
Abstract
Aim:
To determine if a defined set of echocardiographic parameters at entry and exit of a longitudinal study over 5 years showed changes with aging.
Methods:
The cohort consisted of 484 randomly recruited women aged 40–80. They were examined by two echocardiography cardiologists, independent of the medical information for these women.
Results:
Across the age decades (40–49, 50–59, 60–69, 70–79 years), body weight and body surface area (BSA) did not vary, and diastolic blood pressure (DBP) was stable; systolic blood pressure (SBP) progressively increased. There was gradual decline in left ventricular (LV) diastolic function, increase in LV muscle mass, and decrease in LV end-diastolic volume (LVEDV). The serial decrease in rate of change over 5 years in ejection fraction (ET) was small but significant across the four age decades.
Conclusions:
As expected, there were age-related changes in cardiac structure and function over time in women who showed no apparent cardiovascular disease (CVD) at entry to the study. The direction of these serial changes was toward the development of LV stiffness and likelihood of subsequent heart failure. The clinical significance of the decrease in rate of change in EF remains unclear.
Introduction
With the prediction that by 2051, 28.5% of women will be aged >65—from 13.9% in 2002 1 —there is increasing interest in characterizing the effects of aging on cardiovascular health in structure and function. 2 Several changes have been reported in longitudinal studies, including heart rate and variability, 3 blood pressure (BP), 4 electrical conduction, 5 and ventricular wall thickening. 6 Heart failure has been described as the most common cause of hospital admissions in the elderly. 7 The contribution of genetic factors to cardiac aging has been estimated to vary from 17% to 69% on left ventricular mass (LVM). 8 Studies have shown a higher prevalence of diastolic dysfunction than systolic dysfunction in the elderly community and a predilection in men, but because these abnormalities were rare in the absence of such known risk factors as hypertension, coronary artery disease (CAD), and LV hypertrophy, it is speculated that diastolic heart failure may be preventable. 9 In population samples, up to 27.3% of women were found to show diastolic dysfunction, which had a strong association with an NT-probrain natriuretic peptide. 10
In light of these concerns, we used serial echocardiography in a cohort of women aged 40–80 years who were randomly recruited from an urban population as part of a large longitudinal study to evaluate the rate of change in various parameters of heart function. The objectives of the study were to determine if there were differences in a defined set of echocardiographic measurements in the age groups and, in particular, their rate of change over 5 years in paired datasets.
Materials and Methods
Study cohort
The women were participants of a multidisciplinary evaluation of aging in the age group 40–80, the Longitudinal Assessment of Aging in Women (LAW) Study. Design, recruitment, and retention strategies have been described previously. 11 The women identified from the electoral roll of a district in a major city entered the study by invitation and by a process of random sampling after approval by the Human Research Ethics Committee of a major teaching hospital (Royal Brisbane and Women's Hospital). Individual consent was obtained from the women.
The women were evaluated by a preset number of tests, which included echocardiography. They were assessed in year 1 and year 5 of the continuing study by two experienced cardiologists. A total of 511 women entered the study, 27 were excluded because of a history of cardiovascular disease (CVD), and the remaining 484 women were evaluated. Of the 484 women, 222 had used hormone therapy; 82 were past users and 140 were current users at entry to the study, and during the 5-year study, 108 stopped therapy after 2 years when the findings from the Women's Health Initiative (WHI) were announced in 2002.
Technique
Echocardiography data on each woman were obtained using Acuson Sequoia cardiac ultrasound equipment (Siemens, Mountainview, CA). Two-dimensional echocardiographic views were obtained from the parasternal, apical subcostal, and suprasternal windows. Aortic, mitral, and tricuspid Doppler studies were obtained using steerable and nonimaging modalities.
LV volumes (LVV) and ejection fractions (EFs) using the Simpson's method standard M-mode dimensions were obtained following the American Society of Echocardiologists (ASE) criteria. LVM was calculated using the modified ASA formula from M-mode. Stroke volume (SV) was calculated from pulsed wave (PW) Doppler of the LV outflow tract.
Color M-mode and Doppler tissue imaging assessment of diastolic function was undertaken in all cases. Doppler tissue imaging myocardial velocity (E′) was measured in this study from the interventricular septum. This was standard at the time of acquisition of these data. The time constant of ventricular relaxation (tau) was calculated from the isovolumic relaxation time (IVRT) and the systolic systemic blood pressure (SBP) and an estimated left atrial pressure (LAP) of 10 mm Hg, using the formula:
All image data were stored in DICOM format using ProSolv archiving software (ProSolv Concepts, Indianapolis, IN) on digital linear tape for later review. Two intracardiac pressure parameters were measured. The transaortic gradients were assessed by continuous wave (CW) Doppler. Right ventricular (RV) systolic pressure was estimated by interrogation of the maximal tricuspid regurgitation velocity converted to gradient via the modified Bernoulli equation. This value was added to an estimation of right atrial pressure (RAP), with 10 mm Hg considered to be the norm, and higher values applied with hepatic vein (HV) plethora. This measurement represents the combined elements of LAP and transpulmonary flow gradients.
The echocardiographic studies were reported by very experienced cardiologists using state-of-the-art equipment of the time. To validate the new equipment that was acquired at the beginning of the digital echo era and when testing for the LAW Study began, acquisition protocols, sonographer training, and physician reporting methods were tested Studies of 20 patients were reviewed by the two specialist echocardiologists in the study, who were blinded to sonographer interpretation data. The digital loops of these 20 patient studies were then reviewed by seven other cardiologists, again blinded to other data. A grading score of 0–4 was given for global LV function (LVF), regional wall motion abnormalities (RWMA) by coronary distribution, and valvular regurgitation lesions. The following results on concordance were obtained: RWMA completely in 17 of 20 cases, within ± 0.5 grade point for mitral regurgitation in 16 of 20 cases, for aortic regurgitation in 18 of 20 cases, and for tricuspid regurgitation in 18 of 20 cases. The clinical accuracy of the studies was considered to be within the standards of routine cardiology practice. Clinical reports were issued to local medical teams. Recommendations for clinical follow-up of identified conditions were made as appropriate.
Analysis
The women were divided into four age decades for analysis based on their age at entry to the study as 40–49 years, 50–59 years, 60–69 years, and 70–79 years. Descriptive data were presented as mean ± standard deviation (SD) for each group. A test for significance of differences for paired measurements in each woman over 5 years was performed by standard t test.
Results
Baseline characteristics of cohort
Table 1 shows baseline characteristics according to the four age decades. There were 484 women included in the study, with nearly equal distribution among the four age groups, and 440 women were available for paired measurements over 5 years. At initial assessment in year 1, there were 27 women with known cardiac disease (CAD, cardiac failure, arrhythmia); they were excluded from the study. There were also 33 women who gave a history of hypertension and were receiving treatment; they were retained in the study as they were asymptomatic. During the 5-year study, new developments in cardiovascular health were found in 10 women with atrial fibrillation, 7 with ischemic heart disease, 4 with cardiomyopathy, 2 with aortic aneurysm, and 1 with pericardial effusion. All of them remained well compensated after surgery or medication.
ns, not significant, p > 0.05.
ANOVA, analysis of variance.
At entry, body weight and body surface area (BSA) did not vary across the decade groups. Surprisingly, there was no difference in body weight (mean 68–71 kg). Diastolic blood pressure (DBP) also was stable across the decade groups. In contrast, there was a progressive increase in SBP across the decade groups that was clinically and statistically significant. In the youngest decade cohort, the SBP was 116 ± 13 mm Hg; in the oldest decade cohort, the SBP rose to 142 ± 17 mm Hg.
Key two-dimensional echocardiographic data on entry to study
Table 2 shows the data according to the four age decades. The LV end-diastolic volume (LVEDV) decreased progressively with increasing age decade, from 106 ± 18 mL to 96 ± 19 mL (ANOVA, p < 0.001). Systolic function did not decrease with age decades; the EF remained stable between mean values of 68%–69%. There was also no decrease in systolic SV across the age decades. However, LV muscle mass increased slowly from 130 ± 29 g in the youngest age decade to 155 ± 40 g in the oldest age decade (p < 0.001).
ns, not significant, p > 0.05
LV diastolic function assessment parameters deteriorated across the decade groups, with isovolumic relaxation time, mitral deceleration time, and E:E′ ratio all increasing. The left atrial (LA) area increased with age (p = 0.015), consistent with progressively elevated chronic LA filling pressure. Although the Color M-mode propagation velocity (a useful load-independent measure of diastolic function) decreased with age, the change was not significant. Tau as a measure of ventricular stiffness was progressively prolonged from a mean value of 38 ms in the 40–49-year age decade to a mean value of 41.5 ms in the 70–79-year age decade (p = 0.039). The E:E′ ratio, which measured filling pressure of the LV, increased progressively from 6.6 ± 2.0 through 7.2 ± 2.1, 8.4 ± 2.6, to 10.6 ± 0.4 (p < 0.001).
At entry to the study, there was a small but significant increase in RV systolic pressure across the age decade (p < 0.001), from 28 mm Hg (±6.0) in the youngest group to 35 mm Hg (±6.0) in the oldest group. However, there was no significant change in the transaortic peak gradient, suggesting no clinically significant aortic stenosis evolving with aging in the cohort tested.
Change in LV structure and function
The rate of change over 5 year was evaluated by paired measurements in individual women in their age decades for EF of the heart (Fig. 1), LV systolic SV (Fig. 2), and LVM (Fig. 3). As shown in Figure 1, systolic function as measured by EF did not decrease across the age decades at entry to the study, at exit from the study, or as mean values of paired measurements over 5 years. However, there was a decrease within each age decade; this statistically significant change, however, was about 5%.
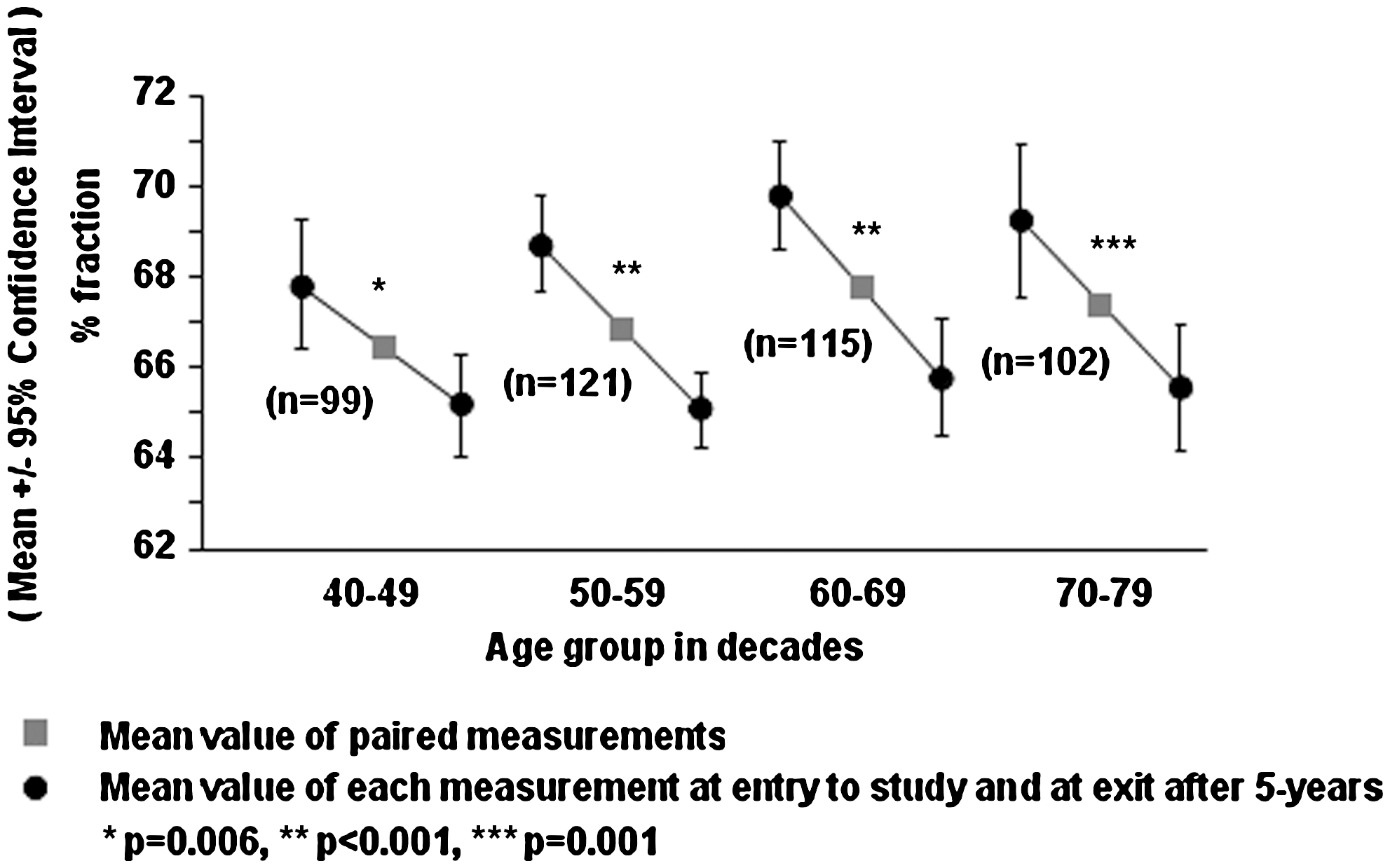
Rate of change in ejection fraction for paired measurements in each woman over 5 years.
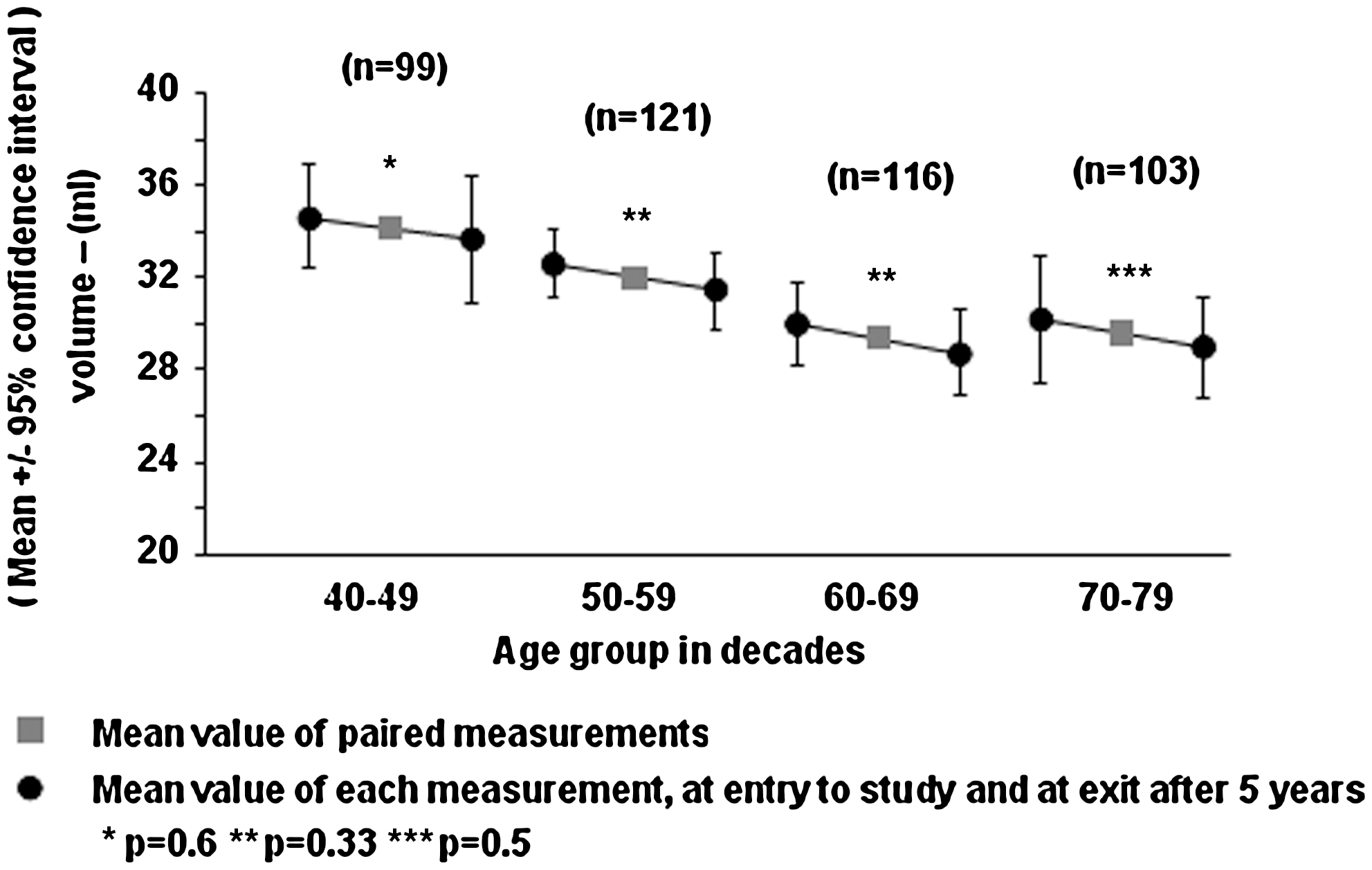
Rate of change in left ventricular systolic volume for paired measurements in each woman over 5 years.
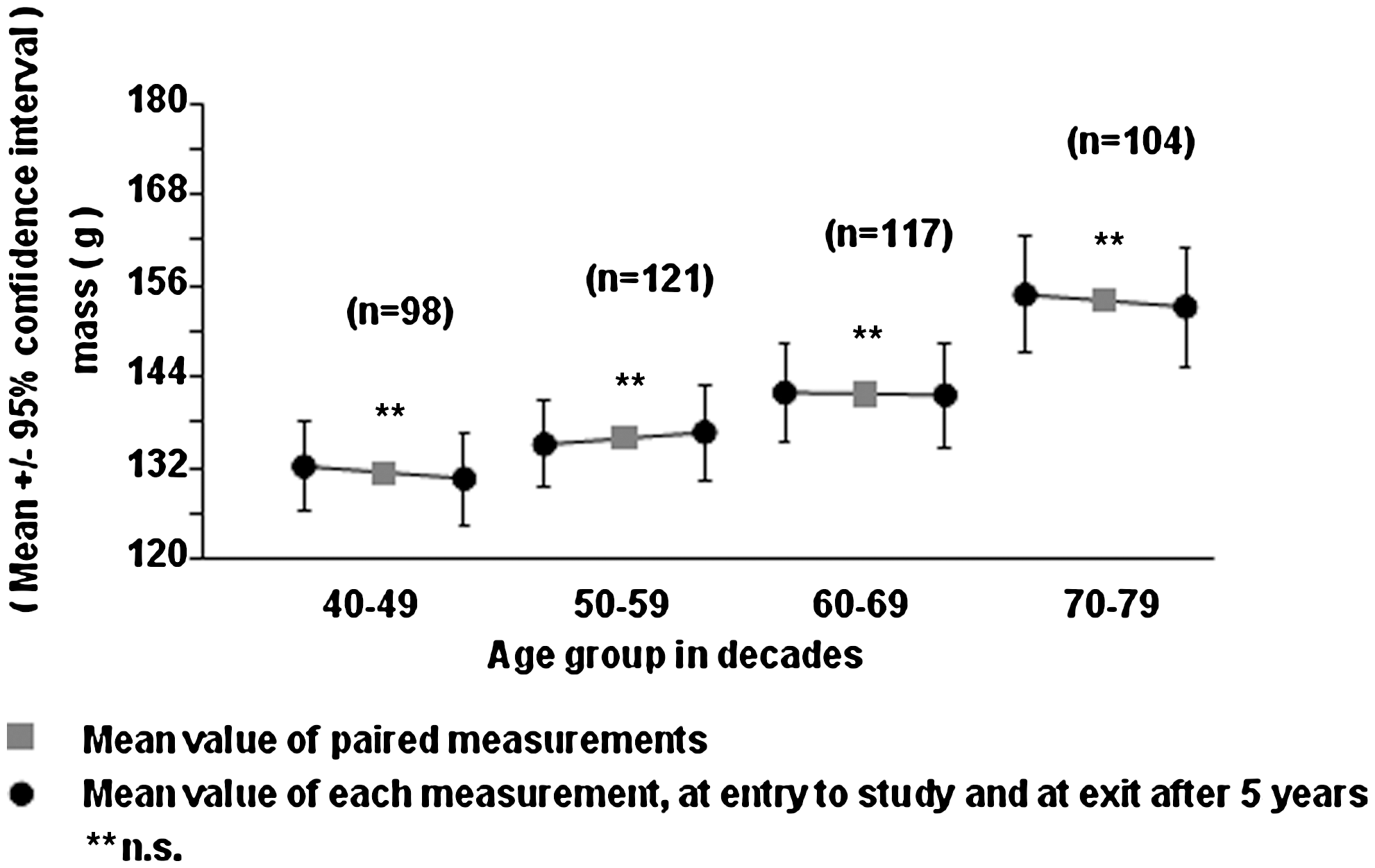
Rate of change in left ventricular mass for paired measurements in each woman over 5 years.
As a secondary marker of LV function, the systolic SV was also assessed (Fig. 2). There was a small and not significant decrease in volume, with each mean value approaching that of the next age decade. The decrease over 5 years was <5 mL within and between each age decade. As shown in Figure 3, there was a gradual and significant increase in LVM in mean values for each age decade (p < 0.001), although the difference over 5 years (between values at entry and at exit) was not discernible within each age decade.
Discussion
It is recognized that aging, even in the absence of disease, imposes multiple effects on cardiac function and structure. 13 One parameter that has been studied in a longitudinal population setting was heart rate and heart rate variability. The Whitehall Cohort Study showed differences between men and women 3 whereby men had higher sympathetic activity and women had higher parasympathetic activity, and the probability of an adverse effect was related to baseline exercise, body mass index (BMI), cholesterol, and BP.
In our study, we extended the evaluation of aging effects in a randomly recruited population setting confined to women within a defined age range using serial echocardiography. The validity of our dataset, especially for paired measurements, was enhanced by a high retention rate in the cohort after 5 years (95.5%). Further, cardiovascular developments in the cohort were infrequent over 5 years; only 22 women (4.5%) had clinical problems.
Because reports have indicated that the menopause with its loss of estrogen has an effect on LVF and LVV, it becomes important to characterize the additional effects of aging. We found that significant changes were not directly related to age decades when menopause occurs but were present progressively across all four age decades. These changes were predominantly in LV diastolic function, with decreases in isovolumic relaxation time, mitral deceleration time, and E:E′ ratio. These changes represent ventricular stiffness, and their relationship with advancing age would suggest that even in absence of apparent disease, aging is unfavorable to specific aspects of heart function, moreso in diastolic function than systolic function. This diastolic dysfunction will lead to secondary increases in ventricular filling pressure and volume and, subsequently, to increases in LA filling pressure to distend the LA and increase its area. As a result, an increase in end-diastolic pressure and filling will cause symptoms of pulmonary congestion and heart failure. We continue to monitor these patients for a clinical outcome.
Is it only diastolic dysfunction that is associated with healthy aging? There is evidence that systolic dysfunction may occur over time in hypertensive patients with diastolic dysfunction or diastolic heart failure. 14,15 Further, a segmental relaxation pattern was correlated with systolic dysfunction 16 in relation to LV hypertrophy, increase in SBP, and aging. We found that EF remained relatively unchanged across the age decades, and the change in individual paired measurements within the age decades was not substantial (<5%), albeit statistically significant.
Our findings on the rate of change of paired measurements in the cohort over 5 years are interesting. Although the rate of change in LV SV and LVM remained similar, the rate of change in the EF was small (<5% difference) but significant (with a decrease) in all four age decades. This raises the question of clinical significance, in the light that this finding was not observed in the cross-sectional data. Although the small difference may be explained by method error/reproducibility, it is unlikely because the difference was statistically significant across all age decades, and the measurements were made by the same experienced cardiologists with the same equipment and validated as described in Materials and Methods. Furthermore, to support the view that reproducibility is unlikely to be an issue, the parameters in question are routine Doppler measurements, which are less susceptible to poor reproducibility.
There appears to be a paradox in our findings on EF across age decades: a decrease over the 5-year longitudinal data and no such decrease at entry from the cross-sectional data. We believe that these changes may be too subtle to show up using the cross-sectional data. The longitudinal data based on paired testing of individual women allow for more power in the analysis to show these changes, especially when all the data move in the same direction. Although the change was small, the differences were found to be highly significant within all the age decades (p = 0.006, p < 0.001, p = 0.001, and p < 0.001 respectively). We suggest that these small decreases in EF over time are in keeping with the predictable decline in LV diastolic function, as evident by prolonged deceleration time, increase in isovolumetric time, and increased tau, and increase in the E:E′ ratio to compensate for the deteriorating LV diastolic relaxation so as to maintain cardiac output.
In conclusion, we were able to confirm that in a randomly recruited cohort of women who were apparently healthy at entry to the study, there were gradual echocardiographic changes in respect to LV diastolic dysfunction with aging.
Footnotes
Acknowledgments
We thank the LAW Study participants for their cooperation and willingness to be assessed in this ongoing longitudinal study. This study was supported by a grant from the Royal Brisbane and Women's Hospital Foundation.
Disclosure Statement
The authors have no conflicts of interest to report.