
Abstract
This article reviews the applications of robotic surgery in gynecology and presents a summary of the early studies that have been performed regarding its use for hysterectomy, myomectomy, reproductive surgery, pelvic floor reconstruction, and gynecological cancer staging. Despite significant advances in conventional laparoscopic techniques, the majority of gynecological procedures are still performed through major abdominal incisions, which are associated with higher surgical morbidity. This article addresses the potential that robotic surgery may have in converting more gynecological operations to a minimally invasive approach.
Introduction
Minimally invasive surgical techniques have revolutionized the approach to management of such conditions as gallbladder disease, appendicitis, and female sterilization. Despite the widespread availability of standard laparoscopic equipment and training, however, the vast majority of routine and advanced gynecological surgeries are still being performed through major abdominal incisions. In a recent study evaluating whether teaching hospitals in Illinois were more likely to perform abdominal compared with nonabdominal hysterectomies (vaginal and laparoscopic), 82% vs. 77% in nonteaching hospitals were performed abdominally. Laparoscopic hysterectomy, even after adjusting for confounders, was associated with fewer complications than either the vaginal or open group. 1 In addition to a reduction in surgical morbidity, studies have clearly shown that laparoscopic surgery allows faster recovery time, reduced inpatient hospitalization, improved cosmesis, decreased blood loss, and less postoperative pain. 2
Why, then, does that rate of abdominal hysterectomy remain so high? Massive uterine fibroids that are not amenable to any approach other than a large incision certainly account for some of the procedures, but other technical barriers likely make up the majority. The learning curve for standard advanced laparoscopy is steep and long, particularly with regard to suturing and intracorporeal knot tying. Conventional laparoscopic instruments that have limited mobility, counterintuitive hand movements, ergonomic difficulty, and amplification of hand tremor present significant technical challenges that the majority of practicing gynecologists seemingly cannot overcome. 3
The introduction of robotic technology may present the tool that can level the playing field between expert and nonexpert laparoscopists and facilitate the transition of more gynecological procedures from an open to a minimally invasive approach without compromising outcomes or surgical morbidity. Robotic instruments have the unique feature of articulating wrists with distal ends that mimic the intricate movements of the human hand, thereby greatly facilitating complex tasks, such as suturing and knot tying. In addition to instruments that work in a similar manner to those one would use during open surgery, the surgical console affords a three-dimensional, magnified view of the operative field in which the surgeon has control over the camera and up to three instruments. This article reviews the applications of robotic surgery in gynecology and discusses the pros and cons of this technological advance.
Evolution of Robotics in Medicine
The evolution of robotics in medicine started with a simple voice-recognition system called HERMES, where camera movement, light source, insufflation, table movement, and patient table positioning were activated by voice control. The U.S. Food and Drug Administration (FDA) approved the first surgical robot, AESOP, in 1994, wherein a single robotic arm controlled the camera, thereby allowing the surgeon to use both hands to operate. By 1999, two arms had been added to create the Zeus surgical system, and the model of a master-slave platform was introduced, where the surgeon sat at a master surgical console and directed the slave robotic instruments. 4 This represented a major paradigm shift, moving the surgeon away from the bedside to a remote console, a theme that would be reproduced with future devices because it presents the unique opportunity to perform remote or telesurgery. Indeed, it was with the Zeus surgical system in 2001 that the first telesurgery was performed, where surgeons in New York successfully performed a laparoscopic cholecystectomy in Strasbourg, France. 5
The da Vinci surgical platform (Intuitive Surgical, Inc., Sunnyvale, CA) is currently the only FDA-approved robotic surgical system, as Intuitive Surgical acquired the manufacturers of the Zeus system and phased it out of production. The da Vinci surgical platform was initially approved for general use in 2000 and for gynecological surgery in 2005. The da Vinci system consists of three components: the surgeon console, which contains large microcomputer motherboards that direct the movements of the robotic arms (Fig. 1); the InSite vision system; and the patient-side cart with EndoWrist instruments and either three or four robotic arms (Fig. 2). The surgeon sits comfortably at the remote console and visualizes the three-dimensional operative field through a stereoscopic viewer while simultaneously maneuvering foot and hand controls. Foot pedals that are seated at the base of the console allow control of the camera, clutching between instruments, repositioning of the surgeon's hands in space, and use of monopolar and bipolar electrocautery. The surgeon's thumb and index fingers are placed through Velcro straps, where each movement that is made in a 360-degree space is reproduced by the instruments in the abdomen (Fig. 3). The patient-side cart has to be docked to special robotic trocars that are inserted into the abdomen at the beginning of the case just as in standard laparoscopy. Once docked, a myriad of different instruments can be introduced through the robotic arms, including scissors, needle drivers, and bowel retractors, affording the surgeon the opportunity to replicate the exact procedure laparoscopically that would have been performed through a major incision.

Surgeon console (© Intuitive Surgical, Inc.).
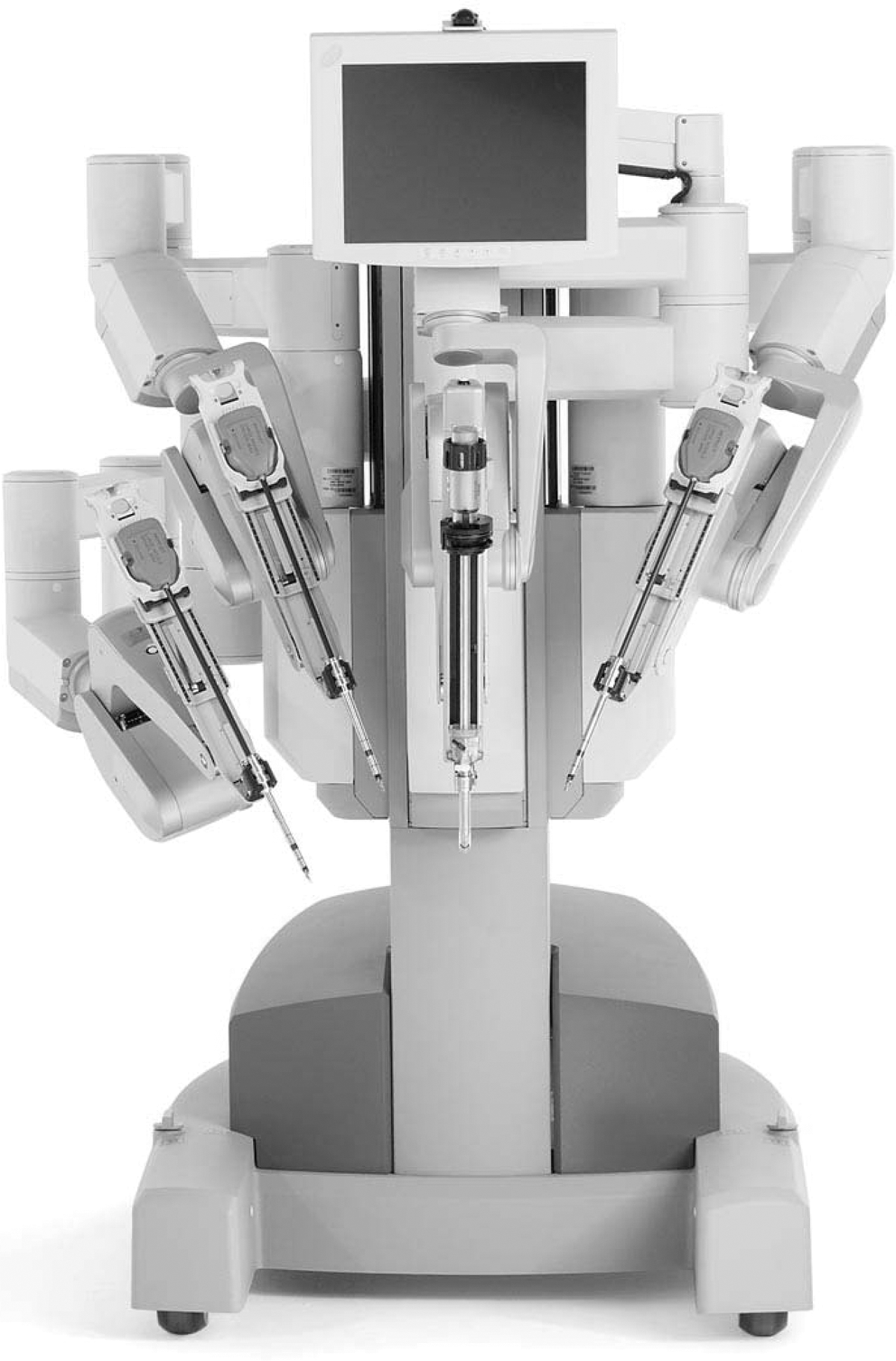
Patient-side cart with four robotic arms (© 2009 Intuitive Surgical, Inc.).

Surgeon's hands in Velcro straps at console.
Hysterectomy
An evaluation of hysterectomy rates in the United States in 2003 reported that of 538,722 hysterectomies performed for benign disease, 66% were performed abdominally, 21.8% vaginally, and 11.8% laparoscopically. The mean length of stay was significantly shorter in the nonabdominal group. 6 Although a major abdominal incision might seem advantageous from a surgeon's perspective, with depth perception and tactile feedback from tissue, the patient suffers the disadvantages of increased pain, longer recovery times, increased blood loss, and wound infection. 2 With rising rates of obesity, the dramatic morbidity associated with wound complications presents an urgent incentive to minimize the use of major abdominal incisions.
Robotics has been viewed as a possible technology to dramatically advance the trend toward a minimally invasive approach for hysterectomy. Reynolds and Advincula 7 were the first to report outcomes on 16 women who underwent total robotic hysterectomy. There were no conversions to laparotomy, and an advantage was reported in 13 of 16 women who had previously undergone surgery and had scarred surgical planes. 7 Several case series of women undergoing robotic hysterectomy have subsequently been published, the most recent of which is by Boggess et al., 8 who reported on 152 women undergoing robotic hysterectomy for benign cases with complex pathology. The overall operative time was 122.9 minutes, the mean estimated blood loss was 79 mL, and there were no conversions to laparotomy. There were 5 patients with postoperative complications and a mean length of hospital stay of 1 day. Of the characteristics indicating complexity, only uterine weight >250 g resulted in a significantly longer operative time. Lenihan et al. 9 reported a series of 100 benign robotic hysterectomies and found that total operative time sequentially stabilized at approximately 95 minutes after 50 cases, suggesting that the impact of a learning curve is significant in a surgeon's early experience with the technology. 9
Comparative studies between robotic and conventional laparoscopic hysterectomy are limited to a report of 200 consecutive cases completed before and after the implementation of a robotics program by Payne and Dauterive. 10 The rate of conversion to laparotomy was twice that in the prerobotic cohort, and mean blood loss was also significantly lower in the robotic group. The incidence of adverse events was similar in each cohort. 10 Robotic hysterectomy may offer no significant advantage to expert laparoscopists and may not demonstrate a significantly improved morbidity profile, but if it allows more surgeons to complete a hysterectomy without making a major abdominal incision, the patient may enjoy the benefits of a minimally invasive approach.
Reproductive Surgery
Myomectomy and tubal anastomosis present perfect robotic surgical opportunities, given the challenges they pose to conventional laparoscopic equipment and techniques. Myomectomy, the removal of isolated uterine fibroids in an attempt to preserve fertility, can cause a substantial defect in the uterine wall that requires expert suturing to achieve hemostasis and restore enough strength in the uterine wall to minimize the risk of uterine rupture in a subsequent pregnancy. Even expert laparoscopists can be challenged by this task. Although two prospective trials have shown postoperative morbidity to be less and recovery faster with laparoscopic myomectomy, the majority are still performed open for the reasons noted. 11,12
Advincula et al. 13 reported on the first series of robotic-assisted laparoscopic myomectomy in 35 women with removal of a mean of 1.6 myomas with a diameter of 7.9 cm. No transfusions were required and the conversion to laparotomy was 8.6%. A subsequent retrospective comparative study of 29 robotic with 29 open myomectomies found significantly reduced blood loss and length of stay in the robot cohort. Although operative time was longer in the robotic group, complications were fewer. 14 Given the recent adoption of robotics for this application, no data currently exist about the impact on subsequent pregnancy outcomes.
Tubal anastomosis requires visualization of a very small diameter lumen and precise suturing with fine-gauge material, both qualities that might benefit from the magnification capabilities of the robotic platform. Two comparative studies of tubal reversal using robotic assistance vs. traditional open microsurgery found longer operative times but shorter hospitalization time and recovery in the robotic cohort, with equal tubal patency and postprocedure pregnancy rates. 15,16 Hopefully as more reproductive surgeons gain exposure to robotic technology, additional data on pregnancy outcomes will be collected.
Reconstructive Pelvic Surgery
Because the prevalence of pelvic organ prolapse increases with age, the changing demographics of the world's population will result in a growing number of affected women. The gold standard surgical approach to the management of uterine or vaginal vault prolapse is the abdominal sacrocolpopexy, which has a high long-term success rate of 93%–99% but has traditionally been performed through a laparotomy incision because of the extensive suturing required. 17 In this procedure, the bladder and rectum are dissected off the apex of the vagina to facilitate the placement of a y-shaped mesh that is then attached to the sacral promontory to provide a tension-free suspending strap. Vaginal reconstructive surgical options, such as uterosacral and sacrospinous ligament suspensions and vaginally placed mesh procedures, are alternative treatments but have different effectiveness levels and are associated with different complications. 18 The recent introduction of the da Vinci robot in urogynecology has facilitated the transition of colposacropexy from an abdominal to a minimally invasive approach.
The studies that have evaluated the success of the robotic-assisted sacrocolpopexy have been limited in sample size and mean time of follow-up. The largest comparative study included 178 patients (73 robotic and 105 abdominal), with a follow-up of only 6 weeks postsurgery. 19 Anatomic outcomes were not significantly different. The robotic approach was associated with less blood loss (103 ± 96 mL vs. 255 ± 155 mL, p < 0.001), longer total operative time (328 ± 55 minutes vs. 225 ± 61 minutes, p < 0.001), shorter length of stay (1.3 ± 0.8 days vs. 2.7 ± 1.4 days, p < 0.001), and a higher incidence of postoperative fever (4.1% vs. 0%, p = 0.04). Another study followed patients for a minimum of 12 months but included only 21 patients. 20 All published studies to date have found that robotic sacrocolpopexy is successful in the treatment of pelvic organ prolapse, with a decreased hospital stay, low complication rate, and low morbidity. Each study, however, concluded that more long-term data are required to prove this procedure to be a durable repair. 19,21
An additional application in urogynecology is the management of complex fistula within the genitourinary tract. We recently performed a robotic fistula repair on a woman who developed a vesicocervical fistula after cesarean section. The meticulous dissection and suturing that was required to complete this operation laparoscopically was greatly afforded by the robot, and the patient had an uneventful recovery. Several case reports of vesicovaginal fistula repair exist in the urological literature. 22
Oncology
Gynecological oncology probably presents the optimal forum for application of robotics, given the complexity of surgical steps involved in performing radical hysterectomies for cervical cancer and lymph node sampling for endometrial cancer. Fanning et al. 23 reported the first series of robotic radical hysterectomy on 20 women with stage IB–IIA cervical carcinoma. Median operative time was 6.5 hours, and median blood loss was 300 mL. No complications were encountered, and all patients were discharged home on the first postoperative day. A retrospective cohort study of robotic vs. open radical hysterectomy found that the mean blood loss was significantly lower for the robotic group (81.9 vs. 665 mL, p < 0.0001), but operative time was longer (4.5 vs. 3.39 hours, p = 0.0002). The mean number of lymph nodes resected did not differ, and no complications were reported in the robotic-assisted group. 24 In a comparative study of laparotomy, standard laparoscopy, and robotic technique for hysterectomy and staging for endometrial cancer, Boggess et al. 25 reported a higher lymph node yield, shorter hospital stay, and lower estimated blood loss in the robotic cohort. Additionally, postoperative complications were significantly lower in the robotic group compared to the open group (5.9% vs. 29.7%, p < 0.001).
A multi-insitutional experience with robotic-assisted hysterectomy with staging for endometrial cancer was recently published. Between 2003 and 2009, 405 patients were identified who underwent robotic surgery for endometrial cancer. The conversion rate to laparotomy was 6.7%, and intraoperative and postoperative complications were low. For the group, <10 cases were required to achieve proficiency with the procedure, and the authors concluded that robotic technology seemed to level the playing field between the novice and expert laparoscopist for endometrial cancer staging. 26 These data present an opportunity for a significant paradigm shift in the surgical treatment of a disease that typically occurs in obese, postmenopausal women, who are most at risk for significant wound complications from an open approach.
Advantages and Disadvantages
Although the opportunity exists for a radical change in surgical approach for most gynecological procedures with the technological advances of robotics, coupled with the potential for remote telesurgery, several disadvantages exist as well. The principal surgical limitation is absence of haptic, or tactile, feedback. Learning as a surgeon to rely principally on visual cues takes practice and sometimes presents the limiting factor in being able to complete a case laparoscopically. The second disadvantage, which is far more difficult to overcome, is cost, which remains in the forefront of challenging issues in implementing robotics into gynecological practice. Each robotics system retails for approximately $1.6 million, is associated with annual maintenance contracts, and requires instruments that retail for approximately $2000 each and have ten limited uses. Laparoscopic and robotic procedures are combined into one current procedural terminology (CPT) code, with no opportunity for higher reimbursement for the more expensive technology. In addition, longer operating times translate into significantly higher operating room and anesthesia costs.
Conclusions
The introduction of robotic technology to the field of gynecology could have a dramatic impact on the conversion of the majority of procedures performed within the specialty from an open to a laparoscopic approach. The evolving literature on the subject suggests that limitations of conventional laparoscopy can be overcome and the skill level of the surgeon may be enhanced without detrimentally affecting outcomes. In fact, with increased exposure to robotic surgery, morbidity may decrease below levels seen for conventional laparoscopy. Women being evaluated for myomectomy, hysterectomy, tubal reanastomosis, pelvic floor reconstruction, and cancer surgery should be aware that the possibility may exist for a minimally invasive approach and that robotic technology may assist in more procedures being performed without making a major abdominal incision. Longer-term studies regarding cost, outcomes, and associated surgical risk are necessary.
Footnotes
Disclosure Statement
The author has no conflicts of interest to report.