compares a subset to the overall population of column 2.
DCIS, ductal carcinoma in situ.
Table 3 continues our comparisons of subgroups of women to the overall population with regard to the recruitment process. Women who screened ineligible were significantly older, fewer were white, and fewer were married. Women who screened eligible and answered the sexual orientation questions were younger, more were white, and more than twice as many were single or separated compared with the population. Women who refused to answer the sexual orientation questions were significantly older than the population, and fewer were married. Women who were screened but not invited for the survey because we had already reached our goal of heterosexual women (e.g., quota) were significantly younger, white, and single and less likely to have been diagnosed in 2000. Eligible women who exceeded the number of calls to reach them for the survey did not differ from the overall population. Women who refused the survey differed only from the population with respect to age, in that they were significantly older. The interviewed heterosexual women were significantly younger, more were white or black, and more were married compared with the population. The interviewed SMW women were significantly younger, less likely to be married, and more likely to be diagnosed with DCIS than the overall population. There were no significant differences with respect to race or year of diagnosis between SMW and the population.
Each p value compares a subset to the overall population of column 2.
SMW, sexual minority women.
Table 4 shows the yield we achieved after asking participants to refer other suitable women with breast cancer to our study. Almost 60% of the heterosexual women reported not knowing others, and more than two thirds of the interviewed SMW reported not knowing SMW with breast cancer. Less than 10% of participants were willing and able to provide us with referrals for other suitable women with breast cancer.
Discussion
To our knowledge this is the first registry-based study with the goal of obtaining a representative sample of breast cancer survivors of different sexual orientations. Our systematic approach to obtaining participants of different sexual orientations indicates how labor intensive it is to recruit the rare population of SMW from a cancer registry. We processed 4143 cases to obtain completed data on 69 SMW.
Of particular interest for this study is the evaluation of recruitment success with respect to the identification and participation of SMW. Because sexual orientation is not recorded in registry data, we can only report on the proportion of SMW among the 1341 women we screened and from whom we obtained answers about their sexual orientation. The proportion of SMW was 6.3%, which represents 84 SMW we were able to identify, even though subsequently only 69 of them completed the survey. Whether this percentage is low or an accurate account of the true proportion of SMW among breast cancer survivors is unclear.
The possibly biggest challenge of this study, and where we assume the biggest loss of SMW occurred, was the high number of survivors (40.1%) we were unable to contact. Locating and contacting survivors using registry data that record only contact information at diagnosis are widely recognized problems in survivorship research. 8 In our study, survivors who were unable to be contacted were younger; more likely to be black or Latina; more likely to be single, separated, or divorced; and had a later stage at diagnosis compared with the population. Similarly, survivors who exceeded the number of call attempts for screening were also more likely to be younger, black, Latina, and single, separated, or divorced. These subgroups represent the more mobile and harder to reach populations in this study. We assume that within these subgroups there are also a number of SMW with whom we never made contact.
We have several indications that SMW may not have been particularly motivated to participate in our study. For example, we needed to place significantly more calls to complete a survey with SMW, possibly suggesting these women were not particularly keen on participating. The same pattern existed when we attempted to obtain referrals from SMW; >20% could not be reached to obtain names of other suitable SMW with breast cancer. Alternatively, it may indicate that SMW lead busier lives than heterosexual women, making it harder to reach SMW by phone. We identified 84 SMW, 75 were eligible, but we were only able to complete interviews with 69. Our experiences also suggest that information about the study reached SMW, but they chose not to participate. For example, we hypothesize that a number of SMW were in the group of women who exceeded their calls because of interviewers' reports of reaching answering machines that gave two women's names. We reason that if SMW were highly motivated to participate in this study, they would have initiated contact with us by responding to the invitation letter or voice messages left about the study. Further, we believe that SMW were among the group of women whom we could never call because we could not find a phone number for them, despite using the multiple common approaches for locating study participants. For this reason, we sent letters to women for whom we had no phone numbers, requesting they contact us about this study. A small number of women responded to this invitation, but none of them were SMW, which again led us to conclude that SMW may not have been highly motivated to participate in this study.
One possible consideration is that the means we used of recruiting SMW through a cancer registry are not favorable for the participation of this population. It is plausible that receiving a letter that indicates they were identified through the MCR and then announces our intention to ask about their sexual orientation is not conducive to gaining the cooperation of this population. A number of registry studies reported that some cancer survivors are unaware of the existence of cancer registries and perceive contact for research purposes as an invasion of privacy, 6,9,10 concerns that may be heightened for SMW when the recruitment letter announces questions about cancer and sexual orientation. Because we needed to recruit women of different sexual orientation for later comparative analyses, our options for building trust and for presenting the study as beneficial for SMW were limited.
Because this study included determination of participants' sexual orientation, the Boston University IRB was worried about privacy issues. Over the course of the study, we informed or contacted 4143 patients about this study and received 15 complaints, which equals 0.36% of cases, that caused a temporary suspension of the study by the Boston University IRB. There was some variation in the causes for the complaints. Two thirds of complaints were about privacy concerns, in that survivors lacked the awareness that cancer is a reportable disease. These complainants assumed that the recruitment letter sent by the PI of this study represented a Health Insurance Portability and Accountability Act (HIPAA) violation. Other complaints were also consistent with problems that occur when contacting survivors through cancer registries, such as upsetting a family member of an individual who was recently deceased or encountering a respondent who was under the impression that she did not have cancer. Less than one third of the complaints about this study were explicitly linked to the study's goal of recruiting women of diverse sexual orientations. Among those sexual orientation-related complaints were religious objections to the study and feeling upset because it was perceived the study's only concern was for lesbians and their partners. Another cause for complaint was the perception that sexual orientation is equivalent to sexuality and the anticipation of being asked in detail about sexual activity. This was perceived as insensitive, given the toll the invasive cancer treatments took on sexuality. In spite of these specific complaints about this study's emphasis on survivors of different sexual orientations, the amount of complaints we received in response to the study was consistent or below the number of complaints to be expected, as documented by a review of 33 registries that allow researchers to contact cases following strict procedures, as we did in this study. 9 Overall, the majority of complaints are consistent with other research studies that involve cancer registries and the tension between survivors' rights for privacy and confidentiality and the public's interest in surveillance. 6,9,10
Given these multiple challenges, one has to critically evaluate the yield of SMW after using this registry-based approach. One possible explanation for the yield of SMW is that our study eligibility criteria were biased against SMW. We set out to conduct a study of healthy survivors, which is why we restricted this study to women with a primary diagnosis of breast cancer, without metastatic cancer or recurrence. A number of studies that focused on cancer screening of SMW suggest that they have less mammography 11,12 and less access to healthcare because they are less likely to have health insurance. 13 The SMW we recruited in this study had earlier disease compared with the population of breast cancer survivors. It is conceivable that our selection criteria inadvertently excluded SMW, who are less engaged in screening and are, therefore, diagnosed with later stage disease, who are more likely to undergo less aggressive treatment, or who have other factors that make them more likely to have metastatic disease, a second cancer, or cancer recurrence. This implies the selected SMW may be women who are actively connected to healthcare and participate in screening and medical treatment and, as a result, were in a better position to achieve healthy survivorship.
The participating SMW were also younger compared with the population of cases, which may suggest another selection bias. Multiple explanations for the differences in age are possible. SMW may be less prevalent in older cohorts, and there may be more hesitation among older cohorts to self-disclose as SMW in research. Another possibility is a difference in the mean age of breast cancer diagnosis between SMW and heterosexual women because of different risk profiles. Although the race of SMW was not significantly different from that of the population, our yield of racial minority SMW with breast cancer was low. This is most likely because breast cancer occurs more frequently in white women than in racial minority women.
For example, the population from which we recruited was 87% white. This raises some questions about whether the approach we took is suitable for racial minority SMW. We suggest that the same recruitment strategy may be more successful if it is implemented in a more racially diverse population. For example, recruitment of African American SMW with colorectal cancer may be more successful because African American women have a higher incidence of colorectal cancer compared with white women. All of these concerns speak to limitations and possible selection biases in the recruited SMW. However, only cancer surveillance data that include sexual orientation will allow us to resolve these questions and facilitate a possibly less selective sample of SMW with breast cancer.
Given these multiple challenges and the yield of SMW after using this registry-based approach, one may question whether there are alternatives for finding breast cancer survivors of different sexual orientations. Although recruitment of nonprobability samples from clinics or the community appears less resource intensive, they are, on the other hand, not suitable for answering questions about disparities because they are not representative of the population of survivors. Paramount questions about the existence of disparities in cancer treatments, which ultimately impact cancer recurrence and mortality, demand representative samples of different sexual orientations. As a possible alternative for finding a representative sample of breast cancer survivors of different sexual orientations, one may think of respondent-driven sampling (RDS), which has been presented as advantageous in that it shares the advantages of probability samples for allowing researchers to obtain unbiased estimates. 14 However, RDS is dependent on the connectedness of the population, a condition that is not necessarily met by lesbian, gay, and bisexual populations. 15 From our findings with respect to obtaining referrals from participants, we can conclude that breast cancer survivors are not well connected, which precludes the successful use of RDS in this population. Until sexual orientation data are included in surveillance systems, 1 future research will either need to follow our resource-intensive model of recruiting a representative population or retreat to nonrepresentative community samples, which can provide information about the perspectives of survivors but do not allow for generalizability.
Despite these limitations, this study has considerable strengths. For example, we demonstrated that it is possible to collect data on sexual orientation from women of all ages. We successfully used registry data to recruit a rare population, which is novel and can inform other researchers who may wish to use this strategy to find sexual minorities with cancers other than breast. Finally, the methodological rigor with which this study obtained a population-based sample of breast cancer survivors of all sexual orientations allows us to use the collected data to address the issue of disparities in the cancer burden as a result of sexual orientation.
Footnotes
Acknowledgments
Support for this research was provided by the American Cancer Society, grant RSGT-06-135-01-CPPB PI (U. B.). We are grateful to the participants who took the time to respond to our questions and complete the survey.
Disclosure Statement
The authors have no conflicts of interest to report.