
Abstract
Objective:
We sought to evaluate differences in the stage at diagnosis and the survival of breast cancer patients enrolled in two different Medicare healthcare delivery systems: fee for service (FFS) and health maintenance organizations (HMO).
Methods:
We used a linkage of two national databases, the Medicare database from the Centers for Medicare and Medicaid Services (CMS), and the National Cancer Institute's (NCI) Surveillance, Epidemiology, and End Results (SEER) program database, to evaluate differences in demographic data, stage at diagnosis, and survival in patients with breast cancers over the period 1985–2001.
Results:
Medicare patients enrolled in HMOs were diagnosed at an earlier stage of diagnosis than FFS patients. HMO patients diagnosed with breast cancer had improved survival, and these differences remained even after controlling for potential confounders. Specifically, breast cancer patients enrolled in HMOs had 9% increased probability of survival (hazard ratio [HR] 0.91, 95% confidence interval [CI] 0.88-0.93) than their counterparts enrolled in FFS. These findings persisted even when patients had a cancer diagnosis before their breast cancer.
Conclusions:
Improved survival among breast cancer patients in HMOs compared with FFS is likely due to a combination of factors, including but not limited to earlier stage at the time of diagnosis.
Introduction
Two of the most common types of healthcare delivery systems in the United States are fee for service (FFS) and managed care systems (which include the health maintenance organizations [HMO]). Medicare's HMO program has grown rapidly in recent years; by 2000, >6.5 million persons were enrolled, which accounted for nearly 20% of the beneficiary population. 1,2 Managed care systems have been developed to contain healthcare costs, but their effect on quality of care has not been clearly established. 3,4 The healthcare delivery system in which a patient is enrolled has been associated with differences in the stage at diagnosis and in survival for several cancers, including melanoma and breast, cervical, and colorectal cancer. 5 –11
Breast cancer is the most common nonskin cancer among women in the United States and is second only to lung cancer as a cause of cancer-related death. 12 In 2009, an estimated 192,370 new cases of breast cancer were diagnosed, accounting for 27% of all new cancer diagnoses among American women. 12 One of every eight women will die of breast cancer. 12 Diagnosis at an earlier stage of breast cancer has been associated with longer survival, suggesting the role of screening in early detection. 13,14 It has been suggested that both routine screening and adjuvant therapy have reduced breast cancer mortality in the United States. 13 –15 The recent recommendation by the United States Preventive Services Task Force (USPSTF) to delay the onset of routine breast mammography from 40 years to 50 years of age has ignited a national debate on the utility and cost-effectiveness of breast cancer screening. 16,17 As discussions of healthcare reform continue, the effect of the healthcare delivery system will become increasingly significant in patient outcomes and cancer prevention.
Using national healthcare databases, the current study evaluated differences in the survival of breast cancer patients after diagnosis between the two Medicare healthcare delivery systems (FFS and HMO) over the period 1985–2001. We hypothesized that women in HMOs would be diagnosed at an earlier stage than their FFS counterparts, and this earlier finding would result in improved survival. Additionally, we hypothesized that patients with a prior diagnosis of any cancer might have increased participation in a healthcare delivery system, including breast cancer screening. We used a prior cancer diagnosis as a surrogate for active participation in a healthcare delivery system. Therefore, we also evaluated the role of prior cancer diagnosis, defined as breast cancer as a second cancer diagnosis, as a possible contributing factor to breast cancer stage at diagnosis and survival.
Materials and Methods
This study represents an analysis of the linkage of two national databases: the Medicare database from the Centers for Medicare and Medicaid Services (CMS) (formerly the Health Care Financing Administration [HCFA]) and the National Cancer Institute's (NCI) Surveillance, Epidemiology, and End Results (SEER) program database. 18 The linked database combining the SEER and Medicare data represents a large population-based source of information for cancer-related epidemiologic and health services research.
SEER data
The SEER program is an epidemiologic surveillance system sponsored by the NCI consisting of population-based tumor registries that routinely collect information on all newly diagnosed cancer (incident) cases that occur in people residing in SEER areas. 18 The information collected about each incident cancer diagnosis includes the patient's demographic characteristics, date of diagnosis, tumor data (e.g., histology, stage, and grade), treatment recommended or provided within 4 months of diagnosis, follow-up of vital status, and cause of death (if applicable).
SEER registries currently cover approximately 26% of the U.S. population, and U.S. cancer statistics are based on analyses from this program. SEER data are considered to be highly valid and are the gold standard with follow-up. 12,19 –25
Medicare data
Medicare is the primary health insurer for 97% of the U.S. population ≥65 years of age. 2,26,27 All Medicare beneficiaries receive Part A benefits, which cover inpatient care in short-stay and long-stay hospitals, skilled nursing facilities, home health, and hospice care. Ninety-five percent of beneficiaries also subscribe to Part B of Medicare to obtain benefits that cover physician services, outpatient care, durable medical equipment, and in some cases, home healthcare. Medicare, in a master enrollment file known as the Enrollment Database, maintains information about each beneficiary's enrollment and entitlement, demographics, and HMO membership. The Medicare enrollment files contain entitlement dates to Part A and Part B, ZIP code of residence, healthcare delivery type, and the months in which the beneficiary was enrolled in a Medicare HMO.
Data linkage
The linkage of the SEER and Medicare data is the result of the collaborative effort of the NCI, the SEER registries, and the CMS. 2,27 For each linked dataset, among persons in the SEER data who were ≥65 years, 94% were matched to the Medicare enrollment database. 2
Patient selection
We first selected all SEER incident cases of breast cancer in women aged ≥65 years diagnosed between 1985 and 2001 who were entitled to Medicare Part A and Part B (Medicare HMO) at the time of diagnosis and who were matched to the Medicare enrollment files. Demographic (age, race, and marital status) and cancer diagnostic information was obtained through SEER, and information on Medicare entitlement and use was obtained from Medicare enrollment records. Because of the lack of information on individual income and educational level, 1990 U.S. Census data were used as proxy measures. 28 The HMO indicators determined HMO status at the time of diagnosis. If a patient was indicated as not being a member of an HMO and the claim was processed by CMS, the patient was classified as a Medicare FFS user.
Cancer staging and survival
For staging of breast cancer, the NCI staging system was used based on the extent of disease at diagnosis as reported by the individual SEER registries. 18 These registries abstract information from a variety of sources, including inpatient hospital records, outpatient records, and pathology reports. The staging system consists of five tumor stages: in situ, local, regional, distant, and unknown stage. Cancer cases with an unknown stage were excluded from the analysis.
Data analysis
Student t tests for continuous variables and chi-square test for discrete variables were used to compare the demographic data, as well as the stage at diagnosis of breast cancer by HMO status. We then performed multivariate analysis using Cox proportional hazards models to determine if the HMO patients had better survival than the FFS patients. In the multivariate models, we adjusted for the stage at diagnosis, as well as a range of potential confounding factors reported in the literature with use of the SEER-Medicare database. 2,5 –11,28 The potential confounding variables adjusted for included age, race, marital status, and Census tract median income and educational level as proxy measures for socioeconomic status (SES). All analyses were performed using SAS Software (Cary, NC). The significance level was set at 0.05 for all tests.
Results
As shown in Table 1, we evaluated 130,336 women with primary breast cancer, of whom 109,000 were enrolled in FFS plans. Breast cancer patients enrolled in FFS were slightly older than HMO patients (mean ± standard deviation [SD] 74.9 ± 7.3 vs. 74.5 ± 6.5) (p < 0.01). The majority of breast cancer patients were non-Hispanic whites. White patients represented a larger percentage of patients with breast cancer in FFS than in HMO (88.5% vs. 83.4%) (p < 0.01)).
Column totals may not add up because of missing data.
FFS, fee for service; HMO, health maintenance organization; SD, standard deviation.
Compared to the HMO patients, FFS patients had a greater proportion from Census tracts with a median income <$20,000 (8.7% vs. 5.1%, p < 0.01) and with <30% of residents with a college education (70.2% vs. 67.4%, (p < 0.01). Patients with breast cancer enrolled in an HMO had a significantly higher proportion of being married at the time of diagnosis (46.6%) than the FFS patients (43.8%) (p < 0.01).
Primary breast cancer
HMO patients with breast cancer were more likely to be diagnosed at an early stage. For example, the proportion of those diagnosed at an in situ stage was 13.1% in HMO patients vs. 10.8% in FFS (p < 0.01). The proportion diagnosed at a local stage was 62.9% of HMO patients vs. 59.5% of FFS patients (p < 0.01). We also found using Kaplan-Meier survival analyses that breast cancer patients enrolled in HMOs had significantly better overall survival than FFS patients (p < 0.01) (Fig. 1). The comparisons of survival by stage at diagnosis for breast cancer revealed that HMO patients diagnosed at a local stage (p < 0.01), regional stage (p < 0.01), or distant stage (p < 0.01) had significantly improved survival than their FFS counterparts (Fig. 2).
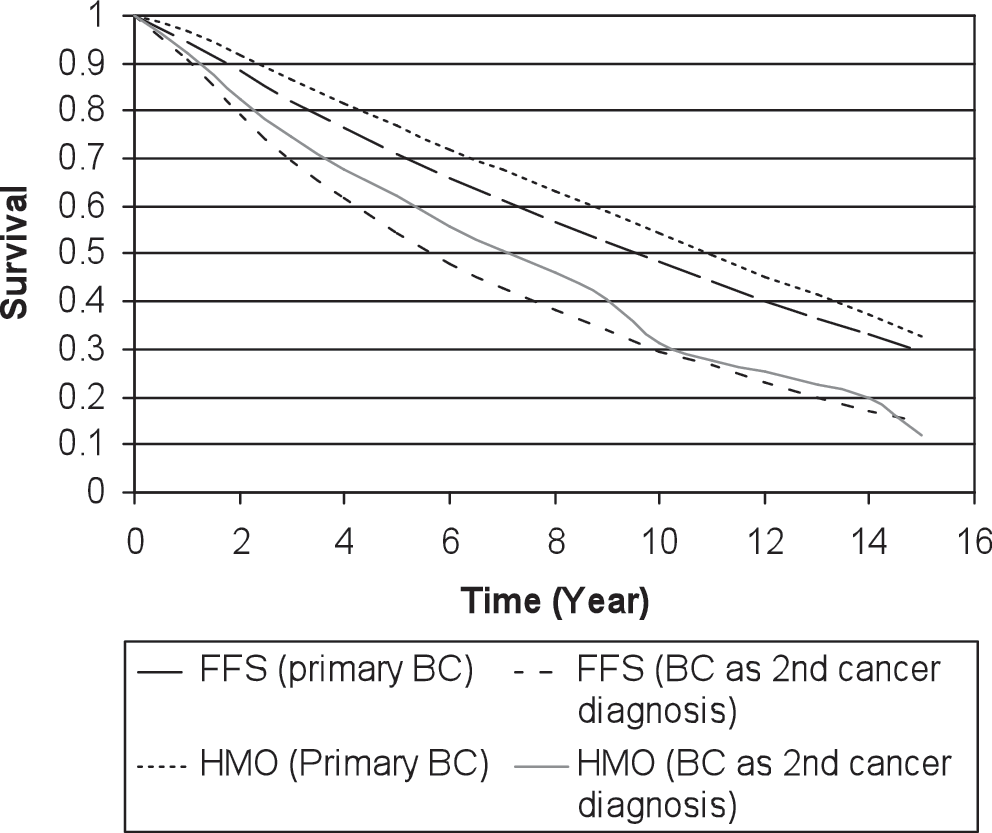
Kaplan-Meier survival curve for primary breast cancer (BC) or BC as the second cancer diagnosis, by HMO status. Log-rank test: p < 0.01 for primary breast cancer and p = 0.58 for breast cancer as the second cancer diagnosis. FFS, fee for service; HMO, health maintenance organization.
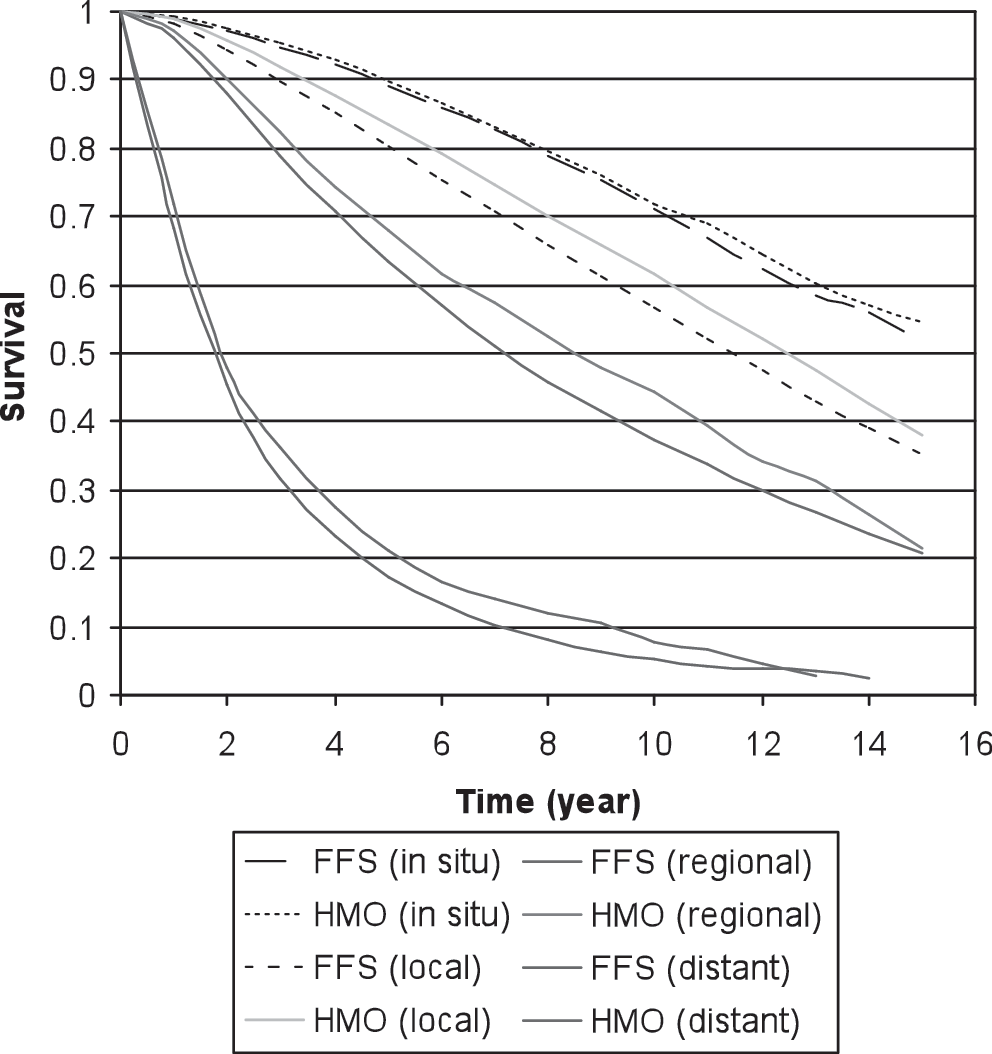
Kaplan-Meier survival curves for BC patients by stage at diagnosis and HMO status. Log-rank tests for equality of survival curves between HMO and FFS by stage at first diagnosis: in situ: p = 0.26; local: p < 0.01; regional: p < 0.01; distant: p < 0.01.
Multivariate analyses using Cox proportional hazards model were performed to evaluate the survival of HMO and FFS patients (Table 2). After initial adjustment for stage at diagnosis, patients with breast cancer enrolled in an HMO had a 14% significantly better survival than FFS patients (hazard ratio [HR] 0.86, 95% confidence interval [CI] 0.83-0.88). After further adjustment for potential confounding factors (i.e., age, race, marital status, Census tract income, and education), the improvements in survival among HMO patients were still significant with breast cancer (HR 0.91, 95% CI 0.88-0.93).
Included age, race, marital status, Census track income, and education.
Breast cancer as a second cancer diagnosis
Of the 130,336 women we studied with primary breast cancer, 6,933 had a previous cancer diagnosis before their breast cancer diagnosis. We chose to evaluate patients based on the order of breast cancer diagnosis (among other cancers) because we hypothesized that patients with a preexisting cancer diagnosis before their diagnosis of breast cancer were more likely to be actively followed in the healthcare delivery system in which they were enrolled. This, therefore, enabled us to evaluate the prior use of healthcare as a potential modifying variable of stage at diagnosis.
As shown in Table 1, breast cancer patients enrolled in FFS plans were slightly older than HMO patients (73.95 ± 6.4 vs. 72.9 ± 6.5) (p < 0.01). The majority of breast cancer patients were non-Hispanic whites. White patients represented a larger percentage of patients with breast cancer in FFS plans than in HMOs (91.1% vs. 87.1%) (p < 0.01). Compared with HMO patients, FFS patients had a greater proportion from Census tracts with a median income <$20,000 (9.4% vs. 5.2%), (p < 0.01) and with <30% of residents with a college education (69.2% vs. 61.8%) (p < 0.01). Patients with breast cancer enrolled in a HMOs had a significantly higher proportion of being married at the time of diagnosis (43.8%) than the FFS patients (34.7%) (p < 0.01). HMO patients with breast cancer as a second or later cancer diagnosis were more likely to be diagnosed at an early stage. For example, the proportion of those diagnosed at an in situ stage was 14.1% in HMO patients vs. 10.9% in FFS patients (p < 0.01).
Kaplan-Meier survival analyses showed that, overall, breast cancer patients enrolled in HMOs had similar survival to FFS patients (p = 0.58) (Fig. 3). At the same stage however, survival did differ; for example, HMO patients diagnosed at a local stage (p = 0.03) and regional stage (p = 0.02) had significantly improved survival over that of their FFS counterparts, but no statistical significance was found in survival for patients with distant stage disease between patients enrolled in FFS plans and those enrolled in HMOs (p = 0.16).
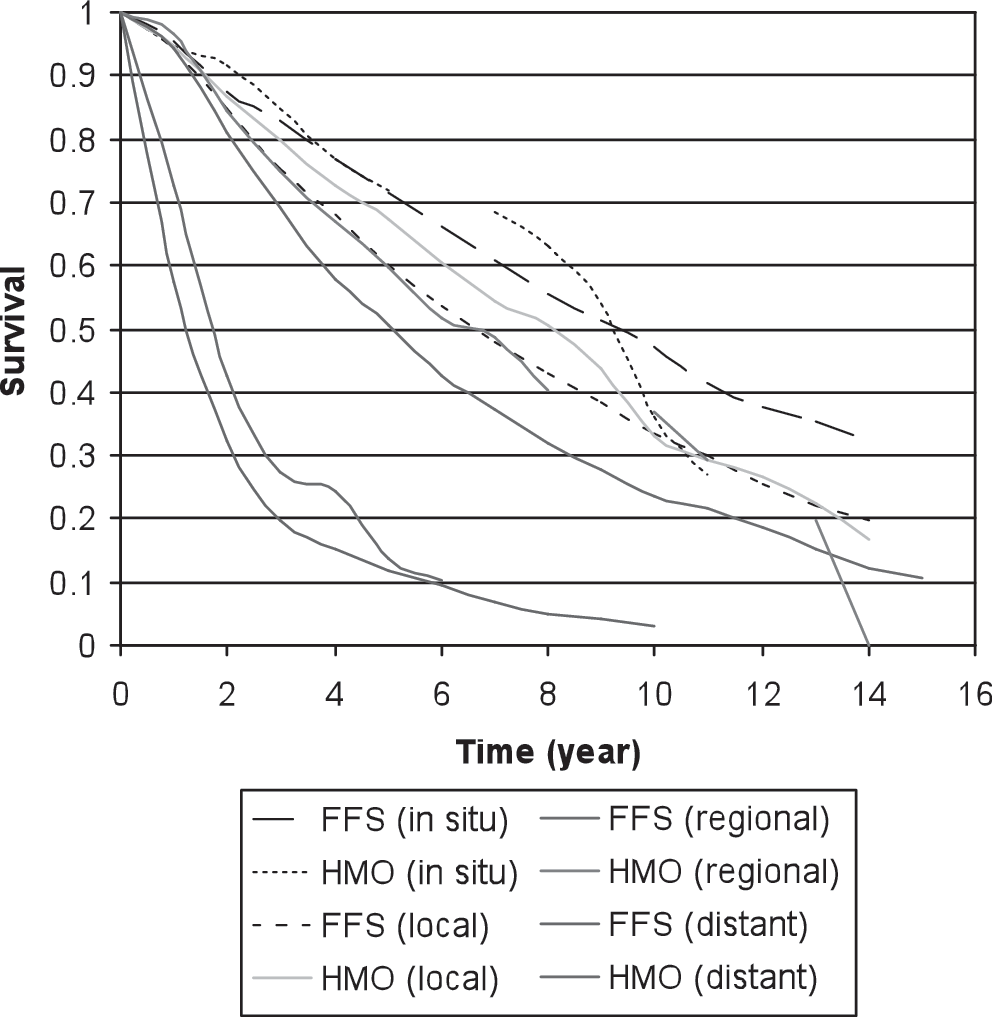
Kaplan-Meier survival curves for patients with BC as second cancer diagnosis by stage at diagnosis and HMO status. Log-rank tests for equality of survival curves between HMO and FFS by stage at first diagnosis: in situ: p = 0.68; local: p = 0.03; regional: p = 0.02; distant: p = 0.16.
Multivariate analyses using the Cox proportional hazards model were performed to evaluate the survival of breast cancer patients with a prior history of any cancer among the HMO and FFS patients. After initial adjustment for stage at diagnosis, patients with breast cancer enrolled in an HMO had a 16% better survival than FFS patients (HR 0.84, 95% CI 0.75-0.94). After further adjustment for potential confounding factors (i.e., age, race, marital status, Census tract income, and education), these improvements in survival among HMO patients with breast cancer persisted (HR 0.88, 95% CI 0.79-0.98).
Discussion
We found that Medicare patients enrolled in HMO healthcare delivery systems had greater survival when diagnosed with breast cancer, either as a first cancer diagnosis or subsequent cancer diagnosis, compared with patients enrolled in FFS systems. These differences remained even after controlling for potential confounders (such as stage at diagnosis, age, race, SES, and marital status). Specifically, primary breast cancer patients enrolled in HMOs had a 9% increased probability of survival over those enrolled in FFS plans. We also evaluated whether breast cancer being a second or later cancer diagnosis influenced stage at diagnosis and survival and found patients diagnosed with another cancer before the breast cancer diagnosis were more often diagnosed at an earlier stage of cancer and had an increased probability of survival, even after controlling for potential confounding variables.
In our study, breast cancer was diagnosed at earlier stages for patients enrolled in HMOs compared to FFS plans. For breast cancer, for example, 13.1% of HMO patients were diagnosed with in situ breast cancer compared with 10.8% of FFS patients. One explanation for these findings could be the phenomenon termed the “HMO effect.” This term has been used to describe the greater likelihood of HMO patients, compared with FFS patients, to use preventive services, including disease screening. 6 This effect could be related to either plan differences in the promotion of and access to preventive services or to qualitative differences among HMO patients in terms of education, income, or health consciousness. Differences in promotion or access to preventive services may exist. 25 –27 For example, differences in preventive health services have been found between different healthcare delivery systems and between the uninsured and the insured populations, as well as within racial and ethnic minorities. 26,27 In a survey of over 7500 patients, greater frequency of both clinical breast examination and Pap smear use was reported among HMO patients. 28 Others have found similar results in the use of screening tests among patients enrolled in different healthcare delivery systems. In one study, use of six different cancer screening tests (i.e., mammography, clinical breast examination, Pap smear, fecal occult blood test, and digital rectal examination) varied according to type of healthcare coverage. HMO enrollees at all ages were approximately 10% more likely to be screened than persons enrolled in private FFS plans. 10
For stage-specific diagnoses using the Kaplan-Meier statistic, as well as after controlling for stage at diagnosis, patients enrolled in HMOs demonstrated significantly greater survival. In addition to earlier detection, however, other survival advantages appear to be associated with HMO enrollment, including screening use and differences in treatment patterns. Studies have found that among earlier stage breast cancer patients requiring surgery, HMO enrollees were significantly more likely to receive radiation therapy. 29,30 Age may also affect treatment choices, as a higher use of breast-conserving surgery and radiation therapy has been found among elderly women with early stage breast cancer. 9 Both cancer stage at diagnosis and treatment patterns may cause differences in mortality; therefore, possible differences in cancer survival among healthcare delivery systems should be evaluated as well. Systems within HMOs (such as the use of case managers) may have a role in the improved survival noted. 31,32
Limitations
The current study has several limitations. It may be possible that, in general, healthier patients are enrolled in HMO plans; however, comorbid conditions were not available for evaluation in this study. 2,27 We did not study regional variation, but others have found that a difference in the managed care market share had limited effect on care for cancer patients. 33
By definition, the study population was ≥65 years of age, and it is not clear if the results are generalizable to a younger patient population. 2 Furthermore, the SEER data do not constitute a probability sample of the nation despite being the primary source of national information on cancer incidence and survival. 2,18 SEER areas are mostly urban and are concentrated in western states within the United States, with an oversampling of Hispanics and African Americans. Health plans and patients from these SEER areas may not be representative of the nation as a whole. Additionally, performance among individual or types of HMOs may vary. 30,34 Despite controlling for potential confounders, differences in the overall health of patients enrolled in the various healthcare systems might exist. 30,34 We also were not able to measure smoking or dietary factors that may affect patient outcomes, 2,18 and although we attempted to adjust for differences in socioeconomic data, there were limitations in using information related to in which Census tract a person resided. 2 Lastly, we used previous cancer diagnoses as a proxy for healthcare services participation; our preference would have been to use actual healthcare services data, which was not available.
The principal finding of significantly improved survival after diagnosis with breast cancer, especially after controlling for potential confounding factors, in patients enrolled in HMOs compared with FFS patients warrants further evaluation.
Footnotes
Disclosure Statement
The authors have no conflicts of interest to report.